

Abstract
Objectives:
To investigate whether intravascular ultrasound (IVUS) guided percutaneous coronary intervention (PCI) could improve clinical outcomes compared with angiography-guided PCI in the treatment of unprotected left main coronary artery stenosis (ULMCA) in the elderly.
Methods:
This controlled study was carried out between October 2009 and September 2012, in Qinhuangdao First Hospital, Hebei Province, China. One hundred and twenty-three consecutive patients with ULMCA, aged 70 or older, were randomized to an IVUS-guided group and a control group. The occurrence of major adverse cardiac events (MACE): death, non-fatal myocardial infarction, or target lesion revascularizations) were recorded after 2 years of follow-up.
Results:
The IVUS-guided group had a lower rate of 2-year MACE than the control group (13.1% versus 29.3%, p=0.031). The incidence of target lesion revascularization was lower in the IVUS-guided group than in the control group (9.1% versus 24%, p=0.045). However, there were no differences in death and myocardial infarction in the 2 groups. On Cox proportional hazard analysis, distal lesion was the independent predictor of MACE (hazard ratio [HR]: 1.99, confidence interval [CI]: 1.129-2.367; p=0.043); IVUS guidance was independent factor of survival free of MACE (HR: 0.414, CI: 0.129-0.867; p=0.033).
Conclusion:
The use of IVUS could reduce MACE in elderly patients undergoing ULMCA intervention.
Intravascular ultrasound (IVUS) may help to evaluate the target lesion and ensure adequate stent expansion during percutaneous intervention. A meta-analysis1 reviewed 5 studies and showed that there were no difference in death, non-fatal myocardial infarction (MI), and major adverse cardiac events (MACE) between IVUS-guided percutaneous coronary intervention (PCI) and angiography-guided PCI using bare-metal stents, other studies,2-5 showed that IVUS use could reduce adverse clinical events compared with angiography guidance. Intravascular ultrasound use may have more benefit in left main (LM) PCI using drug-eluting stent. A recently published study5 demonstrated that survival free of MACE at 3 years was higher in the IVUS group, and the incidence of stent thrombosis was lower in the IVUS group. However, the recent studies did not focus on the elderly, which are a sector of the population that is increasing in China. The elderly patients with unprotected left main coronary artery (ULMCA) generally have multi vessel disease and several risk factors. Due to the influence of culture and faith, these patients would choose PCI rather than coronary artery bypass graft in China. Does IVUS provide clinical benefit for these elderly patients? There are no controlled randomized trials to answer this question. Thus, the purpose of the present study is to investigate whether the IVUS-guided PCI is superior to the angiography-guided PCI during the long-term clinical follow-up in the elderly patients with ULMCA.
Methods
Study population
Between October 2009 and September 2012, in Qinhuangdao First hospital, Hebei Province, China, 123 consecutive elderly patients (age >70) with ULMCA were randomized to the IVUS group (61 patients) or the control group (62 patients). Patients in the IVUS group underwent intervention with IVUS guidance and patients in the control group underwent intervention with routine angiography guidance. Unprotected left main coronary artery was defined5 as at least 50% stenosis by visual assessment in the LM vessel without bypass grafts to the left anterior descending artery or left circumflex artery. Exclusion criteria were severe left ventricular dysfunction (ejection fraction <30%), cardiogenic shock, acute myocardial infarction, carcinoma.
This study was approved by the ethics committee of Qinhuangdao First Hospital, and a written informed consent was obtained from all patients prior to the procedure. This study was performed according to the principles of the Helsinki Declaration.
Procedure
Coronary angiography and PCI were performed in the 2 groups via a transradial or transfemoral approach. Minimal lumen diameter (MLD) and lesion length were measured with the quantitative coronary angiography (QCA) analysis system (Centricity CA1000, GE Healthcare, Waukesha, WI, USA).
In the control group, the intervention strategy was decided based on the location of the lesion. Single stent technology was used in ostium or trunk LM disease without bifurcation lesions. Lesions involving the distal segment of the LM or bifurcation were treated with T-stenting, provisional T-stenting or the kissing-balloon technique. In the IVUS group, the stenting technology was decided based on both angiographic finding and IVUS finding.
Two types of drug eluting stent (DES) were implanted as follows: 1) Sirolimus-eluting stents (Firebird-2, Microport, Shanghai, China). 2) Sirolimus-eluting stents (Excel, Jiwei, Shandong, China). Patients were loaded with 300 mg clopidogrel before procedure and remained on a 75 mg dosage daily for at least one year. Aspirin was administered 300 mg daily during the first month and 100 mg daily after the first month. Procedural success was defined as lumen stenosis <30% by final coronary angiography.
Intravascular ultrasound
Intravascular ultrasound was performed in patients of the IVUS group. After the intracoronary administration of 200 ug nitroglycerin, the IVUS catheter (Eagle Eye; Volcano Corporation, Rancho Cordova, CA, USA) was positioned at more than 10 mm beyond the lesion and was pulled back automatically (0.5 mm/s) to the opening of LM. Intravascular ultrasound images were examined by 2 experienced technicians using computerized planimetry (EchoPlaque, INDEC Systems, Inc., Mountain View, CA, USA). Minimal lumen diameter, minimal lumen area (MLA), reference lumen area, and plaque burden were measured. The cross-sectional luminal area was defined6 as the integrated area central to the intimal leading edge echo. Plaque burden6 was calculated as (EEM CSA-lumen CSA)/EEM CSA.
After the procedure, IVUS was repeated to ensure adequate stent expansion. The expansion ratio6 was calculated as minimum stent CSA / (proximal reference lumen CSA + distal reference lumen CSA) × 1/2. Successful stent expansion7 was defined as lumen area 90% or greater of the average reference lumen area pre-intervention. Patients with stent underexpansion underwent post-dilation to gain adequate stent expansion.
Follow-up
Clinical follow-up was performed at one month, 6 months, 12 months, and 24 months. Mean follow-up time was 23.26±7.24 months. Angiography follow-up was performed 9-12 months after the procedure. The primary endpoint was the 2-year incidence of MACE. It was defined as death, non-fatal myocardial infarction, and target lesion revascularization (TLR). Target lesion revascularization8 was defined as a new intervention (percutaneous or surgical) on a previously implanted stent, or within 5 mm of that stent. Deaths were classified as either cardiac or non-cardiac. Deaths that could not be classified were considered cardiac according to the Academic Research Consortium definitions.8 Myocardial infarction9 was diagnosed by an elevation of serum creatine kinase or troponin 3 times the upper limit of normal, together with chest pain lasting more than 30 minutes.
The safety endpoint was stent thrombosis. It was defined as definite or probable stent thrombosis according to established criteria.9 All data relating to procedures and in-hospital outcomes were collected. Information regarding clinical status were collected at clinic visits and by telephone interview.
Statistics analysis
All statistics analyses were performed using the Statistical Package for Social Sciences version 17 (SPSS Inc., Chicago, IL, USA). Continuous variables were expressed as mean ± standard deviation of the mean, and were compared by use of the unpaired t test; categorical variables were compared with the χ2 statistics or Fisher exact test.
The incidence rates of 2 year MACE were estimated by the Kaplan-Meier method. A probability value <0.05 was considered statistically significant. A Cox proportional hazard regression analyses were performed to find the predictors of the event outcomes. Variables with a probability value <0.20 in univariable analyses were candidates for the multivariable Cox proportional hazard regression models. A backward elimination process was used to develop the final multivariable model, and adjusted hazard ratio (HR) with 95% confidence intervals (CI) was calculated. A probability value <0.05 was considered statistically significant.
Results
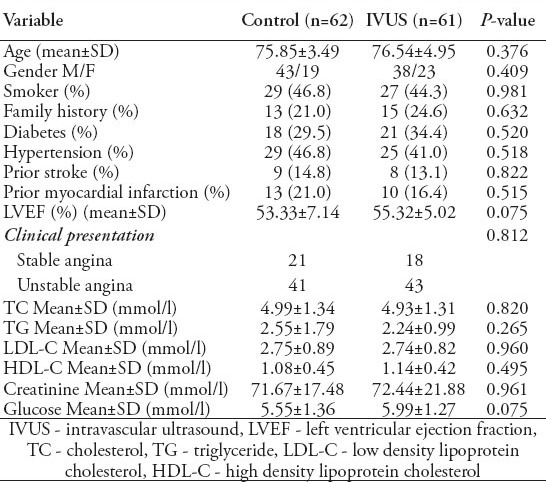
A total of 123 patients with ULMCA underwent IVUS-guided PCI (n=61) or angiography guided PCI (n=62). Baseline clinical characteristics were shown in Table 1. Both groups were balanced in age, gender, family history, diabetes mellitus, hypertension, smoking, prior stroke, and clinical presentation. There were no significant differences in laboratory characteristics such as left ventricular ejection fraction (LVEF), cholesterol, triglyceride, low, and high density lipoprotein cholesterol.
Table 1.
Clinical characteristics of the IVUS-guided and control group in elderly patients with unprotected left main coronary artery.
The angiographic and procedural characteristics are shown in Table 2. The procedural success was 100% in both groups. There was no death or acute stent thrombosis in the hospital. Coronary lesion complexity was similar in the both groups. More than half of the patients received single stent instead of 2 stent strategy in both groups, but the rate of post-dilation was higher in the IVUS group than in the control group (p=0.039).
Table 2.
Angiographic and procedural characteristics of the IVUS-guided and control group in elderly patients with unprotected left main coronary artery.
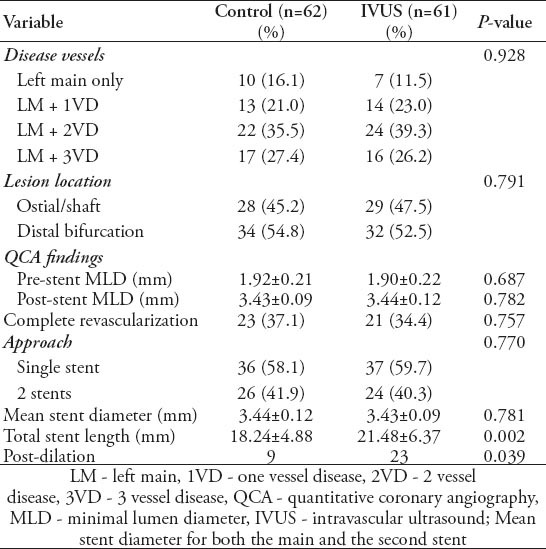
The QCA analysis revealed that pre-stent and post-stent MLD were similar in both groups. Final thrombolysis in MI flow grade 3 was achieved in almost all lesions (95.3%). Stent diameter had no difference between the 2 groups, but the IVUS guidance patients had longer stents than the control patients. Intravascular ultrasound showed that 23 patients had stent under expansion (37.7%). In patients with single stent, the most common site of under expansion was left anterior descending ostium (12 cases, 32.4%), but in patients with double stents, left circumflex ostium was the most common site of under expansion (11 cases, 45.8%).
Intravascular ultrasound characteristics are shown in Table 3. Follow-up coronary angiography was carried out in 63.9% of the patients in the control group and in 65.5% of the patients in the IVUS-guided group. There was no statistical difference in the restenosis rate between the IVUS-guided and the control group, but a trend toward less restenosis remained in favor of the IVUS-guided group (3.28 versus 8.15%; p=0.11). Clinical follow-up was at least 2 years (mean 23.26±7.24 months). In Table 4, the overall MACE rate was lower in the IVUS-guided group than in the control group (12.8% versus 27.3% p=0.049). Aso Kaplan-meier analysis revealed (Figure 1), the IVUS guidance patients had higher MACE-free survival rate. The IVUS guidance patients had a lower rate of TLR than the control patients, but there were no difference in death, and non-fatal MI between the 2 groups (p>0.05). Occurrence of stent thrombosis was similar in the 2 groups (1.6% in the IVUS-guided group versus 3.2% in the control group p=0.568).
Table 3.
Intravascular ultrasound (IVUS) characteristics of IVUS-guided elderly patients with unprotected left main coronary artery.
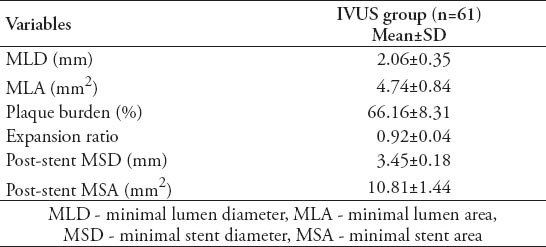
Table 4.
Clinical outcomes (24 months) of IVUS-guided and control group in elderly patients with unprotected left main coronary artery.

Figure 1.

Kaplan-Meier curves illustrating freedom from major adverse cardiac events (MACE) in intravascular ultrasound (IVUS) and control groups over 24 months (p=0.031).
On multivariate Cox regression analysis, age, stent diameter, stent length, lesion location, IVUS use, and diabetes were entered into the multivariate Cox regression analysis. As shown in Table 5, distal bifurcation was the independent predictor of MACE; IVUS guidance was a factor of freedom from MACE.
Table 5.
Predictors of major adverse cardiac events in elderly patients with unprotected left main coronary artery undergoing left main stenting.

Discussion
The main finding of this study was that IVUS guidance could decrease the incidence of adverse events in elderly patients undergoing ULMCA intervention.
We found that the IVUS-guided patients had lower MACE rates. This beneficial result was mainly driven by the decreased rate of TLR. But the IVUS guidance could not reduce mortality and myocardial infarction. As we know, IVUS may confirm the presence of significant LM disease and guide selection of stent size. Also IVUS helps us to detect PCI complications including the presence of edge dissection, stent under expansion, as well as the need for post-dilatation. Some studies,5,10,11 both in the bare metal stent (BMS) era and in the DES era, found that IVUS guidance could reduce the risk of major adverse cardiac events in patients with ULMCA. In a meta-analysis of 2972 patients,10 IVUS-guided BMS implantation showed a reduced risk of binary restenosis, repeat revascularization and MACE, without significant benefits in death or myocardial infarction. In the MAIN-COMPARE study,4 975 patients with ULMCA underwent PCI under the guidance of IVUS or angiography alone. In 201 matched pairs, there was a tendency of lower risk of 3-year morality with IVUS guidance compared with angiography guidance. In particular, patients receiving DES had significantly lower mortality rates with IVUS guidance, but IVUS guidance did not reduce mortality rate in patients receiving BMS. However, these studies were not focused on the elderly, who represent a large portion of admitted patients with ULMCA. Although some studies12-13 demonstrated that LM stenting was safe in the elderly, there is still no randomized trial to compare IVUS guidance and angiography guidance in these patients. The current study demonstrated that IVUS use was safe in the elderly, and it was an independent predictor for freedom from MACE. Intravascular ultrasound was beneficial in the elderly with ULMCA.
In this study, angiography follow-up revealed that the IVUS guidance patients group had tendency toward lower restenosis rate than the angiography guidance patients. It is known that stent under expansion is the most important mechanical cause leading to DES restenosis. Patients without stent under expansion had higher MACE-free survival rates. In this study, IVUS findings showed that 23 patients had stent under expansion. For these patients, post-dilation was performed to gain adequate stent expansion. Our findings suggest that the IVUS guidance may have a trend to decrease restenosis in ULMCA intervention.
This study has several limitations. First, it was a single-center study, the sample size was small. We could not perform a sub-group analysis to investigate whether diabetes or bifurcation lesions influence the beneficial results of IVUS. Second, pre-procedure and post-procedure of LCX pullback were not checked in most single stent cases, so we did not gain IVUS imaging of LCX in these patients. Third, patients with myocardial infarction were excluded, comprising a large portion of ULMCA in the real world.
In conclusion, IVUS use during ULMCA intervention with DES may improve clinical outcomes in the elderly.
Footnotes
References
- 1.Lodi-Junqueira L, de Sousa MR, da Paixão LC, Kelles SM, Amaral CF, Ribeiro AL. Does intravascular ultrasound provide clinical benefits for percutaneous coronary intervention with bare-metal stent implantation?A meta-analysis of randomized controlled trials. Syst Rev. 2012;1:42. doi: 10.1186/2046-4053-1-42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Jang JS, Song YJ, Kang W, Jin HY, Seo JS, Yang TH, et al. Intravascular ultrasound-guided implantation of drug-eluting stents to improve outcome: a meta-analysis. JACC Cardiovasc Interv. 2014;7:233–243. doi: 10.1016/j.jcin.2013.09.013. [DOI] [PubMed] [Google Scholar]
- 3.Kang SJ, Ahn JM, Song H, Kim WJ, Lee JY, Park DW, et al. Comprehensive intravascular ultrasound assessment of stent area and its impact on restenosis and adverse cardiac events in 403 patients with unprotected left main disease. Circ Cardiovasc Interv. 2011;4:562–569. doi: 10.1161/CIRCINTERVENTIONS.111.964643. [DOI] [PubMed] [Google Scholar]
- 4.Park SJ, Kim YH, Park DW, Lee SW, Kim WJ, Suh J, et al. Impact of intravascular ultrasound guidance on long-term mortality in stenting for unprotected left main coronary artery stenosis. Circ Cardiovasc Interv. 2009;2:167–177. doi: 10.1161/CIRCINTERVENTIONS.108.799494. [DOI] [PubMed] [Google Scholar]
- 5.Anterola F, Garcia Camarero T, Gimeno de Carlos F, et al. Clinical impact of intravascular ultrasound guidance in drug-eluting stent implantation for unprotected left main coronary disease: pooled analysis at the patient-level of 4 registries. JACC Cardiovasc Interv. 2014;7:244–254. doi: 10.1016/j.jcin.2013.09.014. [DOI] [PubMed] [Google Scholar]
- 6.Kim JH, Jeong MH, Hong YJ, Lee KH, Kim IS, Choi YH, et al. Low density lipoprotein-cholesterol/high density lipoprotein-cholesterol ratio predicts plaque vulnerability in patients with stable angina. Korean Circ J. 2012;42:246–251. doi: 10.4070/kcj.2012.42.4.246. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Roy P, Steinberg DH, Sushinsky SJ, Okabe T, Pinto Slottow TL, Kaneshige K, et al. The potential clinical utility of intravascular ultrasound guidance in patients undergoing percutaneous coronary intervention with drug-eluting stents. Eur Heart J. 2008;29:1851–1857. doi: 10.1093/eurheartj/ehn249. [DOI] [PubMed] [Google Scholar]
- 8.Wu X, Chen Y, Kubo T, Ge C, Ren F, Wu X, et al. Long-term (4-year) outcomes and predictors of adverse cardiac events after sirolimus-eluting stent implantation in unprotected left main coronary artery. Int Heart J. 2010;51:377–382. doi: 10.1536/ihj.51.377. [DOI] [PubMed] [Google Scholar]
- 9.Kappetein AP, Head SJ, Généreux P, Piazza N, van Mieghem NM, Blackstone EH, et al. Updated standardized endpoint definitions for transcatheter aortic valve implantation: the Valve Academic Research Consortium-2 consensus document. J Am Coll Cardiol. 2012;60:1438–1454. doi: 10.1016/j.jacc.2012.09.001. [DOI] [PubMed] [Google Scholar]
- 10.Parise H, Maehara A, Stone GW, Leon MB, Mintz GS. Meta-analysis of randomized studies comparing intravascular ultrasound versus angiographic guidance of percutaneous coronary intervention in pre-drug-eluting stent era. Am J Cardiol. 2011;107:374–382. doi: 10.1016/j.amjcard.2010.09.030. [DOI] [PubMed] [Google Scholar]
- 11.Gao XF, Kan J, Zhang YJ, Zhang JJ, Tian NL, Ye F, et al. Comparison of one-year clinical outcomes between intravascular ultrasound-guided versus angiography-guided implantation of drug-eluting stents for left main lesions: a single-center analysis of a 1,016-patient cohort. Patient Prefer Adherence. 2014;8:1299–1309. doi: 10.2147/PPA.S65768. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Wang Q, Tan Q, Liu D, Yang H, Ma L. Clinical outcomes of transradial unprotected left main coronary artery stenting in the elderly. Saudi Med J. 2014;35:838–842. [PubMed] [Google Scholar]
- 13.Sheridan BC, Stearns SC, Rossi JS, D’Arcy LP, Federspiel JJ, Carey TS. Three-year outcomes of multivessel revascularization in very elderly acute coronary syndrome patients. Ann Thorac Surg. 2010;89:1889–1894. doi: 10.1016/j.athoracsur.2010.03.003. discussion 1894-1895. [DOI] [PMC free article] [PubMed] [Google Scholar]