

Abstract
In spite of significant disparities in sexual health outcomes for American Indian youth, no studies exist examining the effectiveness of HIV-prevention interventions. Circle of Life is an HIV-prevention intervention specifically developed for American Indian middle-school youth. We describe the rationale, methodology, and baseline results of a longitudinal randomized trial of Circle of Life conducted among American Indian youth aged 11–15 in a reservation community. The innovative design includes two pre-intervention waves to determine patterns of behavior prior to the intervention that might be associated with a differential impact of the intervention on sexual risk. We used one-way analysis of variance and chi-square tests to test for significant differences between randomized group assignment at each baseline wave and generalized estimating equations (GEE) to test significant differences in the rate of change in outcomes by group longitudinally. We present the collaborative and adaptive strategies for consenting, assenting, and data collection methodology in this community. Achieved response rates are comparable to other similar studies. Results from the two baseline waves indicate that few outcomes significantly varied by randomized intervention assignment. Ten percent of youth reported having had sex at Wave 1, rising to 15% at Wave 2. Among those who had had sex, the majority (>70%) reported using a condom at last sex. The project is well positioned to carry out the longitudinal assessments of the intervention to determine the overall impact of the Circle of Life and the differential impact by pre-intervention patterns of behavior across youth.
Keywords: Intervention, HIV/AIDS, American Indian, Youth, Prevention
Introduction and Background
HIV prevention among youth, especially minority youth, has been a national health priority for a number of years (National Institutes of Health 2007). Results from intervention studies strongly suggest that HIV-prevention interventions can improve health and behavior outcomes, especially if they are theory-based, convey a specific and consistent message to a well-defined target group, and provide skill-building for behavior change (Coyle et al. 2004; Kirby et al. 2004; Robin et al. 2004). Further, culturally appropriate interventions have been shown to be effective among minorities (Herbst et al. 2007; Jemmott et al. 1999; Shain et al. 2004). Such findings hold tremendous promise for American Indian youth. Evidence indicates that American Indian youth begin having sex at an earlier age and have sex with more partners when compared to their counterparts at the national level (Hellerstedt et al. 2006; Kaufman et al. 2007a). American Indians have two to four times the rate of sexually transmitted diseases (STDs) compared to their White counterparts, a disparity sustained even at the youngest age groups (Centers for Disease Control and Prevention 2003). Among American Indians diagnosed with AIDS, 7% are youth under the age of 25, compared to 3.5% for the national population (Centers for Disease Control and Prevention 2006). To date, however, no HIV-prevention study has included sufficient numbers of American Indian youth to evaluate the effectiveness of such programs with this population, in spite of the apparent high risk for compromised sexual health.
Circle of Life (COL) is a culturally appropriate and theoretically based HIV-prevention curriculum designed specifically for American Indian middle-school children. This project was designed to evaluate the effectiveness of COL in school settings on an American Indian reservation. This behavioral intervention study included innovative features to accommodate important theoretical and methodological issues. This study also integrated extensive community participation throughout development and implementation. In particular, the design included two initial data points with which to assess pre-intervention risk pathways that may enhance or diminish the effects of the intervention. As important as the innovative design was the role of the American Indian community in this longitudinal behavioral intervention; the success of the project was predicated on community support and participation.
Here we present the design and implementation of this project, and the results from the first two waves of baseline data. In total, the project consists of eight waves completed in the Spring of 2009. The current paper discusses preliminary findings of pre-intervention risk pathways (based on the first two waves), the specific community context of an American Indian reservation in which this intervention research was implemented, and establishes the basis upon which the assessment of this intervention’s effectiveness will proceed.
Study Setting
The project was conducted on a Northern Plains American Indian reservation. Because community confidentiality is often as important as individual confidentiality for many Native communities (Norton and Manson 1996), we do not use the name of the tribe here, but the general descriptor of Northern Plains Tribe (NPT). The NPT is one of the poorest of the federally recognized tribes: Median income in 1999 was less than $28,000, compared to $42,000 for the nation, and more than 30% aged 25 and older did not have a high-school diploma, compared to less than 20% of the US total population (U.S. Census Bureau 2000). Yet it also has a long history of cultural independence and activism (Ostler 2004; Viola 1999), with strong cultural, community, and familial ties. The reservation land can be characterized as very rural with an extremely low population density and large distances between villages.
This reservation was located in the Aberdeen Indian Health Service (IHS) region, which experienced the highest case rates of chlamydia and gonorrhea of all IHS areas—six and three times, respectively, the national level—with those under 20 comprising 50% of all cases reported (Wong et al. 2006). While rates of HIV or AIDS are not calculated by IHS service area, American Indians in the state in which this tribe is located comprised 16% of HIV/AIDS cases in 2007, even though they were only 9% of the population (South Dakota Department of Health 2008). Of note, the risk environment for American Indian youth is often characterized by substance use and emotional stress, which are frequently co-factors in early sexual experience and unsafe sexual practices (Kaufman et al. 2004; Novins et al. 2001).
Interest in an HIV-prevention intervention for youth was high among tribal members in initial discussions. Prior work with this community suggested a high level of awareness of challenges youth face in sexual risk-taking and avoidance, and an openness to addressing those challenges (Kaufman et al. 2007b). We attribute this openness to the accomplishments of community health organizers actively raising awareness, and to the holistic approach of this community to health, including sexual health. Indeed, as a part of the grant application, we received letters of support for the project from all 13 middle schools on the reservation, the local health coordinating group, and the tribal health board administrator. Once funding had been secured, we obtained tribal and University IRB approvals. We also formed a community advisory committee that has served in a consultative and community liaison capacity.
Intervention
Circle of Life (COL) is a 30-hour HIV/AIDS and STD prevention and health education curriculum especially designed for middle-school American Indian children (Orbis Associates 2002). The curriculum was developed by Orbis Associates, an American Indian-controlled, not-for-profit education organization, with support of the BIA Office of Education and the Centers for Disease Control and Prevention-Division of Adolescent and School Health. Based on earlier research in HIV-prevention education (Schinke et al. 1990), COL was designed as a targeted health curriculum for HIV and STD prevention with an emphasis on skills-building and role-playing. Consistent with American Indian philosophies, however, it encompassed far more than sexual-risk prevention—it promoted the development of overall wellness of students. COL embodied the theory and concepts of Social Cognitive Theory (Bandura 1997; Bandura et al. 2003) using the medicine wheel—a cultural symbol of a circle divided into four equal parts, encompassing spiritual, emotional, physical, and mental wellness as the four essential aspects of health and well-being. (See Fig. 1.) As developed within the curriculum, all four parts of this “Circle of Life” touch each other and shape volition (expectancies) located at the center of the circle, with balance among the elements of the circle providing the foundation for making healthy decisions and acting on them. COL provided a conceptual guide for American Indian students, using familiar symbols that explicitly linked behavior with knowledge, ways of thinking, and expectations about acquired skills and ideas. COL included both cognitive and affective learning, with a heavy emphasis on skills-training and practice. Symbols, stories, and ways of learning familiar to American Indian youth provided the foundation for classroom implementation. It benefited from extensive advisory and consultative processes with American Indian communities and education specialists (Orbis Associates 2002).
Fig. 1.
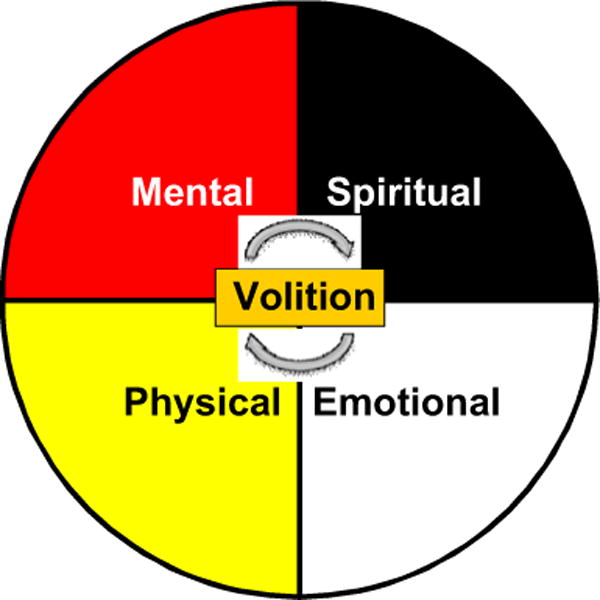
Circle of Life medicine wheel
Target Population
The project consisted of two target populations: (1) youth attending middle schools on the NPT reservation, and (2) their primary caretakers. In this study, middle-school youth were defined as those attending 6th or 7th grade at Wave 1 (W1). Using total enrollment data from the 13 schools, we estimated 768 students comprised the total target population. The population is highly mobile, characterized by youth moving on and off the reservation as well as frequent moves within reservation borders. Moreover, youth do not always move with natal families but often spent time with different relatives or family friends, depending on family and kin resources, needs, or season. For example, some natal families do not have the means to support a child, sometimes children are sent to care for grandparents or other relatives, or sometimes children are sent to live with someone for the school year because of proximity to a preferred school. Some children board at schools during the week (or sometimes longer) because of the long distances involved. Finally, a small but important subset of middle-school youth is characterized by withdrawal from school or dropping out for varying periods of time.
Primary caretakers were defined as the adult aged 18 years or older who was most responsible for the care and well-being of the child. This person may have been different from the legal guardian of the child, since some children live with relatives other than their legal guardian. Thus, both legal guardians and main caretakers had to be identified for appropriate consent and data collection procedures (described below).
Study Design
The project employed a wait-listed group-randomized intervention design. A wait-listed design provides that all respondents receive the intervention within a certain timeframe but that one randomly selected group receives it sometime after the other group, so that intervention and control comparisons can be made in the interim (Campbell and Stanley 1963). This design feature is particularly appealing to many Native communities. For an intervention targeting a high-priority problem, placebo-control designs are often viewed unfavorably since approximately half of all participants do not receive the intervention. In our case, schools agreed to the wait-listed randomization design only if it could be administered to all schools within 12 months. We thus randomly assigned all 13 reservation schools to one of two groups. To minimize confusion over “control” and “experimental” schools—since all schools eventually received the intervention—we refer to randomly assigned schools as COL1 (receiving the intervention in year 1) and COL2 (receiving the intervention in year 2) schools. The interventions were administered in the Fall of subsequent years to minimize seasonality.
Two Pre-intervention Observation Points
A randomized control design includes, at a minimum, a randomization of subjects or groups to control and experimental conditions, a baseline measure, an intervention administered to the experimental group, and a post-test measure to test difference in outcomes between conditions. Frequently, for adolescent research, the “right-hand” side of the design is extended; that is, observations are collected for an extended period of time to measure the long-term effects of an intervention. This has been a particularly important feature of behavioral research with adolescents. Trajectories of youth development may vary considerably over short periods of time and the longevity of the intervention effects may dissipate quickly. In contrast, few have considered the “left-hand” side of the trajectory: By the baseline, youth may have already developed patterns of behaviors that may set them on a particular path through adolescence. In a randomized design comparing control to experimental groups, these prior histories are, in theory, “randomized” away. That is, since subjects are assigned at random to different conditions, history is assumed to no longer affect the control-intervention comparison of outcomes. However, for those who receive the intervention, we do not know how prior patterns of behavior may shape the impact of the intervention (Raudenbush 2001a, b). Consider several hypothetical examples, illustrated in Fig. 2. One group of youth may begin with a low-risk profile, but quickly move to high-risk activities. The intervention may not completely stop the trend, but may slow the advance to high-risk activity. Or, another group of youth may show moderate levels of risk with little change in that profile across the first two waves of observation. With COL, this group may reduce their levels of risk, at least at first. The longitudinal design will allow us to evaluate the need for a booster session if the trajectory of risk again begins to increase at later waves. As demonstrated in this schematic, a design with only one baseline measure would have shown three hypothetical groups of youth to be at the same starting point. Yet response to the intervention can vary according to pre-intervention patterns. To capture such patterns of change and the subsequent effect an intervention may have on these groups of youth, we included two data pretest collection points prior to the intervention in either group—one 6 months before the beginning of the intervention (W1) and one just prior to intervention (W2)—to differentiate possible preexisting patterns in development.
Fig. 2.
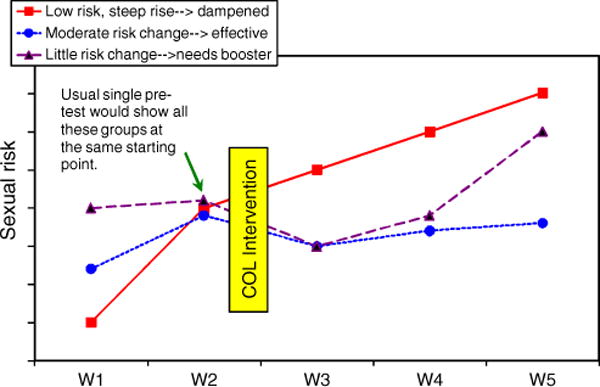
Schematic of potential intervention effects, by pre-intervention paths
Overall Design of Study
The pre-intervention points were integrated within the larger framework of a random group intervention, with follow-up every 4 to 6 months across 18 months for a total of three follow-up data points. The wait-listed design within that time period maintained a 12-month window of observation to compare results of control schools (COL2) and intervention schools (COL1), including two observation points. This wait-listed intervention design provides all schools the opportunity to receive the intervention within a year—a critical requirement from the community’s perspective. It also provided the opportunity to increase the number of students who received the intervention to assess the differential impact of the intervention. Thus, the data collection schedule had two different measurement conceptualizations, depending on whether the analysis question was the effect of the intervention compared to “treatment as usual” (COL1 v. COL2), or the differential effects of the intervention by various subgroups (COL1 + COL2). (See Tables 1 and 2.)
Table 1.
Circle of Life planned research design, pre-post test evaluation

|
O Observation; X intervention
COL1 data collection noted with small bracketed letters, COL2 with numbers.
Smaller black box indicates treatment v. “treatment as usual” effect comparisons, shaded areas indicate observations for assessment of pre-intervention patterns on intervention effect. See Table 2.
W4 recruiting 6th graders for differential impact analysis, COL2 schools only
W7 and W8 collected only for COL2 to obtain their 18-month period of observation; W6 is 18-month endpoint for COL1
Table 2.
Circle of Life planned research design, differential impact evaluation

|
O Observation; X intervention
Differential effects sample denoted by combination of COL1+ COL2 observations, e.g., [small letter + number] data collection event as assigned in Table 1
Finally, early observations of COL2 schools, used for the COL1 v. COL2 comparison (points [1[ and [2] in Table 1], can be used in combination with the other COL2 baseline observation (points [3] and [4] in Table 1) to more fully investigate pre-intervention trajectories.
Of note, we included two additional components of the study. Main caretakers of youth participants were surveyed once to provide additional information about the home and community environment of youth. An additional goal of the project was to develop guidelines for the NPT community on the use or “best practices” of the implementation of COL. To do this, we conducted focus groups with students, teachers, and parents directly after the conclusion of COL in classes. The attendant activities and analyses of these study components have been ongoing. Here we focused primarily on the process and outcomes attendant to youth data collection of the two baselines, and outcomes.
Sample Size
We used Monte Carlo simulations in MPlus (Muthen and Muthen 2002) to calculate sample size requirements for analyses using both conceptualizations of measurement: COL1 v. COL2 for intervention effectiveness, and COL1 + COL2 for differential impact of intervention by subgroups. Results from these simulations suggested that we would have sufficient power (80% or more) to conduct both types of analyses if we had between 400 and 535 youth participants.
Our next step was to develop a plan to achieve this sample size within the NPT. We had few examples of intervention research of this magnitude with American Indian youth with which to estimate participation. Many earlier studies of American Indian youth were small. Other studies used passive consent procedures, whereby parents had to notify the school or researcher if they did not want their children to participate in a study. Such efforts were not able to inform our project. Studies with American Indian youth that have included active parent consent tended to provide little information on sample frame or response rate at either parent or child levels or used the consented population as the denominator to determine response rate for subsequent data collection waves (similar to clinical trials; Caballero et al. 2003; Stiffman et al. 2005). Further, although prior community input suggested a high level of acceptability of COL for youth, we had no information about parent/guardian consent rate for child participation in this sensitive study. Prior community-based research with American Indian adults in similar settings indicated that locating randomly selected individuals was often time- and resource-consuming in these highly mobile and geographically dispersed populations (Beals et al. 2003). For the project, this implied that finding specific parents or guardians might be challenging.
To be as cautious as possible, we did not sample from the population but included all youth attending middle schools on the NPT. So, for example, with an estimated total population of 768 6th- and 7th-grade students, and assuming 15–25% of parents could not be contacted and another 15–25% would refuse to allow their child’s participation or the child would not want to participate, we would still have sufficient power for analyses (N between 540 and 420).
Sample Recruitment
Recruitment of the sample required a number of steps, including school recruitment and participation agreement, parent or guardian consent, student assent, and caretaker consent. We had an established field office in the NPT, staffed by community members well experienced in community relations and extensively trained in human subjects confidentiality and consenting or assenting procedures.
Schools
The Tribe indicated that each school was autonomous and had its own right to participate or not in the project. We thus developed a Memorandum of Understanding (MOU) between the University and each school, delineating specific agreements including class scheduling, school confidentiality, and data sharing. Every school decided to make the COL class mandatory—even if a student did not have guardian consent to participate in the surveys (i.e., research portion) for the project, all students had to attend the class.
Adult and Youth Recruitment
Schools provided students rosters in early Fall, 2005. We sent project materials, including the parent—guardian consents and contact information for any questions, home with students. We tested this school-based approach with one medium-sized school. Return rates were quite low, under 30% in 10 days, and many of the returned documents were not completed correctly. Moreover, although the vast majority of adults in this population spoke English as a first language, many had difficulty reading and understanding the consent. We decided that parent-guardian consent would be personally administered by trained project staff to ensure comprehension and accuracy. Our goal, then, was to identify and meet with the parent or guardian of each youth so that staff could explain the project, review the consent form, and answer any questions.
A number of challenges arose: Some schools would not provide home contact information to project personnel. For those students for whom we had information, addresses were frequently post office box addresses and phone numbers often were not operational. We used several strategies to establish contact with parents or guardians, all with prior approval of the University IRB and local authorities: We organized community meetings or dinners, using local media to invite parents or guardians of middle-school children to participate; we sent letters home with students asking parents to contact us to set up a meeting; and we attended events that were frequented by parents, such as sporting events or parent-teacher meetings. We also tried a “giveaway” — a culturally common event like a raffle. If parents contacted our offices about the project, their names and their children’s names were entered into a drawing for a prize. Entry into the giveaway drawing was based on speaking with a staff member, not on consent or refusal of the parent.
Consent and Assent
Parent/guardian consent was administered by trained project staff, most of whom were community members. Each staff member confirmed guardianship of the child and explained the purpose of the project, the duration of project, the maximum number of times each child would be surveyed, and the compensation for each survey the child completed ($10 money order or the equivalent). Additionally, staff described the content of the survey questions including sexual activity and substance use; our protection of the confidentiality of each child; and our obligation to report to authorities youth disclosures of events or threats of harm to self or to others or of sexual abuse including statutory rape. If the parent or guardian consented, the staff member verified the most regular caretaker of the child. In most cases, these two were the same person. A staff member asked the caretaker if he or she would like to participate in the caretaker component of the study. If so, the staff member explained the consent for the adult survey and its purpose. If the caretaker consented, he or she was given a self-administered survey, which took about 45 minutes to complete. Caretakers could return the survey at any time in self-sealed envelopes or ask that a staff member pick it up. Caretakers were given a $20 money order for their time.
During youth data collection, each child for whom we obtained parent/guardian consent was asked to give assent. Project staff verbally explained the project to the youth: Participation was voluntary, they could withdraw any time, and they could refuse to answer any question. Staff also explained situations that had to be reported to the authorities, including disclosure of intent to harm self or others and of sexual abuse, including statutory rape. Only assenting youths were provided a self-administered survey, to be completed in class at a scheduled time. To accommodate varying reading levels, each student had the option of having a staff member read survey questions to him or her individually. Each student was paid a $10 money order or equivalent upon return of a survey in a self-sealing envelope. All students with parental consent were given the opportunity to provide or withdraw assent at each wave. Youth surveys also required about 45 minutes to complete.
Sample Definition
We developed a definition of study population to accommodate the high mobility of youth and the inevitable inconsistencies between school roster information and actual class attendance. We compiled a master list of students, including names from rosters and names from the consenting process (since not all youth eligible to participate appeared on a school roster), noting consent status. This list allowed us to verify quickly consent status of all participants. To maximize participation of eligible youth with parent consent, we defined as our sample any student who participated in at least one wave of data collection through the wave immediately following the second implementation of the intervention (W6). Although this will likely result in several missing data points for some participants, it provided a concrete response to community concerns about including mobile youth. Further, recent developments in imputation provide a means for maximizing the known data to estimate missing data (Croy and Novins 2005; Royston 2004). Indeed, using this definition of participating respondent, we will be able to investigate the methodological and substantive consequences of limited participation in longitudinal school-based studies for youth. It is this mobile population that may be at greatest risk and most likely to benefit from such an intervention.
Study Measures
Study measures were developed from a variety of sources, including established psychosocial measures; measures of ethnicity and cultural identity; parental and peer relationships; alcohol and drug use items; and measures of knowledge, attitudes, and expectancies about sex and HIV/AIDS/STDs. All items were reviewed by community members and adapted if appropriate. Several measures were suggested by community members and added to the survey. Measures were piloted in a culturally similar but geographically distinct tribal community. Psychometric analyses of pilot data provided a means for assessing reliability of scales, as well as problematic questions or skip patterns. We provide a summary of selected psychosocial measures, item examples, and alphas for W1 and W2 data collection for youth in Table 3. The alphas indicate a reasonable level of reliability. The self-esteem measure was lowest for both waves. Self-efficacy for refusing sex and outcome expectancy in W1 were also low. This may have been a function of the young age of the respondents. Behavioral outcomes were based on questions from Youth Risk Behavior Surveys (Grunbaum et al. 2004), AddHealth surveys (Harris et al. 2003), Panel Study of Income Dynamics. Child Development Supplement. Available at:www.psidonline.isr.umich.edu/CDS. Accessed July 21, 2004, and items developed with community members.
Table 3.
Psycho-social scales
| Scale* | Number of items | example | Response set | Cronbach’s alpha
|
|
|---|---|---|---|---|---|
| Wave 1 | Wave 2 | ||||
| Cultural identification (Phinney, 1992) | 5 | “Being a part of my tribe or cultural group is important to me.” | 4-pt response from strongly disagree to strongly agree | 0.73 | 0.79 |
| Self-esteem (not modified) (Rosenberg, 1965) | 6 | “I have a positive attitude.” | 4-pt response from strongly disagree to strongly agree | 0.66 | 0.71 |
| Self-efficacy: Sex avoidance (Cecil & Pinkerton, 2000) | 4 | “I stay away from people who are pressuring me to have sex.” | 4-pt scale, from not at all sure I would do this to completely sure I would do this | 0.81 | 0.83 |
| Self-efficacy: Resisting sex (Cecil & Pinkerton, 2000) | 4 | “What would you say to having any kind of sex with someone you wanted to go out with again?” | 4-pt scale, from “I’d definitely say ‘no’” to “I’d definitely say ‘yes’” | 0.70 | 0.75 |
| Outcome expectancy: Sex refusal (Rotheram-Borus et al., 1998) | 5 | “If I didn’t have sex, my friends would think there is something wrong with me.” | 4-pt scale, from strongly agree to strongly disagree. | 0.68 | 0.74 |
| Self-efficacy: Condom use (Dilorio et al., 1997) | 5 | “If neither of us had a condom, we would get one before we had sex.” | 4-pt scale, from “not at all sure I would do this” to “completely sure I would do this” | 0.81 | 0.80 |
| Self-efficacy: Obtaining condoms (Baele, et al., 2001) | 4 | “I know where to get condoms.” | 4-pt scale, from “not sure I would do this” to “completely sure I’d do this” | 0.76 | 0.76 |
| Outcome expectancies: Condom use (Albarracin et al., 2000) | 4 | “Using a condom would protect me and my partner from getting STDs (for example, herpes). | 4-pt scale, from “strongly disagree” to “strongly agree” | 0.73 | 0.77 |
All scales reviewed by community and subsequently modified when necessary
Data Collection and Sample Disposition at Baseline
Originally, we estimated 3 months for the parent/guardian consent process. However, we had only been able to contact about 50% of parents or guardians in that timeframe. We thus extended the recruitment period another 4 months and delayed the intervention by one school term. Data collection for W1 began in Spring, 2006. W2 was completed in Fall, 2006, prior to the implementation of the intervention. Subsequent waves were scheduled for 4 to 6 month intervals thereafter, for completion in Spring of 2009. In W1, we identified a total of 846 students attending 6th and 7th grades in participating schools — about 100 more than appeared on the original rosters we were provided—and 100 new parents or guardians to seek out for consent quickly. This exemplifies the incongruity between rosters and actual class attendance, often related to high mobility. We adapted youth tracking procedures to account for this. Results for youth participation in the project are presented in Table 4.
Table 4.
Response rates for Circle of Life, W1 & W2
| W1 | W2 | |
|---|---|---|
| Total class population | 846 | 866 |
| Number of parents/guardians (PG) contacted | 641 | 698 |
| % PG contacted/total class | 76 | 81 |
| % PG gave consent/total class | 74 | 79 |
| % PG gave consent/contacted | 98 | 98 |
| Consented eligible youtha | 617 | 628 |
| % consented eligible youth surveyed | 90 | 86 |
| Overall response rate | ||
| % youth surveyed × % parent consented of total eligible | 67 | 68 |
| % youth surveyed × % parent consented of contacted | 88 | 84 |
Some youth who had parental consent to participate were subsequently found to be ineligible (e.g. out of age range, transferred to off-reservation school etc)
We were able to contact 76% of all parents or guardians by W1. By W2, we contacted a total of 81%. Of those contacted, 98% consented to their child’s participation, yielding a pool of 617 and 628 youth eligible to complete surveys in W1 and W2, respectively. Ninety percent of eligible youth completed surveys in W1, and 86% completed them in W2. Overall, combining parent/guardian consent rate and youth response rate, 67% (W1) and 68% (W2) of the total classroom population participated in the project.
Hypotheses and Statistical Methods for Baseline Data
We had two hypotheses with respect to the baseline integrity of the study design.
Youth participants will not differ significantly on demographic or sexual risk indicators by COL1 or COL2 status at pre-test points W1 or W2.
The slope of the change in sexual risk outcomes between the pre-test points W1 and W2 will not significantly differ by COL1 and COL2 status.
Our first goal was to determine the comparability of youth of COL1 and COL2 at both baselines (intercepts). The second goal was to determine the comparability of youth of COL1 and COL2 schools by changes between the two baselines (if any). In the first case, we were concerned with cross-sectional differences: Are students in COL1 schools significantly different from students in COL2 schools on key outcomes at W1? And then at W2? We used simple one-way analysis of variance and chi-square tests in SPSS v. 16 (SPSS) to determine significant difference across COL school status.
The second goal required statistical methods able to accommodate the longitudinal character of the sample (slopes): If any changes occurred across waves for key outcome variables, was the change systematically related to enrollment in a COL1 or COL2 school? For example, we might expect that the probability of youth ever having sex increased between W1 and W2 because increasing numbers of teens, even young ones, are likely to have sex over time. It is not the change over time for these two baseline waves that we wanted to measure to test the second hypothesis. Instead, we wanted to measure if that increased probability of having sex was different according to whether students attended COL1 or COL2 schools. We used the panel data commands of Stata, v10 (Stata 2006) to estimate longitudinal models across the two school groups. We used regression or logit techniques as indicated by the type of outcome variable. We estimated population-averaged models since we were interested in outcomes changes of youth in COL1 or COL2 schools as two groups, not as individuals. This is equivalent to a generalized estimating equation (GEE) to allow for correlated observations. For both cross-sectional and longitudinal analyses, we did not account for clustering by schools. Since we were anticipating no or few significant differences, this was a conservative approach. Without accounting for the randomized group design, standard errors are likely to be underestimated and significance likely to be overestimated. In the interest of simplicity, we refrained from school-specific adjustments. Note that we applied the longitudinal analyses to the outcome variables only. Cross-sectional information is provided for compositional description of the two waves by COL1 and COL2.
Results
We present baseline W1 and W2 background and demographic results in Table 5.
Table 5.
Sample demographic description by COL1 and COL2, by Wave
| Outcome variable (%) | W1 (cross-sectional)
|
W2 (cross-sectional)
|
|||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| N | Overall | COL1 | COL2 | p-value | N | Overall | COL1 | COL2 | p-value | ||
| Youth characteristic: | |||||||||||
| Gender (%) | female | 268 | 48.6 | 51.5 | 45.2 | 255 | 47.1 | 51.7 | 42.7 | ||
| male | 284 | 51.4 | 48.5 | 54.8 | 0.137 | 286 | 52.9 | 48.3 | 57.3 | 0.036 | |
| Age (%) | 11–12 | 274 | 50.4 | 50.2 | 50.6 | 143 | 26.6 | 28.6 | 24.5 | ||
| 13–15 | 270 | 49.6 | 49.8 | 49.4 | 0.925 | 396 | 73.5 | 71.4 | 75.5 | 0.289 | |
| Grades in school (mean, A=4.0; F=0.0) | 533 | 2.8 | 2.8 | 2.9 | 0.104 | 518 | 2.9 | 2.9 | 3.0 | 0.785 | |
| Household composition: | |||||||||||
| Number of adults in HH (mean) | 338 | 3.0 | 3.0 | 3.0 | 0.954 | 375 | 3.1 | 3.2 | 3.0 | 0.617 | |
| Number of children (mean) | 371 | 3.9 | 4.0 | 3.8 | 0.528 | 380 | 3.9 | 4.1 | 3.8 | 0.183 | |
| Household economic characteristic | |||||||||||
| Often no money for food (%) | 479 | 6.90 | 6.10 | 7.90 | 0.427 | 467 | 7.9 | 5.4 | 10.5 | 0.042 | |
| Often no money for heat (%) | 481 | 6.00 | 5.30 | 7.00 | 0.432 | 467 | 6.0 | 5.4 | 6.6 | 0.588 | |
| Often no money for electricity (%) | 481 | 8.90 | 7.50 | 10.70 | 0.224 | 470 | 6.0 | 5.8 | 6.1 | 0.871 | |
| Life outside of school: | |||||||||||
| # of sports, other activities (mean) | 441 | 2.5 | 2.4 | 2.6 | 0.492 | 408 | 2.0 | 1.9 | 2.1 | 0.463 | |
| Work for pay, last 12 months (%) | 506 | 33.8 | 32.0 | 35.9 | 0.352 | 483 | 35.2 | 33.2 | 37.2 | 0.352 | |
| Watches TV 3+ hours/day (%) | 503 | 24.9 | 26.3 | 23.1 | 0.418 | 483 | 21.1 | 26.4 | 15.8 | 0.004 | |
| Computer games 3+ hours/day (%) | 503 | 17.1 | 19.3 | 14.4 | 0.143 | 481 | 17.5 | 19.0 | 15.9 | 0.369 | |
| Combined screen time 5+ hrs/day | 500 | 25.4 | 26.5 | 24.1 | 0.548 | 480 | 23.1 | 27.4 | 18.8 | 0.026 | |
| Cultural life (% strongly agree): | |||||||||||
| Important to be part of tribe | 535 | 51.0 | 45.9 | 56.7 | 0.026 | 514 | 50.8 | 50.6 | 51.0 | 0.888 | |
| Speak or learning language | 530 | 26.6 | 24.2 | 29.3 | 0.018 | 505 | 28.3 | 25.1 | 31.5 | 0.040 | |
| Feels good re cultural background | 533 | 59.1 | 55.9 | 62.7 | 0.069 | 513 | 51.1 | 51.6 | 51.5 | 0.913 | |
Bold=p>.05
Two of 16 background and demographic characteristics were found to be significantly different across COL1 and COL2 in W1, and 5 of 16 in W2. In W1, COL2 included more youth endorsing positively two of the 3 cultural life measures. In W2, COL2 included more boys and fewer girls compared to COL1. COL2 in W2 also included youth reporting higher levels of no money for food, lower levels of screen viewing time, and higher levels of speaking or learning the language. Overall, ages of participants were about evenly divided between 11-to-12 year-olds and 13-to-15 year-olds, and attained grades just below a “B.” Youth reported that they shared their homes with about six other people and, on average, between 6% and 8% reported their families often had no money for food, heat, or electricity. Youth in this project appeared to be active outside of school, reporting that they were involved in two to three activities, and about a third had worked for pay. However, about a quarter of the youth in this project reported they watched TV or played computer games for five or more hours on a school day. The majority of youth reported that they strongly agreed that being a part of the tribe was important and felt good about their culture.
Sexual risk outcomes are presented in Table 6. We found few significant differences by randomized group (COL1 v. COL2, first two panels). In W1, we found no significant differences. In W2, 2 of 18 outcomes among all sexual risk measures were significantly different by COL1 and COL2, both of them related to alcohol use and first sex. No longitudinal differences were found for other sexual risk outcomes. That is, although increases or decreases across the waves may have occurred, COL1 and COL2 groups did not experience that change in a significantly different way from each other over time.
Table 6.
HIV/ADIS knowledge and sexual risk behavior by COL1 and COL2, by wave
| Outcome variable | W1 (cross-sectional) | W2 (cross-sectional) | Relationship between COL year and change in outcome between W1 & W2 (longitudinal) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
|
|
|
|||||||||||
| N | Overall | COL1 | COL2 | p-value | N | Overall | COL1 | COL2 | p-value | coeff | se | p-value | |
| Knowledge (% correct of 12) | 515 | 59.7 | 60.9 | 58.4 | 0.365 | 494 | 58.4 | 59.0 | 57.8 | 0.420 | −0.2006 | 0.153 | 0.191 |
| Ever had sex either gender (%) | 520 | 9.8 | 8.4 | 11.3 | 0.265 | 499 | 15.2 | 12.8 | 17.7 | 0.130 | 0.341 | 0.204 | 0.095 |
| Have had oral sex (%) | 446 | 2.2 | 2.1 | 2.4 | 0.818 | 453 | 5.3 | 4.3 | 6.3 | 0.359 | 0.426 | 0.370 | 0.249 |
| Have had vaginal sex (%) | 461 | 6.7 | 5.3 | 8.4 | 0.187 | 471 | 11.0 | 10.1 | 12.0 | 0.503 | 0.391 | 0.244 | 0.109 |
| Have had anal sex (%) | 446 | 2.9 | 2.5 | 2.7 | 0.774 | 445 | 2.2 | 3.1 | 1.4 | 0.224 | −0.401 | 0.459 | 0.382 |
| Below calculated only for those answering “Yes” to ever had sex | |||||||||||||
| Age of first sex (mean) | 47 | 12.0 | 11.6 | 12.3 | 0.104 | 73 | 12.9 | 12.7 | 13.0 | 0.650 | 0.429 | 0.385 | 0.265 |
| Age of first partner (mean) | 42 | 13.7 | 14.3 | 13.2 | 0.569 | 70 | 14.1 | 14.0 | 14.2 | 0.794 | −0.353 | 0.857 | 0.681 |
| Lifetime # partners >2 (%) | 44 | 25.0 | 28.6 | 21.7 | 0.732 | 66 | 27.3 | 31.0 | 24.3 | 0.544 | −0.088 | 0.298 | 0.767 |
| Had partner last 3 months (%) | 45 | 55.6 | 52.4 | 58.3 | 0.769 | 69 | 65.2 | 62.1 | 67.5 | 0.640 | 0.384 | 0.263 | 0.145 |
| Any sex last 12 mos (%) | 49 | 63.3 | 72.7 | 55.6 | 0.248 | 85 | 55.3 | 52.8 | 57.1 | 0.689 | −0.129 | 0.360 | 0.719 |
| Ever used condom (%) | 54 | 77.8 | 82.6 | 74.2 | 0.525 | 91 | 84.6 | 88.2 | 82.5 | 0.460 | −0.458 | 0.466 | 0.326 |
| Condom last sexual intercourse (%) | 43 | 83.7 | 88.9 | 80.0 | 0.680 | 86 | 70.9 | 71.4 | 70.6 | 0.933 | −0.181 | 0.416 | 0.664 |
| Ever been or caused pregnancy (%) | 50 | 4.0 | 0.0 | 7.1 | 0.497 | 90 | 2.2 | 2.9 | 1.8 | 1.000 | 0.748 | 1.167 | 0.521 |
| STD diagnosis (%) | 55 | 0.0 | 0.0 | 0.0 | – | 99 | 3.0 | 2.8 | 3.2 | 1.000 | 0.194 | 1.234 | 0.875 |
| Alcohol at first sex (%) | 48 | 18.8 | 18.2 | 19.2 | 1.000 | 89 | 19.1 | 30.6 | 11.3 | 0.023 | −0.7002 | 0.445 | 0.115 |
| Partner used alc/drugs at first sex (%) | 48 | 14.6 | 18.2 | 11.5 | 0.687 | 92 | 19.6 | 30.6 | 12.5 | 0.033 | −0.877 | 0.459 | 0.056 |
| Alc/drugs at last sex (%) | 49 | 22.4 | 26.1 | 19.2 | 0.734 | 90 | 21.1 | 25.0 | 18.5 | 0.460 | −0.3679 | 0.422 | 0.383 |
| Partner used alc/drugs at last sex (%) | 49 | 16.3 | 17.4 | 15.4 | 1.000 | 88 | 15.9 | 22.9 | 11.3 | 0.148 | −0.5444 | 0.476 | 0.252 |
Substantively, results are indicative of the need for effective interventions. Almost 10% had reported having had sex at W1, with vaginal sex by far the most common type of sex. In W2, about six months later, 15% had reported having sex and 5% reported having had oral sex, a 3% increase. Of those who had sex, about 25% reported having two or more partners, increasing to 27% in W2. Importantly, the vast majority of those who had had sex reported that they had used a condom at last sex, although the level declined by more than 10 points between W1 and W2.
Discussion
Overall, the results of the baseline analyses indicate that the project is well positioned to carry out analyses using the two conceptualizations of measurements: Intervention effectiveness and differential effect of the intervention. This innovative design provides a means to assess the benefits of an HIV-prevention intervention among youth of a Northern Plains tribe and to assess the differential impact of that intervention by pre-intervention patterns of behavior. The design was crafted to test the hypothesis that youth were likely to respond differently to the same intervention, depending on their own set of characteristics; on their pre-and post-intervention growth trajectories; and on the larger familial, peer, and community influences shaping those characteristics—all factors in the theoretical framework that will be used to assess the impact of the intervention.
The project is not without its limitations. First, we are working with only one tribal community. We will be unable to generalize our findings to other communities, although our approach is likely to provide a template for intervention in other settings. Although we spent extra time and a great deal of resources, we were unable to contact approximately 24% and 19% of parents in W1 and W2, respectively. These parents were likely to be those that worked in places requiring long-distance commutes or long hours, parents living in very remote or rural areas, those who were particularly uninvolved in their child’s school life, or parents who may have feared that abuse, neglect, or their own substance use patterns may come to light in the research process. However, our response rates were similar to those in other comparable studies (Ebreo et al. 2002; Kirby et al. 2004; O’Donnell et al. 2002; Tortolero et al. 2008). For example, Coyle and colleagues (2004), in a recent longitudinal study of a school-based sexual risk reduction intervention with ethnically diverse urban middle-school youth, reported 90% parent contact, 77% consent rate, and an overall youth response rate of 68%. Randomization at the group level when the outcome of interest is at the individual level has its known disadvantages (Murray 1998) yet is often the only practical solution for many settings, such as schools, when randomization at the individual level is not possible and resources are not sufficient for alternative designs (Bloom et al. 2007). Finally, outcomes relating substance use with first sex were significantly different across COL1 and COL2 schools in W2. This finding indicates that closer inspection of these measures in subsequent analyses will be necessary, even though no significant differences were found in the change across groups over time.
While the emphasis here was on methodology, important too were the substantive results that highlight both the great need of sexual risk addressed in this population, and the uniqueness of this project. This project is among the first in an American Indian setting to include specific measures of types of sexual activity for youth as young as 11 years old. These measures, when reviewed by schools, health organization leaders, and parents, produced lively and extended debate. Yet, all recognized that information about these key behaviors would be critical to address sexual risk—and attendant transmission of diseases—in this community. As in other settings, youth may be discounting the risk associated with this activity (Brewster and Harker Tillman 2008). For example, the results of this project indicated that for many, sexual activity began young, included diverse forms of sexual risk, and for 15 to 22%, involved alcohol or drugs. Notably, while measures of sexual risk pointed to challenges youth face—even very young adolescents—these results were equally clear that many were making healthy decisions and taking responsibility for their actions. In W2, for example, 85% have not had any kind of sex. Of those that had sex, 71% reported using a condom at last sex. Further analyses will provide insight into the trajectories of sexual risk, why those trajectories differ among youth, and how an intervention might make a difference.
In summary, we presented various innovative features of this prevention project and some compelling baseline results. While the design of this intervention project may include unique dimensions that will enable prevention evaluation in ways not previously possible, it is important to note that the project has been embedded in significant community collaboration and support. Without such cooperation and partnership, the project’s innovative potential would never have been realized.
Acknowledgments
We thank the schools and the tribal community for their ongoing support; parents, guardians, and youth who gave so generously of their time; and project staff who made it all happen. We acknowledge the support of the National Institute of Mental Health (R01 MH069086) and the Bureau of Indian Education, Division of Performance and Accountability.
References
- South Dakota Department of Health. South Dakota HIV/AIDS Surveillance Report, January 2008. 2008 Retrieved March 31 2008, from http://doh.SD.gov/Disease/Documents/January08.pdf.
- Albarracin D, McNatt PS, Williams WR, Hoxworth T, Zenilman J, Ho RM, et al. Structure of outcome beliefs in condom use. Health Psychology. 2000;19:458–468. doi: 10.1037//0278-6133.19.5.458. [DOI] [PubMed] [Google Scholar]
- Baele J, Dusseldorp E, Maes S. Condom use self-efficacy: Effect on intended and actual condom use in adolescents. Journal of Adolescent Health. 2001;28:421–431. doi: 10.1016/s1054-139x(00)00215-9. [DOI] [PubMed] [Google Scholar]
- Bandura A. Self-efficacy: The exercise of control. New York: W.H. Freeman and Company; 1997. [Google Scholar]
- Bandura A, Caprara GV, Barbaranelli C, Gerbina M, Pastorelli C. Role of affective self-regulatory efficacy in diverse spheres of psychosocial funtioning. Child Development. 2003;74:769–782. doi: 10.1111/1467-8624.00567. [DOI] [PubMed] [Google Scholar]
- Beals J, Manson SM, Mitchell CM, Spicer P, TAI-SUPERPFP Team Cultural specificity and comparison in psychiatric epidemiology: Walking the tightrope in American Indian research. Culture, Medicine and Psychiatry. 2003;27:259–289. doi: 10.1023/a:1025347130953. [DOI] [PubMed] [Google Scholar]
- Bloom HS, Richburg-Hayes L, Black AR. Using covariaties to improve precision for studies that randomize schools to evaluate educational interventions. Educational Evaluation and Policy Analysis. 2007;29:30–59. [Google Scholar]
- Brewster KL, Harker Tillman K. Who’s doing it? Patterns and predictors of youths’ oral sexual experiences. Journal of Adolescent Health. 2008;42:73–80. doi: 10.1016/j.jadohealth.2007.08.010. [DOI] [PubMed] [Google Scholar]
- Caballero B, Himes JH, Lohman T. Body composition and overweight prevalence in 1704 schoolchildren from 7 American Indian communities. American Journal of Clinical Nutrition. 2003;78:199–200. doi: 10.1093/ajcn/78.2.308. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Campbell DT, Stanley JC. Experimental and quasi-experimental designs for research. Chicago: Rand McNally; 1963. [Google Scholar]
- Cecil H, Pinkerton SD. Magnitude: An important dimension of self-efficacy. Journal of Applied Social Psychology. 2000;30:1243–1267. [Google Scholar]
- Centers for Disease Control and Prevention. Sexually transmitted disease and surveillance, 2002. Atlanta: U.S. Department of Health and Human Services; 2003. [Google Scholar]
- Centers for Disease Control and Prevention. Cases of HIV infection and AIDS in the United States, by race/ethnicity, 2000–2004. HIV/AIDS Surveillance Supplemental Report 2006. 2006;12:1–24. [Google Scholar]
- Coyle KK, Kirby DB, Marín BV, Gómez CA, Gregorich S. Draw the line/respect the line: A randomized trial of a middle school intervention to reduce sexual risk behaviors. American Journal of Public Health. 2004;94:843–851. doi: 10.2105/ajph.94.5.843. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Croy CD, Novins DK. Methods for addressing missing data in psychiatric and developmental research. Journal of the American Academy of Child & Adolescent Psychiatry. 2005;44:1230–1240. doi: 10.1097/01.chi.0000181044.06337.6f. [DOI] [PubMed] [Google Scholar]
- Dilorio C, Maibach E, O’Leary A, Sanderson CA, Celentano DD. Measurement of condom use self-efficacy and outcome expectancies in a geographically diverse group of STD patients. AIDS Education and Prevention. 1997;9:1–13. [PubMed] [Google Scholar]
- Ebreo A, Feist-Price S, Siewe Y, Zimmerman RS. Effects of peer education on the peer educators in a school-based HIV prevention program: Where should peer education research go from here? Health Education & Behavior. 2002;29:411–423. doi: 10.1177/109019810202900402. [DOI] [PubMed] [Google Scholar]
- Grunbaum JA, Kann L, Kinchen S. Youth Risk behavior surveillance–United States, 2003. Morbidity and Mortalitiy Weekly Report Surveillance Summary. 2004;53:1–96. [PubMed] [Google Scholar]
- Harris KM, Florey F, Tabor J, Bearman PS, Jones J, Udry JR. The National Longitudinal Study of Adolescent Health: Research design. 2003;2006 [Google Scholar]
- Hellerstedt WL, Peterson-Hickey M, Rhodes KL, Garwick A. Environmental, social, and personal correlates of having ever had sexual intercourse among American Indian youths. American Journal of Public Health. 2006;96:2228–2234. doi: 10.2105/AJPH.2004.053454. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Herbst JH, Kay LS, Passin WF, Lyles CM, Crepaz N, Marin BV. A systematic review and meta-analysis of behavioral interventions to reduce HIV risk behaviors of Hispanics in the United States and Puerto Rico. AIDS Behavior. 2007;11:25–47. doi: 10.1007/s10461-006-9151-1. [DOI] [PubMed] [Google Scholar]
- Jemmott JB, Jemmott LS, Fong GT, McCaffree K. Reducing HIV risk-associated sexual behavior among African American adolescents: Testing the generality of intervention effects. American Journal of Community Psychology. 1999;27:161–187. doi: 10.1007/BF02503158. [DOI] [PubMed] [Google Scholar]
- Kaufman CE, Beals J, Mitchell CM, LeMaster PL, Fickenscher A. Stress, trauma, and risky sexual behavior among American Indians in young adulthood. Culture, Health, and Sexuality. 2004;6:301–318. doi: 10.1080/13691050310001645032. [DOI] [PubMed] [Google Scholar]
- Kaufman CE, Desserich J, Big Crow CK, Holy Rock B, Keane E, Mitchell CM, et al. Culture, context, and sexual risk among Northern Plains American Indian youth. Social Science & Medicine. 2007a;64:2152–2164. doi: 10.1016/j.socscimed.2007.02.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kaufman CE, Shelby LK, Mosure D, Marrazzo JM, Wong D, de Ravello L, et al. Within the hidden epidemic: Sexually transmitted disease and HIV/AIDS among American Indians and Alaska Natives. Sexually Transmitted Diseases. 2007b;34:766–777. doi: 10.1097/01.olq.0000260915.64098.cb. [DOI] [PubMed] [Google Scholar]
- Kirby DB, Baumler E, Coyle KK, Basen-Engquist K, Parcel GS, Harrist R, et al. The “Safer Choices” intervention: It’s impact on the sexual behaviors of different subgroups of high school students. Journal of Adolescent Health. 2004;35:442–452. doi: 10.1016/j.jadohealth.2004.02.006. [DOI] [PubMed] [Google Scholar]
- Murray DM. Design and analysis of group-randomized trials. New York: Oxford University; 1998. [Google Scholar]
- Muthen LK, Muthen BO. How to use a Monte Carlo study to decide on sample size and determine power. Structural Equation Modeling. 2002;9:599–620. [Google Scholar]
- National Institutes of Health. Trans-NIH plan for HIV-related research. Office of AIDS Research, National Institutes of Health, U.S. Department of Health and Human Services; 2007. [Google Scholar]
- Norton IM, Manson SM. Research in American Indian and Alaska Native communities: Navigating the cultural universe of values and process. Journal of Consulting and Clinical Psychology. 1996;64:856–860. doi: 10.1037//0022-006x.64.5.856. [DOI] [PubMed] [Google Scholar]
- Novins DK, Beals J, Mitchell CM. Sequences of substance use among American Indian adolescents. Journal of the American Academy of Child & Adolescent Psychiatry. 2001;40:1168–1174. doi: 10.1097/00004583-200110000-00010. [DOI] [PubMed] [Google Scholar]
- O’Donnell L, Steueve A, O’Donnell C, Duran R, San Doval A, Wilson R, et al. Long-term reductions in sexual initiation and sexual activity among urban middle schoolers in the Reach for Health service learning program. Journal of Adolescent Health. 2002;31:93–100. doi: 10.1016/s1054-139x(01)00389-5. [DOI] [PubMed] [Google Scholar]
- Orbis Associates. Circle of Life HIV/AIDS and STD Prevention curriculum: Wellness education for American Indian and Alaska Native middle school students. Washington DC: Orbis Associates; 2002. [Google Scholar]
- Ostler J. The Plains Sioux and U.S colonialism from Lewis and Clark to Wounded Knee. Cambridge, UK: Cambridge University; 2004. [Google Scholar]
- Phinney JS. The multigroup ethnic identity measure: A new scale for use with diverse groups. Journal of Adolescent Research. 1992;7:156–176. [Google Scholar]
- Raudenbush SW. Comparing personal trajectories and drawing causal inferences from longitudinal data. Annual Review of Psychology. 2001a;52:501–525. doi: 10.1146/annurev.psych.52.1.501. [DOI] [PubMed] [Google Scholar]
- Raudenbush SW. Toward a coherent framework for comparing trajectories of individual change. In: Collins LM, Sayer AG, editors. New methods for the analysis of change. Washington, DC: American Psychological Association; 2001b. pp. 33–64. [Google Scholar]
- Robin L, Dittus R, Whitaker D, Crosby R, Ethier K, Mezoff J, et al. Behavioral interventions to reduce incidence of HIV, STD, and pregnancy among adolescents: A decade in review. Journal of Adolescent Health. 2004;24:3–26. doi: 10.1016/s1054-139x(03)00244-1. [DOI] [PubMed] [Google Scholar]
- Rosenberg M. Society and the adolescent self-image. Princeton, NJ: Princeton University; 1965. [Google Scholar]
- Rotheram-Borus MJ, Murphy DA, Fernandez MI, Srinivasan S. A brief HIV intervetnion for adolescents and young adults. American Journal of Orthopsychiatry. 1998;68:553–564. doi: 10.1037/h0080364. [DOI] [PubMed] [Google Scholar]
- Royston P. Multiple imputation of missing values. The Stata Journal. 2004;4:227–241. [Google Scholar]
- Schinke SP, Gordon AN, Weston RE. Self-instruction to prevent HIV infection among African-American and Hispanic-American adolescents. Journal of Consulting and Clinical Psychology. 1990;58:432–436. doi: 10.1037//0022-006x.58.4.432. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shain RN, Piper JM, Holden AEC, Champion JD, Perdue ST, Korte JE, et al. Prevention of gonorrhea and chlamydia through behavioral intervention: Results of a two-year controlled randomized trial in minority women. Sexually Transmitted Diseases. 2004;31:401–408. doi: 10.1097/01.olq.0000135301.97350.84. [DOI] [PubMed] [Google Scholar]
- Stata. Intercooled Stata for Windows (Version Special Edition 9.1,) College Station, TX: Stata Corporation; 2006. [Google Scholar]
- Stiffman AR, Freedenthal S, Brown E, Ostman E, Hibbeler P. Field research with underserved minorities: The ideal and the real. Journal of Urban Health. 2005;82:iii56–iii66. doi: 10.1093/jurban/jti064. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tortolero SR, Markham CM, Addy RC, Baumler ER, Escobar-Chavez SL, Basen-Engquist KM, et al. Safer Choices 2: Rationale, design issues, and baseline results in evaluating school-based health promotion for alternative school students. Contemporary Clinical Trials. 2008;29:70–82. doi: 10.1016/j.cct.2007.05.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- U.S. Census Bureau. Census 2000 summary files 1 2, 3 (SF1, SF2, SF3) 2000 Retrieved October 25, 2007, from http://www.census.gov/main/www/cen2000.html.
- Viola HJ. Little Bighorn remembered. New York: Random House; 1999. [Google Scholar]
- Wong D, Swint E, Paisano EL, Cheek JE. Indian health surveillance report-Sexually transmitted diseases, 2004. Atlanta, GA: US Department of Health and Human Services, Centers for Disease Control and Prevention and the Indian Health Service; 2006. [Google Scholar]