

Abstract
Hepatic artery thrombosis (HAT) is the most serious vascular complication after liver transplantation. Multiple risk factors have been identified to impact its development. Changes in haemostasis associated with end stage liver disease and the disturbance of the coagulation and anticoagulation cascades play an important role in development of this lethal complication. Early recognition and therapeutic intervention is mandatory to avoid its consequences. Pharmacological prophylaxis, by the use of antiplatelet or anticoagulant agents, is an important tool to reduce its incidence and prevent graft loss. Only a few studies have shown a clear benefit of antiplatelet agents in reducing HAT occurrence, however, these studies are limited by being retrospective and by inhomogeneous populations. The use of anticoagulants such as heparin is associated with an improvement in the outcomes mainly when used for a high-risk patients like living related liver recipients. The major concern when using these agents is the tendency to increase bleeding complications in a setting of already unstable haemostasis. Hence, monitoring of their administration and careful selection of patients to be treated are of great importance. Well-designed clinical studies are still needed to further explore their effects and to formulate proper protocols that can be implemented safely.
Keywords: Hepatic artery thrombosis, Haemostasis, Anticoagulation, Liver transplantation, Antiplatelets, Heparin
Core tip: Hepatic artery thrombosis (HAT) is the most serious vascular complication after liver transplantation. Changes in haemostasis associated with liver disease play a role in its development. Pharmacological prophylaxis may reduce its incidence and prevent graft loss. Few studies have shown a clear benefit of antiplatelets in reducing HAT occurrence, however, these studies have several limitations. The use of anticoagulants showed an improvement in the outcomes when used for high-risk patients. Their major concern is the tendency to increase bleeding complication. Hence, monitoring of their administration and careful selection of patients to be treated are of great importance.
INTRODUCTION
Vascular complications after liver transplantation (LT) are common despite the progressive improvement and innovations in anastomotic vascular techniques. They frequently result in hepatic failure and graft loss and thus the need for re-transplantation. Hepatic artery thrombosis (HAT) after LT remains the most serious vascular complication with an overall incidence varies from 2% to 9%[1]. It is usually associated with around 50% rate of mortality or re-transplantation[2].
The mechanism of HAT development is not fully understood. It is believed to be multifactorial including both operative and non-operative factors (Table 1)[3,4]. All these factors are involved in causing recipient hypercoagulability and to disturb the unstable rebalanced haemostasis that usually occurs in liver disease patients leading to a rise in the incidence of HAT[5,6].
Table 1.
Risk factors of hepatic artery thrombosis
| Operative factors | Non operative factors |
| Surgical technique | Donor age of more than 60 yr |
| Number of anastomosis | Long cold ischemia time |
| Use of conduits | Preservation damage |
| Vessels kinking | Lack of blood group compatibility |
| Small vessels size | Cytomegalovirus-positive donor status |
| Hypercoagulable recipient status | |
| Recipient cigarette smoking | |
| Rejection | |
| Primary sclerosing cholangitis |
An early diagnosis with immediate treatment is the key to proper management of HAT. Therapeutic options for managing HAT include either revascularization of the transplanted graft or re transplantation[7]. Revascularization can be achieved through arterial reconstruction, surgical thrombectomy, or radiologically guided thrombolysis. Shortage of organs and poor patients conditions may lead physicians to consider revascularization, which can achieve good success rates[8]. Re-transplantation is still the gold standard treatment for HAT but is confounded by both graft availability and the patient’s general condition.
Prophylaxis against HAT in the early postoperative period by usage of antiplatelet or anticoagulant agents is thought to be hazardous by many surgeons because of the risk of postoperative bleeding. However, postoperative pharmacological prophylaxis can reduce the risk of arterial anastomosis thrombosis when used in vascular surgical procedures[9]. The adoption of this in LT could help in reducing the incidence of HAT.
HAEMOSTASIS IN END STAGE LIVER DISEASE
In liver transplant recipient with cirrhosis, considerable changes in the haemostatic system are often found[10]. These changes include thrombocytopenia, platelet functional defects, decreased circulating levels of coagulative factors and decreased fibrinolytic proteins. Although routine diagnostic tests of haemostasis are commonly abnormal, interpretation of these tests is more difficult in patients with a complex haemostatic disorder as in cirrhotic patients. It is now well established that patients with cirrhosis and abnormal routine coagulation tests might not have an increased bleeding tendency and that thrombotic complications may still occur[11]. This happens through a state of a rebalanced haemostasis where the changes in the pro-haemostatic pathways are associated with changes in the anti-haemostatic pathways (Figure 1)[12]. The changes that promote bleeding include thrombocytopenia, platelet function defects, enhanced production of nitric oxide and prostacyclin, low levels of factors II, V, VII, IX, X, and XI, vitamin K deficiency, dysfibrinogenemia, low levels of a2-antiplasmin, factor XIII and thrombin-activatable fibrinolysis inhibitor and elevated tissue plasminogen activator level. Those alterations are encountered by others that counteract bleeding such as: elevated levels of von Willebrand factor, decreased levels of ADAMTS-13 (von Willebrand factor cleaving protease), elevated levels of factor VIII, decreased levels of protein C, protein S, antithrombin, a2-macroglobulin and heparin cofactor II and low levels of plasminogen[5,12].
Figure 1.
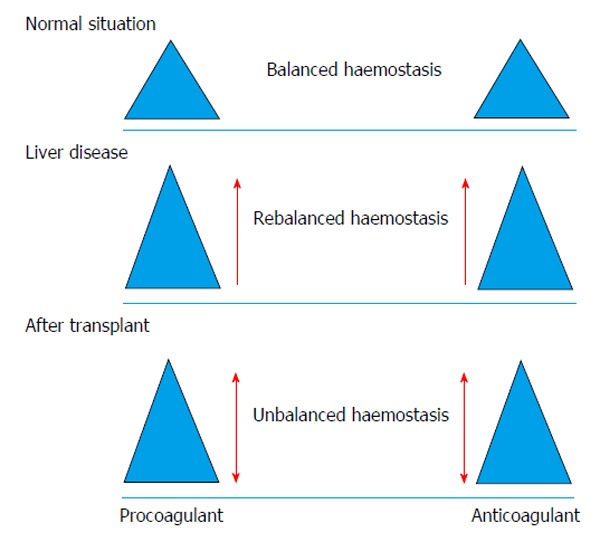
Changes in haemostasis in normal situation, liver disease and after liver transplantation.
The resultant effect of all these changes is a rebalanced haemostasis. Although it is a functional system, it is unstable compared to the haemostatic balance in healthy individuals, explaining the potential occurrence of both bleeding and thrombotic complications in patients with cirrhosis[12].
CHANGES IN THE HAEMOSTATIC BALANCE AFTER LT
In the first days after LT, multiple transplantation-related triggers initiate pro-coagulation, anticoagulation and pro-fibrinolytic cascades. Theses mechanisms might not be balanced properly leading to thrombosis in the area of anastomosis (Figure 1). The triggers include substantial surgical damage, stasis as a result of clamping of major vessels, release of activators from the donor liver and systemic inflammatory responses. Other factors are shown in Table 1[6].
Intraoperatively, the graft endothelium gets activated due to cold ischemia and reperfusion effects. As soon as the reperfusion happens, platelets adhere to the sinusoidal endothelium, which contributes to endothelial cell apoptosis causing more ischemia/reperfusion damage. This process will probably expose additional pro-coagulant triggers causing further platelet activation and initiation of coagulation[13]. As long as these pro-coagulant triggers go on, thrombosis can easily occur. However, the activated fibrinolytic system removes the clots immediately as they are formed. When this balance is disturbed, a state of hypercoagulability arises and a clinically evident thrombus might form in the anastomotic areas[14].
In addition, an acquired hypercoagulability may increase the risk for immediate graft thrombosis. It can be due to transplanting a liver from a donor with factor V Leiden mutation or infections like cytomegalovirus (CMV). Perioperative haemostatic agent such as fresh frozen plasma, platelets, recombinant factor VIIa, and anti-fibrinolytics such as aprotinin and aminocaproic acid plays role as well (Table 2)[12].
Table 2.
Factors involved in development of hypercoagulability after liver transplantation
| Endogenous | Acquired |
| Substantial surgical damage | Donor with factor V Leiden mutation |
| Stasis as a result of clamping of major vessels | Infections |
| Release of activators from the donor liver | Viral infection like cytomegalovirus |
| Systemic inflammatory responses | Perioperative haemostatic agent |
| The quality of the graft | Fresh frozen plasma |
| The length of surgery | Platelets |
| The technique of graft preservation | Recombinant factor VIIa |
| Cold ischemia/reperfusion effect | Anti-fibrinolytics |
| Aprotinin Aminocaproic acid |
Mechanisms of late thrombosis of the graft vascular anastomosis or even systemic thrombosis are less obvious. It could be because of pro-thrombotic side effect of immunosuppressant or as consequences of medical comorbidities like hypertension, hypercholesterolemia and diabetes mellitus. It could happen due to viral infection as well especially CMV[15].
Liver diseases are classically portrayed as having a substantial bleeding tendency. For this reasons, the postoperative use of anticoagulants or antiplatelets has been restricted, in order to limit bleeding complications. However, recent data showed that the bleeding diathesis of patients with liver disease is not only a result of poor haemostasis[16]. Other factors may play a significant role and augment bleeding tendency. Portal hypertension is an example of that. The minimal blood loss and the decreasing requirements of coagulation products in nowadays transplant support this concept. Moreover, improvements in surgical techniques and a restrictive fluid and transfusion protocols has led to a reduction in perioperative transfusion requirements[17]. Considering this fact, the limited use of anticoagulants or antiplatelets in the postoperative period is reconsidered.
USE OF ANTIPLATELETS IN LT
In the immediate periods after LT, the constant platelet activation and aggregation result in development of thromboxane leading to fibrinogen activation, which contribute to arterial thrombosis and graft failure[18]. Because of this pivotal role of platelets, antiplatelets therapy by inhibiting this platelet-activation may lead to reduction in the incidence of such complication. Aspirin, which is the most frequent used antiplatelet agents, interferes with platelet aggregation, which in turn leads to an endothelial cell-mediated inhibition of the coagulation cascade. This happens through irreversible inhibition of cyclooxygenase 1 and hence, inhibition of thromboxane generation[19].
Very few studies focused on the efficacy and safety of antiplatelet therapy in patients after LT. In 1997, in a retrospective study, Wolf et al[20] found no significant difference in the incidence of early HAT (3.7%) vs (4.0%) between patients who had a prophylaxis aspirin (354 of 529 patients) and those who did not. Bleeding events occurred in 1.1% of patients treated with aspirin compared to 0.6% of the control group. The effect of aspirin prophylaxis on late HAT was not investigated[20].
Vivarelli et al[21] reported a single centre retrospective study where they looked to the effect of long-term aspirin administration (100 mg) on the incidence of late HAT in a large number of patients. In this study, they categorize the patients into high and low risk groups based on their finding on a previous study. One of two independent risk factors was used to categorize the patients into either group: grafts retrieved from donors who died from a cerebrovascular accident or the use of an arterial iliac conduit. Late HAT incidence was 3.6% (12 of 338) of the high-risk patients who were not given aspirin, whilst it was seen in only 0.6% (1 of 160) of the high-risk patients who received aspirin prophylaxis. The relative risk reduction was 82%. In the low-risk group, 1 of 330 patients developed late HAT and he was in the non-prophylaxis arm (254 patients). Out of 236 patients who received aspirin, there was no recorded episode of any bleeding complications throughout the follow up period (median of 1704 d). They could not assess the effect of antiplatelets on early HAT due to their inability to start patients immediately on aspirin with a known impaired coagulative function and a high risk of bleeding. This obvious benefit of aspirin on late HAT occurrence should be considered specifically in patients with an absence of bleeding complications.
Shay et al[22] showed that aspirin prophylaxis is safe and effective in decreasing early HAT in adult recipients. The incidence of overall HAT was found to be significantly higher at 4.9% in the control group vs 3.0% in the treated group. Early HAT incidence dropped from 3.9% in the control group to 1.8% with aspirin prophylaxis. Also the incidence of early HAT causing graft loss decreased significantly from 3.6% to 0% with the use of early aspirin prophylaxis. There was no difference in bleeding complications between the two groups. The main difference between these studies is the dosage and the time of initiation of therapy. Shay et al[22] used a higher dosage at 325 mg/d, initiated immediately after surgery with no evidence of significant bleeding.
There are several limitations to these studies that should be considered. First, not all of them include paediatric patients, where the incidence of HAT is higher and survival is better. Secondly, they were all retrospective studies with a higher risk of bias. Also the compared groups were mostly from different time periods where surgical techniques, donor selection, and postoperative management are different. However, these studies showed evidence of benefit from the use of antiplatelet agents as a prophylaxis for early and late HAT without increasing the risk of bleeding or other surgical complications. The current usage of antiplatelet agents in treatment of cardiovascular and peripheral vascular disease might support this conclusion. A further well-designed randomized study to explore this field would be appropriate.
USE OF ANTICOAGULANTS IN LT
The plasma concentration of coagulant and anticoagulant proteins is disturbed after LT. This imbalance leads to hypercoagulability condition that contributes to vascular thrombosis and possible loss of the graft[14]. The reducing level of antithrombin III and protein C are believed to be responsible for the development of this hypercoagulability state[23]. For this reason, supplementation of protein C and augmenting the effect of antithrombin III could help to overcome this haemostatic disturbance.
Fresh frozen plasma (FFP) is usually the source of protein C along with other clotting factors. Hashikura et al[24] reported that infusing FFP was helpful in reducing incidence of HAT and maintaining coagulation haemostasis. In contrast, Mazzaferro et al[25] found a higher incidence of HAT in paediatric liver recipient who received more FFP compared to those who did not receive FFP intraoperatively. Hatano et al[26] found a similar result where the occurrence of HAT was associated with a higher intraoperative infusion of FFP. Although the use of FFP might be associated with an increased risk of HAT, its usage is still warranted to maintain haemostasis and to reduce bleeding complication. Excessive use of FFP should be avoided as it might induce a state of hypercoagulability and could result in graft thrombosis.
Heparin appears to be the method of choice to anticoagulate liver transplant recipients. Most liver transplant centres have developed their own protocols for heparin infusions and the monitoring of its activity. It is important to note that the rationales of these protocols remain unclear, as they are designed based on empirical rules. The Shinshu group demonstrated that intensive anticoagulation should be established in living related liver transplantation (LDLT) in a paediatric Population[24]. Sugawara et al[27] showed a similar result in the setting of living donor LT. The reports on usage of heparin in cadaveric liver transplant are very limited to date. The anti-coagulatory effect of the unfractionated heparin (UFH) is known to be through its antithrombin III activity. The low molecular weight heparin (LMWH) selectively inhibit clotting factor Xa and to a lesser extent augment antithrombin III activity[28].
Bleeding complication can occur with the unmonitored use of heparin. Kaneko et al[28] reported that 9% of their living related liver recipients who used UFH developed haemorrhagic complications that required surgical treatment. In contrast to UFH, using LMWH is believed to be useful to reduce haemorrhagic complications due to its selective inhibition of coagulation factor Xa and because of its reduced ability to bind to endogenous plasma proteins such as platelet factor 4 and von Willebrand factor[29]. In addition, LMWH lessen liver damage in ischemia-reperfusion injury and hyperperfusion[30]. For these reasons, LMWH is more advantageous than UFH for intraoperative and postoperative anticoagulant therapy in LT. The major problem for the prophylactic use of LMWH is determining the optimal dose and monitoring serum factor Xa activity. The route of administration of LMWH depends on the indication. In patients with a high bleeding tendency, such as liver transplant recipients, an adjustable continuous infusion may be recommended to avoid increased plasma levels and to cope with continuous pathophysiological changes in the coagulation cascade[31].
Antithrombin is plasma glycoprotein synthesized in the liver and plays a major role in the coagulation after LT. The level of antithrombin III drops after transplant and remains low for up to two weeks. Replacing this drop might help to gain an adequate anticoagulation effect[32]. Kaneko et al[32] in his pilot study found that the combined use of AT and UFH might reduce fibrin degradation product D-dimer levels and prevent a postoperative drop in the platelet count. Taniai et al[33] concluded in his study that adding antithrombin to heparin could be the best approach. Further research should be done to prove its benefit and safety in LT[33].
Monitoring of anticoagulation after LT assures an adequate level without an increase in the bleeding complications. Activated clotting time (ACT) is the most commonly used monitoring method. Linkins et al[34] showed that UFH is more sensitive than LMWH in regards to ACT level. This indicates that the ACT cannot monitor the activity of factor Xa but is still a valuable tool in monitoring the anticoagulant effects of LMWH. The lower level of antithrombin activity in the LMWH compared to the anti-Xa activity could explain this lower sensitivity[29]. It has been shown that ACT can monitor the anticoagulatory effect of LMWH in coronary intervention procedures[35]. Uchikawa et al[31] showed that ACT measurement is a simple, reliable method for bedside monitoring of LMWH anticoagulant effects for LDLT. It is assumed that ACT level should be kept within the normal range in order to prevent haemorrhagic complication. Thus, the anticipated value of ACT is between 140 and 150 s, which is the upper limit of the normal range. However, Kaneko et al[32] tested the ACT level by measuring plasmin-alpha2 plasmin inhibitor complex, thrombin-antithrombin III complex and fibrin degradation product pre and postoperatively with measurement of complete blood count, ACT, activated partial thromboplastin time and prothrombin time international normalized ratio for two weeks after surgery. They conclude that frequent monitoring of ACT is necessary to keep the ACT level in the target range in the first postoperative week. Because of hyper-fibrinolytic condition and the high rate of haemorrhagic complications after the first week, the dose of heparin should be adjusted to maintain lower ACT levels during this period.
In contrast to UFH, LMWH are cleared by renal route. Hence in patients with impaired renal functions, as commonly seen following LT, monitoring and adjustment of the dose according to the degree of renal injury are required. Observational studies have shown more bleeding complications in renal impaired patients[36]. Prophylactic LMWH doesn’t appear to increase the bleeding tendency and therefore might not need monitoring or adjustment[37]. Therapeutic LMWH bio accumulates and cause more bleeding if left unadjusted[38]. This bioaccumulation is more evident when creatinine clearance is less than 30 mL/min[38]. No clear guidelines are available for dose adjustment and further clinical and pharmacological studies are required for dosage guidance[39].
It is clear that a further study looking to the appropriate protocols of anticoagulation and the proper monitoring tools is needed. The rarity of studies and the empirical assumption of tailoring the protocols make drawing a conclusion difficult.
CONCLUSION
Pharmacological prophylaxis is probably beneficial in reducing the incidence of HAT. It is relatively safe if used carefully with a continuous monitoring and adjustment. Proper protocols need to be developed based on proper well-designed clinical studies.
Footnotes
P- Reviewer: Grassi A, Zielinski J S- Editor: Song XX L- Editor: A E- Editor: Liu SQ
Conflict-of-interest: None of the authors has any potential conflicting financial interests relevant to this article.
Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Peer-review started: August 30, 2014
First decision: October 14, 2014
Article in press: February 11, 2015
References
- 1.Mourad MM, Liossis C, Gunson BK, Mergental H, Isaac J, Muiesan P, Mirza DF, Perera MT, Bramhall SR. Etiology and management of hepatic artery thrombosis after adult liver transplantation. Liver Transpl. 2014;20:713–723. doi: 10.1002/lt.23874. [DOI] [PubMed] [Google Scholar]
- 2.Stange BJ, Glanemann M, Nuessler NC, Settmacher U, Steinmüller T, Neuhaus P. Hepatic artery thrombosis after adult liver transplantation. Liver Transpl. 2003;9:612–620. doi: 10.1053/jlts.2003.50098. [DOI] [PubMed] [Google Scholar]
- 3.Bekker J, Ploem S, de Jong KP. Early hepatic artery thrombosis after liver transplantation: a systematic review of the incidence, outcome and risk factors. Am J Transplant. 2009;9:746–757. doi: 10.1111/j.1600-6143.2008.02541.x. [DOI] [PubMed] [Google Scholar]
- 4.Grodzicki M, Anysz-Grodzicka A, Remiszewski P, Cieślak B, Kotulski M, Kalinowski P, Paluszkiewicz R, Rowiński O, Krawczyk M. Treatment of early hepatic artery thrombosis after liver transplantation. Transplant Proc. 2011;43:3039–3042. doi: 10.1016/j.transproceed.2011.08.028. [DOI] [PubMed] [Google Scholar]
- 5.Tripodi A, Primignani M, Chantarangkul V, Dell’Era A, Clerici M, de Franchis R, Colombo M, Mannucci PM. An imbalance of pro- vs anti-coagulation factors in plasma from patients with cirrhosis. Gastroenterology. 2009;137:2105–2111. doi: 10.1053/j.gastro.2009.08.045. [DOI] [PubMed] [Google Scholar]
- 6.Pastacaldi S, Teixeira R, Montalto P, Rolles K, Burroughs AK. Hepatic artery thrombosis after orthotopic liver transplantation: a review of nonsurgical causes. Liver Transpl. 2001;7:75–81. doi: 10.1053/jlts.2001.22040. [DOI] [PubMed] [Google Scholar]
- 7.Tian MG, Tso WK, Lo CM, Liu CL, Fan ST. Treatment of hepatic artery thrombosis after orthotopic liver transplantation. Asian J Surg. 2004;27:213–217; discussion 218. doi: 10.1016/S1015-9584(09)60035-X. [DOI] [PubMed] [Google Scholar]
- 8.Boyvat F, Aytekin C, Harman A, Sevmiş S, Karakayali H, Haberal M. Endovascular stent placement in patients with hepatic artery stenoses or thromboses after liver transplant. Transplant Proc. 2008;40:22–26. doi: 10.1016/j.transproceed.2007.12.027. [DOI] [PubMed] [Google Scholar]
- 9.Cadroy Y, Bossavy JP, Thalamas C, Sagnard L, Sakariassen K, Boneu B. Early potent antithrombotic effect with combined aspirin and a loading dose of clopidogrel on experimental arterial thrombogenesis in humans. Circulation. 2000;101:2823–2828. doi: 10.1161/01.cir.101.24.2823. [DOI] [PubMed] [Google Scholar]
- 10.Lisman T, Leebeek FW, de Groot PG. Haemostatic abnormalities in patients with liver disease. J Hepatol. 2002;37:280–287. doi: 10.1016/s0168-8278(02)00199-x. [DOI] [PubMed] [Google Scholar]
- 11.Lisman T, Leebeek FW. Hemostatic alterations in liver disease: a review on pathophysiology, clinical consequences, and treatment. Dig Surg. 2007;24:250–258. doi: 10.1159/000103655. [DOI] [PubMed] [Google Scholar]
- 12.Lisman T, Porte RJ. Antiplatelet medication after liver transplantation: does it affect outcome? Liver Transpl. 2007;13:644–646. doi: 10.1002/lt.21063. [DOI] [PubMed] [Google Scholar]
- 13.Sindram D, Porte RJ, Hoffman MR, Bentley RC, Clavien PA. Platelets induce sinusoidal endothelial cell apoptosis upon reperfusion of the cold ischemic rat liver. Gastroenterology. 2000;118:183–191. doi: 10.1016/s0016-5085(00)70427-6. [DOI] [PubMed] [Google Scholar]
- 14.Gologorsky E, De Wolf AM, Scott V, Aggarwal S, Dishart M, Kang Y. Intracardiac thrombus formation and pulmonary thromboembolism immediately after graft reperfusion in 7 patients undergoing liver transplantation. Liver Transpl. 2001;7:783–789. doi: 10.1053/jlts.2001.26928. [DOI] [PubMed] [Google Scholar]
- 15.Johnston SD, Morris JK, Cramb R, Gunson BK, Neuberger J. Cardiovascular morbidity and mortality after orthotopic liver transplantation. Transplantation. 2002;73:901–906. doi: 10.1097/00007890-200203270-00012. [DOI] [PubMed] [Google Scholar]
- 16.Lisman T, Caldwell SH, Leebeek FW, Porte RJ. Is chronic liver disease associated with a bleeding diathesis? J Thromb Haemost. 2006;4:2059–2060. doi: 10.1111/j.1538-7836.2006.02075.x. [DOI] [PubMed] [Google Scholar]
- 17.de Boer MT, Molenaar IQ, Hendriks HG, Slooff MJ, Porte RJ. Minimizing blood loss in liver transplantation: progress through research and evolution of techniques. Dig Surg. 2005;22:265–275. doi: 10.1159/000088056. [DOI] [PubMed] [Google Scholar]
- 18.Patrono C, Rocca B. Drug insight: aspirin resistance--fact or fashion? Nat Clin Pract Cardiovasc Med. 2007;4:42–50. doi: 10.1038/ncpcardio0728. [DOI] [PubMed] [Google Scholar]
- 19.Fritsma GA, Ens GE, Alvord MA, Carroll AA, Jensen R. Monitoring the antiplatelet action of aspirin. JAAPA. 2001;14:57–58, 61-62. [PubMed] [Google Scholar]
- 20.Wolf DC, Freni MA, Boccagni P, Mor E, Chodoff L, Birnbaum A, Miller CM, Schwartz ME, Bodenheimer HC. Low-dose aspirin therapy is associated with few side effects but does not prevent hepatic artery thrombosis in liver transplant recipients. Liver Transpl Surg. 1997;3:598–603. doi: 10.1002/lt.500030608. [DOI] [PubMed] [Google Scholar]
- 21.Vivarelli M, La Barba G, Cucchetti A, Lauro A, Del Gaudio M, Ravaioli M, Grazi GL, Pinna AD. Can antiplatelet prophylaxis reduce the incidence of hepatic artery thrombosis after liver transplantation? Liver Transpl. 2007;13:651–654. doi: 10.1002/lt.21028. [DOI] [PubMed] [Google Scholar]
- 22.Shay R, Taber D, Pilch N, Meadows H, Tischer S, McGillicuddy J, Bratton C, Baliga P, Chavin K. Early aspirin therapy may reduce hepatic artery thrombosis in liver transplantation. Transplant Proc. 2013;45:330–334. doi: 10.1016/j.transproceed.2012.05.075. [DOI] [PubMed] [Google Scholar]
- 23.Stahl RL, Duncan A, Hooks MA, Henderson JM, Millikan WJ, Warren WD. A hypercoagulable state follows orthotopic liver transplantation. Hepatology. 1990;12:553–558. doi: 10.1002/hep.1840120317. [DOI] [PubMed] [Google Scholar]
- 24.Hashikura Y, Kawasaki S, Okumura N, Ishikawa S, Matsunami H, Ikegami T, Nakazawa Y, Makuuchi M. Prevention of hepatic artery thrombosis in pediatric liver transplantation. Transplantation. 1995;60:1109–1112. doi: 10.1097/00007890-199511270-00009. [DOI] [PubMed] [Google Scholar]
- 25.Mazzaferro V, Esquivel CO, Makowka L, Belle S, Kahn D, Koneru B, Scantlebury VP, Stieber AC, Todo S, Tzakis AG. Hepatic artery thrombosis after pediatric liver transplantation--a medical or surgical event? Transplantation. 1989;47:971–977. doi: 10.1097/00007890-198906000-00011. [DOI] [PubMed] [Google Scholar]
- 26.Hatano E, Terajima H, Yabe S, Asonuma K, Egawa H, Kiuchi T, Uemoto S, Inomata Y, Tanaka K, Yamaoka Y. Hepatic artery thrombosis in living related liver transplantation. Transplantation. 1997;64:1443–1446. doi: 10.1097/00007890-199711270-00012. [DOI] [PubMed] [Google Scholar]
- 27.Sugawara Y, Kaneko J, Akamatsu N, Imamura H, Kokudo N, Makuuchi M. Anticoagulant therapy against hepatic artery thrombosis in living donor liver transplantation. Transplant Proc. 2002;34:3325–3326. doi: 10.1016/s0041-1345(02)03576-5. [DOI] [PubMed] [Google Scholar]
- 28.Kaneko J, Sugawara Y, Tamura S, Togashi J, Matsui Y, Akamatsu N, Kishi Y, Makuuchi M. Coagulation and fibrinolytic profiles and appropriate use of heparin after living-donor liver transplantation. Clin Transplant. 2005;19:804–809. doi: 10.1111/j.1399-0012.2005.00425.x. [DOI] [PubMed] [Google Scholar]
- 29.Weitz JI. Low-molecular-weight heparins. N Engl J Med. 1997;337:688–698. doi: 10.1056/NEJM199709043371007. [DOI] [PubMed] [Google Scholar]
- 30.Harada N, Okajima K, Uchiba M. Dalteparin, a low molecular weight heparin, attenuates inflammatory responses and reduces ischemia-reperfusion-induced liver injury in rats. Crit Care Med. 2006;34:1883–1891. doi: 10.1097/01.CCM.0000220764.10155.03. [DOI] [PubMed] [Google Scholar]
- 31.Uchikawa Y, Ikegami T, Masuda Y, Ohno Y, Mita A, Urata K, Nakazawa Y, Terada M, Miyagawa S. Administration of dalteparin based on the activated clotting time for prophylaxis of hepatic vessel thrombosis in living donor liver transplantation. Transplant Proc. 2009;41:3784–3790. doi: 10.1016/j.transproceed.2009.04.011. [DOI] [PubMed] [Google Scholar]
- 32.Kaneko J, Sugawara Y, Tamura S, Togashi J, Matsui Y, Makuuchi M. Antithrombin effect on coagulation and fibrinolytic profiles after living donor liver transplantation: a pilot study. Int J Lab Hematol. 2009;31:81–86. doi: 10.1111/j.1751-553X.2007.01008.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Taniai N, Onda M, Tajiri T, Akimaru K, Yoshida H, Mamada Y, Yokomuro S, Mineta S, Yoshioka M, Hirakata A, et al. Anticoagulant therapy in living-related liver transplantation. Transplant Proc. 2002;34:2788–2790. doi: 10.1016/s0041-1345(02)03414-0. [DOI] [PubMed] [Google Scholar]
- 34.Linkins LA, Julian JA, Rischke J, Hirsh J, Weitz JI. In vitro comparison of the effect of heparin, enoxaparin and fondaparinux on tests of coagulation. Thromb Res. 2002;107:241–244. doi: 10.1016/s0049-3848(02)00340-7. [DOI] [PubMed] [Google Scholar]
- 35.Marmur JD, Anand SX, Bagga RS, Fareed J, Pan CM, Sharma SK, Richard MF. The activated clotting time can be used to monitor the low molecular weight heparin dalteparin after intravenous administration. J Am Coll Cardiol. 2003;41:394–402. doi: 10.1016/s0735-1097(02)02762-6. [DOI] [PubMed] [Google Scholar]
- 36.Gerlach AT, Pickworth KK, Seth SK, Tanna SB, Barnes JF. Enoxaparin and bleeding complications: a review in patients with and without renal insufficiency. Pharmacotherapy. 2000;20:771–775. doi: 10.1592/phco.20.9.771.35210. [DOI] [PubMed] [Google Scholar]
- 37.Chan KE, Thadhani RI, Maddux FW. No difference in bleeding risk between subcutaneous enoxaparin and heparin for thromboprophylaxis in end-stage renal disease. Kidney Int. 2013;84:555–561. doi: 10.1038/ki.2013.152. [DOI] [PubMed] [Google Scholar]
- 38.Lim W, Dentali F, Eikelboom JW, Crowther MA. Meta-analysis: low-molecular-weight heparin and bleeding in patients with severe renal insufficiency. Ann Intern Med. 2006;144:673–684. doi: 10.7326/0003-4819-144-9-200605020-00011. [DOI] [PubMed] [Google Scholar]
- 39.Lai S, Coppola B. Use of enoxaparin in end-stage renal disease. Kidney Int. 2013;84:433–436. doi: 10.1038/ki.2013.163. [DOI] [PubMed] [Google Scholar]