

Abstract
Valproic acid (VPA) is one of the most prescribed drugs in children with newly diagnosed epilepsy. Weight gain and obesity have been observed as side effects of VPA. These are often linked with other metabolic disturbances such as development of insulin resistance, dyslipidemia, metabolic syndrome (MetS) and non-alcoholic fatty liver disease or nonalcoholic fatty liver disease (NAFLD). NAFLD refers to a group of liver disorders with marked hepatic steatosis. It is associated with an increased incidence of cardiovascular diseases and overall reduced life expectancy. NAFLD occurs in 20%-25% of the general population and it is known to be the most common cause of chronic liver disease. NAFLD therefore represents a major public health issue worldwide. This study reviews and summarizes relevant literature that supports the existence of an association between VPA therapy and the development of NAFLD in children. Long-term VPA-therapy appears to be associated with an increased risk of developing NAFLD. Further studies are needed to clarify the pathogenic mechanisms that lie behind this association and to standardize the options for the use of this drug in overweight patients and in those with risks for developing MetS and NAFLD.
Keywords: Nonalcoholic fatty liver disease, Valproic acid, Obesity, Insulin resistance
Core tip: Nonalcoholic fatty liver disease (NAFLD) is a major medical issue worldwide. It affects 20%-25% of the general population including children. The term NAFLD covers a wide spectrum of hepatic diseases. These diseases include simple hepatic steatosis, inflammation, cirrhosis and the development of hepatocellular carcinoma. Valproic acid (VPA), one of the most used anti-epileptic drugs, has been investigated as a contributing factor for the development of NAFLD. This association seems stronger with long term VPA therapy. Further studies are required to determine the mechanism of this association.
NONALCOHOLIC FATTY LIVER DISEASE: DEFINITION
Nonalcoholic fatty liver disease (NAFLD) is a group of diseases characterized by steatosis and the absence of a secondary cause for hepatic fat accumulation. Steatosis must be documented histologically or with sonography[1]. Secondary causes of hepatic fat accumulation such as hereditary syndromes, infective diseases, significant alcohol use or steatogenic drugs should be excluded. NAFLD has two subsets. These are nonalcoholic fatty liver (NAFL) and nonalcoholic steatohepatitis (NASH). NAFL is a benign condition characterized by the presence of intrahepatic fat accumulation (micro or macro-vesicular steatosis) without evidence of hepatic injury. NASH has worse lesions like hepatic steatosis with associated inflammation and hepatic injury with or without fibrosis. NASH also poses a risk for the development of cirrhosis and hepatic malignancy. NAFLD can be suspected in findings of slightly elevated liver enzymes. Such blood exam results correlate well with NAFLD in obese patients. Ultrasound and other non-invasive imaging techniques can diagnose the presence of NAFLD[1,2]. However, a histologic evaluation is necessary to accurately assess the degree of steatosis and confirm the distinct inflammatory lesions that characterize NASH. Biopsy of the liver is therefore needed to distinguish simple steatosis from other conditions like steatosis with inflammation, fibrosis, cirrhosis and cancer. The spectrum of lesions associated with NAFLD is presented in Table 1 which shows a validated semi-quantitative scoring system to assess the severity of inflammation (grading), fibrosis (staging) and steatosis in NAFLD. This system is simple and useful in managing both adults and children with any degree of NAFLD. Biopsy samples with scores ≥ 5 are diagnosed as having NASH while scores less than 3 are not considered as NASH[3,4]. The estimated prevalence of NAFLD in the general population is about 20%-25%[1,2]. In children, it has been estimated to be 9%-10%. Several studies have demonstrated that NAFLD is more common in adolescents than in children with a male predominance ratio of 2:1[5,6]. Factors that may explain the higher rate of NAFLD in adolescents include increased circulating hormones, puberty related insulin resistance (IR), diet preferences and having a sedentary lifestyle[6]. Patients with NAFLD are usually asymptomatic[2]. Patients with NASH have a general sensation of being unwell and have an upper right abdominal discomfort[7]. Physical examination may document the presence of hepatomegaly and, rarely, splenomegaly. NAFLD is associated with obesity, dyslipidaemia, type 2 diabetes, IR, metabolic syndrome (MetS). There are also emerging associations between NAFLD and polycystic ovary syndrome, hypothyroidism, hypopituitarism, hypogonadism, obstructive sleep apnea and pancreatico-duodenal resection. Adults with a diagnosis of NAFLD in childhood have a higher risk to develop cardiovascular diseases, MetS, cirrhosis and hepatocellular carcinoma[6]. There are no current specific therapeutic indications for NAFLD. Since most NAFLD patients are overweight or obese, experts recommend lifestyle modification which include proper dieting and exercise programs[8]. It is a primary intervention with the intention of maintaining ideal body weight in this set of patients. For patients with poor compliance or unresponsive to this conservative approach, a pharmacological approach can be considered. Dietary supplementation with docosahexaenoic acid has been shown to improve liver steatosis and insulin sensitivity in children with NAFLD[9,10]. Other therapeutic approaches for NAFLD may include administration of antioxidants such as alpha-tocopherol (vitamin E), insulin sensitizers like metformin, cytoprotective agents like ursodeoxycholic acid, probiotic therapy and bariatric surgery[8,11,12].
Table 1.
Nonalcoholic steato-hepatitis Clinical Research Network Scoring System (adapted from ref. [3])
| Item | Definition | Score/code | |
| Steatosis | |||
| Grade | Low-to medium-power evaluation of parenchymal involvement by steatosis | ||
| < 5% | 0 | ||
| 5%-33% | 1 | ||
| > 33%-66% | 2 | ||
| > 66% | 3 | ||
| Location | Predominant distribution pattern | ||
| Zone 3 | 0 | ||
| Zone 1 | 1 | ||
| Azonal | 2 | ||
| Panacinar | 3 | ||
| Microvesicular steatosis | Contiguous patches | ||
| Not present | 0 | ||
| Present | 1 | ||
| Fibrosis | |||
| Stage | None | 0 | |
| Perisinusoidal or periportal | 1 | ||
| Mild, zone 3, perisinusoidal | 1A | ||
| Moderate, zone 3, perisinusoidal | 1B | ||
| Portal/periportal | 1C | ||
| Perisinusoidal and portal/periportal | 2 | ||
| Bridging fibrosis | 3 | ||
| Cirrhosis | 4 | ||
| Inflammation | |||
| Lobular inflammation | Overall assessment of all inflammatory foci | ||
| No foci | 0 | ||
| < 2 foci per 200 × field | 1 | ||
| 2-4 foci per 200 × field | 2 | ||
| > 4 foci per 200 × field | 3 | ||
| Microgranulomas | Small aggregates of macrophages | ||
| Absent | 0 | ||
| Present | 1 | ||
| Large lipogranulomas | Usually in portal areas or adjacent to central veins | ||
| Absent | 0 | ||
| Present | 1 | ||
| Portal inflammation | Assessed from low magnification | ||
| None to minimal | 0 | ||
| Greater than minimal | 1 | ||
| Liver cell injury | |||
| Ballooning | None | 0 | |
| Few balloon cells | 1 | ||
| Many cells/prominent ballooning | 2 | ||
| Acidophil bodies | None to rare | 0 | |
| Many | 1 | ||
| Pigmented macrophages | None to rare | 0 | |
| Many | 1 | ||
| Megamitochondria | None to rare | 0 | |
| Many | 1 | ||
| Other findings | |||
| Mallory's hyaline | Visible on routine stains | ||
| None to rare | 0 | ||
| Many | 1 | ||
| Glycogenated nuclei | Contiguous patches | ||
| None to rare | 0 | ||
| Many | 1 | ||
VALPROIC ACID: MAIN SIDE EFFECTS
Valproic acid (VPA) is a widely used antiepileptic drug (AED). It is effective against many types of seizure disorders either alone or as a component of a multidrug regimen. It was commercialized in 1969 in France and 1978 in United States. VPA has a broad spectrum of activity against generalized and partial epilepsy in both adults and children. VPA is generally regarded as a first-choice agent for newly diagnosed epilepsy[13]. Recently, it has been used for other medical conditions such as neuropathic pain, in prophylaxis for migraine headaches and as a mood stabilizer for specific psychiatric disorders. VPA is sometimes used for controlling behavioral disturbances in dementia patients and in treating spinal muscular atrophy[14]. It has been estimated that more than one million people in the world are taking VPA every day. It may as well be the most widely prescribed antiepileptic drug world-wide[15]. VPA is available in oral (immediate release, enteric-coated and delayed-release) and parenteral preparations. The side effects of this drug are listed in Table 2[16,17].
Table 2.
Main side effects of valproic acid
| GI disorders: an increase of liver enzymes is common, particularly in early treatment, and it may be transient. Nausea and diarrhea occur frequently at the beginning of treatment, but disappear after a few days without discontinuing treatment. Rare cases of pancreatitis have been reported |
| Nervous system disorders: transient side effects such as dizziness, headache, tremor, diplopia and sedation have been evaluated and they can lead to the reduction or the discontinuation of the drug |
| Weight gain: being overweight at the beginning of treatment may be a significant predictor of further weight gain with VPA |
| Blood dyscrasias: different studies demonstrated the association of VPA with pro and anticoagulatory effects and they are dose-dependent |
| Endocrinological disorders: there is a correlation between hypothyroidism and treatment with VPA in monotherapy; moreover, VPA increases the synthesis of Testosterone and decreases its conversion to Estradiol, leading to the PCOS with amenorrhea and irregular periods |
| Hair loss: it is usually transient and sometimes dose-related. Regrowth normally begins within 6 months after the end of the therapy |
| Hypersensitivity: this effect is rare and dose, time, frequency-independent |
| Teratogenicity: despite VPA can induce teratogenic effects during pregnancy, United States Food and Drugs Administration considers acceptable the risk/benefit ratio. The most common teratogenic effect is the delay/impaired development |
VPA: Valproic acid; PCOS: Polycystic ovary syndrome.
In 1978, several clinical studies revealed the existence of VPA-related biochemical abnormalities in the liver. Hepatotoxicity associated with VPA may manifest as one of the following conditions: (1) Hyperammonaemia: It can be observed as an isolated biochemical finding discovered on a routine blood examination. It can be a symptomatic condition with progressive impairment of consciousness and ataxia that is usually preceded by gastrointestinal symptoms like nausea, vomiting, anorexia and diarrhea. Generally, hyperammonaemia and its related symptoms resolve after one to three days of drug discontinuation[18]; (2) Hepatitis-like syndrome: It is characterized by a dose-dependent elevation of serum aminotransferases. Majority of the patients are asymptomatic but a few can manifest symptoms of malaise, anorexia and lethargy. Biochemical abnormalities and clinical aspects usually normalize after discontinuing the drug[16,18]; (3) Reye’s-like syndrome: It is a dangerous, rare and idiosyncratic condition. Patients usually manifest with acute onset of high fever, vomiting, anorexia, lethargy, loss of consciousness and cerebral edema[16,18]; and (4) NAFLD: The steatogenic effect of VPA has been demonstrated since the beginning of the 1980s. This was documented by histology of liver tissue taken from patients considered to have died from VPA hepatotoxicity[19] and by experimental studies on animals[20,21].
The pathology behind the development of hepatotoxicity, hyperammonaemia and NAFLD in relation to VPA therapy is still poorly understood.
VPA, WEIGHT GAIN AND INSULIN RESISTANCE
The association between VPA-therapy and weight gain was first proved in a study performed in 1981[22]. The frequency of developing obesity in children treated with VPA ranged from 10% to 70%[23]. Most affected patients were peri-pubertal girls who underwent a prolonged therapy and were already overweight from the beginning of treatment[23]. The pathogenic mechanisms of VPA-induced weight gain remains unclear and is most likely multifactorial. It is regulated centrally and peripherally by various neuropeptides and cytokines (Figure 1). These regulatory substances include resistin, fasting-induced adipose factor (FIAF), adiponectin, leptin, ghrelin and visfatin[23]. VPA may increase appetite and craving by enhancing gamma-aminobutyric acid (GABA) transmission in the hypothalamic pathways. VPA may also modify gene expression of adipokines such as resistin and FIAF. This could lead to leptin and insulin resistance and eventually, obesity. These mechanisms have been suggested in patients treated with VPA[24-26]. Adiponectin is a protein that belongs to the adipokine family. It plays an important role in the modulation of lipid metabolism and insulin sensitivity and therefore in body-weight regulation[27]. VPA has been shown to down-regulate adiponectin gene expression in adipocytes[28] and increase the gene expression of its receptor (adipoR1) in liver cells. This contributes to the dysregulation of fatty acid oxidation[29]. Leptin, another protein of the adipokine group, suppresses hunger and increases fatty acid metabolism within the adipocytes[30]. Its serum concentration and mRNA expression in adipose tissue is directly related to fasting insulin serum concentrations and to the obesity severity[31]. Increased serum leptin and leptin resistance was frequently reported in obese patients undergoing long term VPA therapy. Normal leptin levels were observed in non-obese patients[31,32]. The leptin levels and resistance may not be directly affected by VPA but could be a consequence of the abundance in adipose tissue[31,32]. Ghrelin is an orexigenic hormone which acts in increasing appetite. Plasma ghrelin levels increase before meals and decrease post-prandial[33]. Moreover, ghrelin regulates the secretion of leptin and insulin and preferentially consumes carbohydrates over lipids[33]. There is an increase in ghrelin levels in the early period of VPA-treatment[34]. Hyperinsulinaemia has been extensively reported during VPA-therapy[26,35]. It is known that this alteration is often associated with obesity, dyslipidaemia and insulin resistance. Some authors do not consider insulin resistance as an effect of weight gain. Rather, they consider it as a trigger for the development of weight gain itself[35,36]. This is supported by the observation that VPA-induced obesity is related to an increase in insulin levels and a decrease in glucose levels[23]. This could stimulate appetite and therefore lead to obesity. A study on the prevalence of MetS among a group of obese Chinese patients treated with VPA for epilepsy revealed that the homeostasis model assessment index was higher in the VPA-obese patients than in the non-VPA treated obese control group[36]. This supports the hypothesis that VPA may be the trigger for IR. These findings have also been confirmed by a study which showed that both obese and lean patients taking VPA had higher serum insulin levels compared to their respective control groups with similar body mass index (BMI) values[35]. Different hypotheses regarding the role of VPA in determining hyperinsulinaemia and IR have been formulated: (1) VPA is a GABA agonist which may increase insulin levels directly stimulating GABA receptors of pancreatic beta-cells[37,38]; (2) VPA and its metabolites may increase oxidative stress and consequently cause pancreatic beta-cells dysfunction[39,40]; (3) VPA can affect the sympathetic response to glucose load[41]; (4) VPA metabolism can compete with fatty acid mitochondrial oxidation thus increasing free fatty acid plasma levels and therefore increase insulin release from pancreatic beta-cells[42,43]; and (5) VPA can impair insulin signal transduction pathway by inhibiting GLUT-1 mRNA expression[44]. GLUT-1 is a cell membrane carrier involved in the insulin transduction signal pathway.
Figure 1.
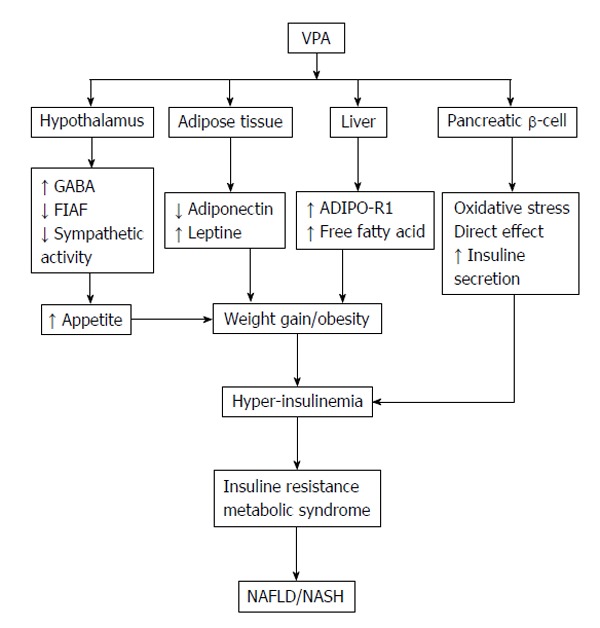
Pathogenic mechanisms of valproic acid-induced nonalcoholic fatty liver disease/nonalcoholic steato-hepatitis. VPA: Valproic acid; GABA: Gamma-aminobutyric acid; FIAF: Fasting-induced adipose factor; ADIPO-R1: Adiponectin receptor expression; NAFLD: Nonalcoholic fatty liver disease; NASH: Nonalcoholic steato-hepatitis.
On the other side of the spectrum, some others authors believe that IR and MetS are the consequences and not the trigger for increased body fat. Supporting this theory, a recent 2010 study reported that about 40% of patients who became obese during treatment with VPA developed MetS and IR, while patients who did not gain weight did not manifest such metabolic changes[45].
In summary, irrespective of the mechanism involved, VPA significantly increases body-weight and therefore the likelihood of obesity, IR and MetS. All these conditions are important risk factors for the development of cardiovascular complications, diabetes, dyslipidemia and intrahepatic fat accumulation (NAFLD). The choice of initiating VPA-therapy is a decision that should thus be made after evaluating the individual risks and benefits posed by the treatment especially in children[23].
VPA AND NAFLD
Despite the growing body of literature regarding NAFLD, the role of VPA-therapy in the development of this liver disease is poorly understood. Luef et al[46] in 2004 published a pilot study. In a group of forty-five non-diabetic, non-obese, epileptic patients treated with VPA or carbamazepine (CBZ) monotherapy for at least two years, ultrasound features of fatty liver disease were found in 61% of the VPA-treated patients compared to 23% of CBZ-treated patients[46]. In 2009, the same authors led a cross-sectional controlled study where sixty-eight non-diabetic and non-obese epileptic patients received either VPA, CBZ or lamotrigine (LTG) as monotherapy for at least two years. They were compared with sixteen healthy controls. All the patients were evaluated by abdominal ultrasound and by measurement of serum fasting insulin and glucose, serum lipids, liver function parameters and anthropometric data. They demonstrated ultrasound characteristics of NAFLD in 60.9% of patients treated with VPA, in 22.7% with CBZ, in 8.7% with LTG and in 12.5% of healthy controls. The mean BMI was significantly higher in the VPA-treated group compared to LTG group and controls (P = 0.015 and P = 0.049 respectively). The authors emphasized the importance of regular ultrasound monitoring as well as measuring serum lipids and BMI during treatment with VPA and other AEDs[47]. In 2005, a Spanish group reported three cases of adult NAFLD in patients receiving long term VPA-therapy for epilepsy. NAFLD was diagnosed by ultrasound evaluation and by histological findings in one case. At the time of diagnosis the patients were asymptomatic but obese, dyslipidemic and with slightly elevated serum aminotransferases. Treatment with VPA was interrupted and interestingly, some months later, aminotransferase levels normalized and the ultrasound evidence of NAFLD disappeared[48]. The first pediatric case of an eleven year old pre-pubertal girl who developed NAFLD after one year of treatment with VPA was reported in 2004. At the beginning of the treatment, the girl had a normal body mass index (between 50th-75th percentiles) and normal routine biochemical serum laboratory exams. Her serum exams included albumin, total proteins, alanine-aminotransferase, aspartate-aminotransferase, gamma-glutamyltransferase, ammonia and lipid profile. No major changes were noted during the first six months of therapy with VPA. After twelve months the patient showed a clear increase in BMI (95th percentile) and a threefold increase in serum aminotransferases values. At this time an ultrasound scan of the abdomen revealed NAFLD. The VPA treatment was replaced with LEV. Three months later, serum liver enzymes returned to normal values and NAFLD disappeared[49]. In 2011, the same authors published a cross sectional double-controlled study to highlight the prevalence of NAFLD in adolescents receiving VPA. Eighty-six adolescents with epilepsy who had received VPA monotherapy for at least twelve months and had a normal weight (BMI < 85th percentile) before starting VPA were enrolled. During the same period, two groups of subjects for comparison were taken. Sixty seven age and sex-matched adolescents with normal weight (normal weight controls) and forty three age, sex and BMI-matched adolescents (weight-matched controls) were included. The occurrence of NAFLD was significantly higher in the VPA-treated patients than in the normal weight control group (36% vs 7.5% respectively, P < 0.001) but was surprisingly similar between the VPA-treated and weight-matched control (36% vs 34.9% respectively, P > 0.05). Considering these data, the authors hypothesized that even if there is a clear association between NAFLD and VPA-treatment, the development of NAFLD may not be the consequence of the action of the VPA-metabolites per se[50]. It may be the consequence of the weight gain, MetS and IR induced by VPA. Finally, a recent 2012 cross-sectional controlled study performed by an Egyptian group evaluated the presence of NAFLD in thirty-eight children and adolescents treated with VPA, CBZ or in combination for at least eight months. Interestingly, they found characteristics of NAFLD in 42.8% of VPA, in 21.4% of CBZ, in 60% of combination therapy and none in the healthy control group[51]. In this study, the diagnosis of hepatic steatosis was made by an abdominal computer tomography scan. This diagnostic modality is not normally recommended due to the unjustified radiation exposure especially for the pediatric population[12].
CONCLUSION
Long term VPA-therapy is associated with an increased development of NAFLD. Evidences from the current literature indicate that the association is particularly strong in patients who are initially overweight with presenting features of MetS. The pathogenic mechanisms through which VPA leads to obesity, MetS and increased risk of NAFLD are still an issue for debate. Further studies are needed to clarify the chronology and sequencing of events between NAFLD, weight gain, MetS and VPA therapy and to determine if any VPA metabolite is involved. Patients in VPA-treatment who gain weight or develop features of MetS should be closely monitored to prevent or detect the early development of NAFLD. Monitoring with abdominal ultrasound, liver function tests, lipid profile and fasting blood glucose determination is strongly recommended in patients taking VPA alone or as part of a multi-AED treatment. Finally, the option to replace or retain VPA-therapy in obese patients, in patients who quickly gain weight during the treatment and in patients with risks of developing MetS and NAFLD requires standardization.
Footnotes
P- Reviewer: Farris AB, Pan JJ S- Editor: Ji FF L- Editor: A E- Editor: Liu SQ
Conflict-of-interest: The researchers involved in this study have no financial interests and are not affiliated in any company involved with the medications mentioned in this research.
Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Peer-review started: November 22, 2014
First decision: December 26, 2014
Article in press: February 9, 2015
References
- 1.Chalasani N, Younossi Z, Lavine JE, Diehl AM, Brunt EM, Cusi K, Charlton M, Sanyal AJ. The diagnosis and management of non-alcoholic fatty liver disease: practice guideline by the American Gastroenterological Association, American Association for the Study of Liver Diseases, and American College of Gastroenterology. Gastroenterology. 2012;142:1592–1609. doi: 10.1053/j.gastro.2012.04.001. [DOI] [PubMed] [Google Scholar]
- 2.Loria P, Adinolfi LE, Bellentani S, Bugianesi E, Grieco A, Fargion S, Gasbarrini A, Loguercio C, Lonardo A, Marchesini G, et al. Practice guidelines for the diagnosis and management of nonalcoholic fatty liver disease. A decalogue from the Italian Association for the Study of the Liver (AISF) Expert Committee. Dig Liver Dis. 2010;42:272–282. doi: 10.1016/j.dld.2010.01.021. [DOI] [PubMed] [Google Scholar]
- 3.Kleiner DE, Brunt EM, Van Natta M, Behling C, Contos MJ, Cummings OW, Ferrell LD, Liu YC, Torbenson MS, Unalp-Arida A, et al. Design and validation of a histological scoring system for nonalcoholic fatty liver disease. Hepatology. 2005;41:1313–1321. doi: 10.1002/hep.20701. [DOI] [PubMed] [Google Scholar]
- 4.Schwimmer JB, Behling C, Newbury R, Deutsch R, Nievergelt C, Schork NJ, Lavine JE. Histopathology of pediatric nonalcoholic fatty liver disease. Hepatology. 2005;42:641–649. doi: 10.1002/hep.20842. [DOI] [PubMed] [Google Scholar]
- 5.Barshop NJ, Francis CS, Schwimmer JB, Lavine JE. Nonalcoholic fatty liver disease as a comorbidity of childhood obesity. Ped Health. 2009;3:271–281. doi: 10.2217/phe.09.21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Giorgio V, Prono F, Graziano F, Nobili V. Pediatric non alcoholic fatty liver disease: old and new concepts on development, progression, metabolic insight and potential treatment targets. BMC Pediatr. 2013;13:40. doi: 10.1186/1471-2431-13-40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Chopra S. Patient information. Nonalcoholic steatohepatitis (NASH) (Beyond the basics). [Up date 2013] Available from: http://www.uptodate.com/contents/nonalcoholic-fatty-liver-disease-nafld-including-nonalcoholic-steatohepatitis-nash-beyond-the-basics.
- 8.Nobili V, Alisi A, Raponi M. Pediatric non-alcoholic fatty liver disease: preventive and therapeutic value of lifestyle intervention. World J Gastroenterol. 2009;15:6017–6022. doi: 10.3748/wjg.15.6017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Nobili V, Bedogni G, Alisi A, Pietrobattista A, Risé P, Galli C, Agostoni C. Docosahexaenoic acid supplementation decreases liver fat content in children with non-alcoholic fatty liver disease: double-blind randomised controlled clinical trial. Arch Dis Child. 2011;96:350–353. doi: 10.1136/adc.2010.192401. [DOI] [PubMed] [Google Scholar]
- 10.Nobili V, Carpino G, Alisi A, De Vito R, Franchitto A, Alpini G, Onori P, Gaudio E. Role of docosahexaenoic acid treatment in improving liver histology in pediatric nonalcoholic fatty liver disease. PLoS One. 2014;9:e88005. doi: 10.1371/journal.pone.0088005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Iacono A, Raso GM, Canani RB, Calignano A, Meli R. Probiotics as an emerging therapeutic strategy to treat NAFLD: focus on molecular and biochemical mechanisms. J Nutr Biochem. 2011;22:699–711. doi: 10.1016/j.jnutbio.2010.10.002. [DOI] [PubMed] [Google Scholar]
- 12.Nobili V, Svegliati-Baroni G, Alisi A, Miele L, Valenti L, Vajro P. A 360-degree overview of paediatric NAFLD: recent insights. J Hepatol. 2013;58:1218–1229. doi: 10.1016/j.jhep.2012.12.003. [DOI] [PubMed] [Google Scholar]
- 13.Guerrini R. Valproate as a mainstay of therapy for pediatric epilepsy. Paediatr Drugs. 2006;8:113–129. doi: 10.2165/00148581-200608020-00004. [DOI] [PubMed] [Google Scholar]
- 14.Tyrer P, Bateman AW. Drug treatment for personality disorders. Advances in Psychiatric Treatment. 2004;10:389–398. [Google Scholar]
- 15.Perucca E. Pharmacological and therapeutic properties of valproate: a summary after 35 years of clinical experience. CNS Drugs. 2002;16:695–714. doi: 10.2165/00023210-200216100-00004. [DOI] [PubMed] [Google Scholar]
- 16.Gerstner T, Bell N, König S. Oral valproic acid for epilepsy--long-term experience in therapy and side effects. Expert Opin Pharmacother. 2008;9:285–292. doi: 10.1517/14656566.9.2.285. [DOI] [PubMed] [Google Scholar]
- 17.Nanau RM, Neuman MG. Adverse drug reactions induced by valproic acid. Clin Biochem. 2013;46:1323–1338. doi: 10.1016/j.clinbiochem.2013.06.012. [DOI] [PubMed] [Google Scholar]
- 18.Powell-Jackson PR, Tredger JM, Williams R. Hepatotoxicity to sodium valproate: a review. Gut. 1984;25:673–681. doi: 10.1136/gut.25.6.673. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Zimmerman HJ, Ishak KG. Valproate-induced hepatic injury: analyses of 23 fatal cases. Hepatology. 1982;2:591–597. doi: 10.1002/hep.1840020513. [DOI] [PubMed] [Google Scholar]
- 20.Lewis JH, Zimmerman HJ, Garrett CT, Rosenberg E. Valproate-induced hepatic steatogenesis in rats. Hepatology. 1982;2:870–873. doi: 10.1002/hep.1840020622. [DOI] [PubMed] [Google Scholar]
- 21.Olson MJ, Handler JA, Thurman RG. Mechanism of zone-specific hepatic steatosis caused by valproate: inhibition of ketogenesis in periportal regions of the liver lobule. Mol Pharmacol. 1986;30:520–525. [PubMed] [Google Scholar]
- 22.Egger J, Brett EM. Effects of sodium valproate in 100 children with special reference to weight. Br Med J (Clin Res Ed) 1981;283:577–581. doi: 10.1136/bmj.283.6291.577. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Verrotti A, D’Egidio C, Mohn A, Coppola G, Chiarelli F. Weight gain following treatment with valproic acid: pathogenetic mechanisms and clinical implications. Obes Rev. 2011;12:e32–e43. doi: 10.1111/j.1467-789X.2010.00800.x. [DOI] [PubMed] [Google Scholar]
- 24.Brown R, Imran SA, Ur E, Wilkinson M. Valproic acid and CEBPalpha-mediated regulation of adipokine gene expression in hypothalamic neurons and 3T3-L1 adipocytes. Neuroendocrinology. 2008;88:25–34. doi: 10.1159/000113927. [DOI] [PubMed] [Google Scholar]
- 25.Howard JK, Flier JS. Attenuation of leptin and insulin signaling by SOCS proteins. Trends Endocrinol Metab. 2006;17:365–371. doi: 10.1016/j.tem.2006.09.007. [DOI] [PubMed] [Google Scholar]
- 26.Verrotti A, Basciani F, De Simone M, Trotta D, Morgese G, Chiarelli F. Insulin resistance in epileptic girls who gain weight after therapy with valproic acid. J Child Neurol. 2002;17:265–268. doi: 10.1177/088307380201700405. [DOI] [PubMed] [Google Scholar]
- 27.Kawano J, Arora R. The role of adiponectin in obesity, diabetes, and cardiovascular disease. J Cardiometab Syndr. 2009;4:44–49. doi: 10.1111/j.1559-4572.2008.00030.x. [DOI] [PubMed] [Google Scholar]
- 28.Qiao L, Schaack J, Shao J. Suppression of adiponectin gene expression by histone deacetylase inhibitor valproic acid. Endocrinology. 2006;147:865–874. doi: 10.1210/en.2005-1030. [DOI] [PubMed] [Google Scholar]
- 29.Greco R, Latini G, Chiarelli F, Iannetti P, Verrotti A. Leptin, ghrelin, and adiponectin in epileptic patients treated with valproic acid. Neurology. 2005;65:1808–1809. doi: 10.1212/01.wnl.0000187074.27586.d1. [DOI] [PubMed] [Google Scholar]
- 30.Aydin K, Serdaroglu A, Okuyaz C, Bideci A, Gucuyener K. Serum insulin, leptin, and neuropeptide y levels in epileptic children treated with valproate. J Child Neurol. 2005;20:848–851. doi: 10.1177/08830738050200101501. [DOI] [PubMed] [Google Scholar]
- 31.Verrotti A, Basciani F, Morresi S, de Martino M, Morgese G, Chiarelli F. Serum leptin changes in epileptic patients who gain weight after therapy with valproic acid. Neurology. 1999;53:230–232. doi: 10.1212/wnl.53.1.230. [DOI] [PubMed] [Google Scholar]
- 32.Hamed SA. Leptin and insulin homeostasis in epilepsy: relation to weight adverse conditions. Epilepsy Res. 2007;75:1–9. doi: 10.1016/j.eplepsyres.2007.04.001. [DOI] [PubMed] [Google Scholar]
- 33.Asakawa A, Inui A, Kaga T, Katsuura G, Fujimiya M, Fujino MA, Kasuga M. Antagonism of ghrelin receptor reduces food intake and body weight gain in mice. Gut. 2003;52:947–952. doi: 10.1136/gut.52.7.947. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Gungor S, Yücel G, Akinci A, Tabel Y, Ozerol IH, Yologlu S. The role of ghrelin in weight gain and growth in epileptic children using valproate. J Child Neurol. 2007;22:1384–1388. doi: 10.1177/0883073807307096. [DOI] [PubMed] [Google Scholar]
- 35.Pylvänen V, Knip M, Pakarinen A, Kotila M, Turkka J, Isojärvi JI. Serum insulin and leptin levels in valproate-associated obesity. Epilepsia. 2002;43:514–517. doi: 10.1046/j.1528-1157.2002.31501.x. [DOI] [PubMed] [Google Scholar]
- 36.Fang J, Chen S, Tong N, Chen L, An D, Mu J, Zhou D. Metabolic syndrome among Chinese obese patients with epilepsy on sodium valproate. Seizure. 2012;21:578–582. doi: 10.1016/j.seizure.2012.06.001. [DOI] [PubMed] [Google Scholar]
- 37.Luef GJ, Lechleitner M, Bauer G, Trinka E, Hengster P. Valproic acid modulates islet cell insulin secretion: a possible mechanism of weight gain in epilepsy patients. Epilepsy Res. 2003;55:53–58. doi: 10.1016/s0920-1211(03)00091-3. [DOI] [PubMed] [Google Scholar]
- 38.Shi Y, Kanaani J, Menard-Rose V, Ma YH, Chang PY, Hanahan D, Tobin A, Grodsky G, Baekkeskov S. Increased expression of GAD65 and GABA in pancreatic beta-cells impairs first-phase insulin secretion. Am J Physiol Endocrinol Metab. 2000;279:E684–E694. doi: 10.1152/ajpendo.2000.279.3.E684. [DOI] [PubMed] [Google Scholar]
- 39.Aycicek A, Iscan A. The effects of carbamazepine, valproic acid and phenobarbital on the oxidative and antioxidative balance in epileptic children. Eur Neurol. 2007;57:65–69. doi: 10.1159/000098053. [DOI] [PubMed] [Google Scholar]
- 40.Evans JL, Goldfine ID, Maddux BA, Grodsky GM. Are oxidative stress-activated signaling pathways mediators of insulin resistance and beta-cell dysfunction? Diabetes. 2003;52:1–8. doi: 10.2337/diabetes.52.1.1. [DOI] [PubMed] [Google Scholar]
- 41.Meeker RB, Myers RD. GABA and glutamate: possible metabolic intermediaries involved in the hypothalamic regulation of food intake. Brain Res. 1980;5:253–259. [Google Scholar]
- 42.McGarry JD. Banting lecture 2001: dysregulation of fatty acid metabolism in the etiology of type 2 diabetes. Diabetes. 2002;51:7–18. doi: 10.2337/diabetes.51.1.7. [DOI] [PubMed] [Google Scholar]
- 43.Yoshikawa H, Tajiri Y, Sako Y, Hashimoto T, Umeda F, Nawata H. Effects of free fatty acids on beta-cell functions: a possible involvement of peroxisome proliferator-activated receptors alpha or pancreatic/duodenal homeobox. Metabolism. 2001;50:613–618. doi: 10.1053/meta.2001.22565. [DOI] [PubMed] [Google Scholar]
- 44.Wong HY, Chu TS, Lai JC, Fung KP, Fok TF, Fujii T, Ho YY. Sodium valproate inhibits glucose transport and exacerbates Glut1-deficiency in vitro. J Cell Biochem. 2005;96:775–785. doi: 10.1002/jcb.20555. [DOI] [PubMed] [Google Scholar]
- 45.Verrotti A, Manco R, Agostinelli S, Coppola G, Chiarelli F. The metabolic syndrome in overweight epileptic patients treated with valproic acid. Epilepsia. 2010;51:268–273. doi: 10.1111/j.1528-1167.2009.02206.x. [DOI] [PubMed] [Google Scholar]
- 46.Luef GJ, Waldmann M, Sturm W, Naser A, Trinka E, Unterberger I, Bauer G, Lechleitner M. Valproate therapy and nonalcoholic fatty liver disease. Ann Neurol. 2004;55:729–732. doi: 10.1002/ana.20074. [DOI] [PubMed] [Google Scholar]
- 47.Luef G, Rauchenzauner M, Waldmann M, Sturm W, Sandhofer A, Seppi K, Trinka E, Unterberger I, Ebenbichler CF, Joannidis M, et al. Non-alcoholic fatty liver disease (NAFLD), insulin resistance and lipid profile in antiepileptic drug treatment. Epilepsy Res. 2009;86:42–47. doi: 10.1016/j.eplepsyres.2009.04.004. [DOI] [PubMed] [Google Scholar]
- 48.Ortiz-Sáenz de Santa María R, Santiago-Fernández C, Cano-Del Pozo M, Pérez-Gil O, Soto-Alvarez MI, Barriuso-Pérez E, Moche-Loeri JA. [Treatment with valproate and hepatic steatosis] Rev Neurol. 2005;41:766–767. [PubMed] [Google Scholar]
- 49.Verrotti A, Di Marco G, la Torre R, Pelliccia P, Chiarelli F. Nonalcoholic fatty liver disease during valproate therapy. Eur J Pediatr. 2009;168:1391–1394. doi: 10.1007/s00431-009-0927-y. [DOI] [PubMed] [Google Scholar]
- 50.Verrotti A, Agostinelli S, Parisi P, Chiarelli F, Coppola G. Nonalcoholic fatty liver disease in adolescents receiving valproic acid. Epilepsy Behav. 2011;20:382–385. doi: 10.1016/j.yebeh.2010.12.012. [DOI] [PubMed] [Google Scholar]
- 51.Saleh DA, Ismail MA, Ibrahim AM. Non alcoholic fatty liver disease, insulin resistance, dyslipidemia and atherogenic ratios in epileptic children and adolescents on long term antiepileptic drug therapy. Pak J Biol Sci. 2012;15:68–77. doi: 10.3923/pjbs.2012.68.77. [DOI] [PubMed] [Google Scholar]