

Abstract
“Beauty is in the mind of the beholder, each mind perceives a different beauty” famously said by writer Margeret Wolfe Hungerford. A beautiful smile is a gateway to the world. The aim of this article was to identify the criteria for designing the perfect smile. It was determined, smile design is a multifactorial process and various steps are involved in designing a radiant smile.
KEY WORDS: Arc, buccal corridor, smile
Dale carnegie said that one of the most important way to win friends and influence friends and people is to smile.[1] An attractive, well-balanced smile can be a personal asset.[2] When a person senses happiness, pleasure, humor or greetings, a smile develops. Webster defines the smile as “a change of facial expression involving a brightening of the eyes, an upward curving of the corners of the mouth with no sound and less muscular distortion of the features than in a laugh that may express amusement, pleasure, tender affection, approval, restrained mirth, irony, derision or any of various other emotions.”
The success of smile design is determined by the patient's soft-tissue limitations and the extent to which orthodontics or multidisciplinary treatment can satisfy the patient's and orthodontist's esthetic goals. Classical cultures of Greece and Rome based their standards of beauty on set rules of proportions and compositions.
Divine Proportion
The Greek art and literature gave importance on divine proportion or the golden ratio which is often associated with esthetics and harmony in many fields like architecture, sculpture, music, human face etc., [Figure 1]. Phythagoras, a Greek sculptor, used the golden ratio so often in his work that the number 1.618 (golden ratio) was given the name phi.[3]
Figure 1.

Sunflower, e.g., of the golden proportion
Lombardi was a pioneer in use of golden proportion in dentistry. He described the use of a “repeated ratio” in the maxillary anterior teeth which implies that an optimized dentofacial composition of the width of lateral to central incisor width and the canine to lateral incisor are repeated in proportion.
Levin devised a grid to evaluate and develop harmonious proportions of teeth. The Golden proportion for each tooth was 62% of the adjacent teeth.[4] The golden percentage was calculated by dividing the width of each central incisor, lateral incisor, and canine by the total width of all six maxillary anterior teeth and multiplying the resulting value by 100.[5,6]
Anatomy of the Smile
Smile emanates from the facial movements and is the clear manifestation of the facial structures. The perioral musculature can be classified into three groups:
Group I muscles: Buccinator, orbicularis oris, levator anguli oris, depressor anguli oris, risorius, zygomaticus major
Group II muscles: Levator labii superioris, levator labii superioris alaeque nasi, zygomaticus minor
Group III muscles: Depressor labii inferioris, mentalis, platysma.
Group I muscles insert into the modiolus, Group II muscles inserted into the upper-lip, and Group III muscles insert into lower-lip.
The upper and lower lips frame the display zone of the smile [Figure 2]. Within this framework, the components of the smile are the teeth and the gingival scaffold. The main effectors of the smile are the zygomaticus major muscles which insert into the modiolus of the orbicularis oris at each corner of the mouth.
Figure 2.
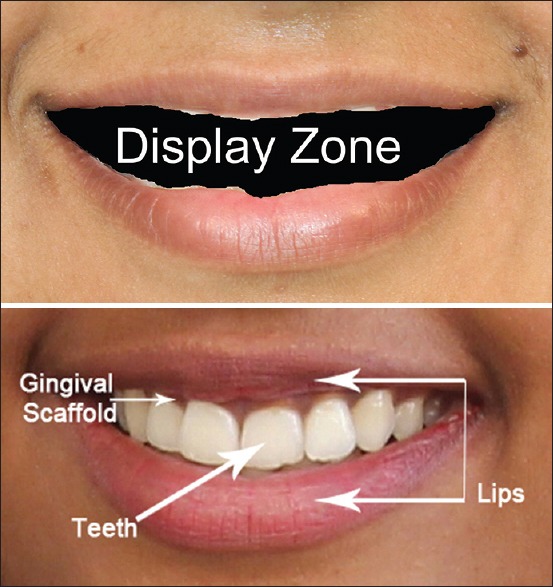
Smile components
The soft-tissue determinants of the display zone are lip thickness, interlabial gap, intercommissure width, smile index (width/height), gingival architecture.[7]
Muscular Basis of Smile
Rubin et al. have identified the nasolabial fold as the keystone of the smiling mechanism. They stated that a smile is formed in two stages. In the first stage, the levator muscles contract and raise the upper lip to nasolabial fold. In the second stage, the levator labii superioris, zygomaticus major, and buccinator muscles raise the lips even more superiorly. The final stage if often characterized by appearance of squinting. It represents the contraction of the periocular musculature to support maximum upper-lip elevation through the fold.
Classification of Smile
Many authors have classified smile into different types, e.g. Ackerman et al. classified smile into two basic types: The social smile/posed smile which is reproducible, voluntary. The lips part due to moderate muscular contraction of the lip elevator muscles, and the teeth and sometimes, the gingival scaffold are displayed; the enjoyment smile/unposed smile/Duchenne smile, is an involuntary smile and is elicited by laughter or great pleasure and results from maximal contraction of the elevator and depressor muscles causing full expansion of the lips, gingival show, and maximum anterior tooth display [Figure 3].[7,8]
Figure 3.

Social smile enjoyment smile
Tjan[2] classified smile into high smile where complete length of incisors is exhibited along with some amount of gingival display [Figure 4]. In average smile, 75–100%of upper incisors and inter dental papilla is displayed [Figure 5].
Figure 4.

High smile
Figure 5.

Average smile
In low smile line, <75% of the maxillary incisors in the full smile is displayed [Figure 6].
Figure 6.

Low smile
Rubin[9] classified three styles of smile depending on the direction of elevation and depression of the lips and the predominant muscle groups involved. He stated that in Commissure smile, the zygomaticus major muscles pull the upper-lip like a Cupid's bow. This is referred as the Mona Lisa smile. In the canine smile, the upper-lip is elevated uniformly like a diamond without the corners of the mouth turning upward. In the complex smile/full denture smile, the upper-lip moves superiorly as in the canine smile, but the lower-lip also moves inferiorly.
Records in the Treatment of Smile
Orthodontic records fall into three separate categories which provide the information and documentation required in the treatment planning regimen. They are: (1) Static records (2) dynamic records,[3] direct biometric measurement static records include photographs, radiographs, and study casts. Digital photography captures the facial images like frontal at rest, frontal smile, oblique facial smile (for evaluation of occlusal plane, palatal cant, overjet etc.), close-up oblique smile (for assessment of crown height, gingival architecture), and profile smile.
The dynamic recordings of smile and speech are accomplished through the use of digital videography where it is taken in frontal and oblique dimension. Digital video and computer technology captures around 30 frames/s. Ackerman et al. developed Smile mesh, computer software to analyze photographs of posed smiles and test the reproducibility and reliability of the smile. Three smile images of the patient are taken and the software measures 15 attributes of the smile such as the upper lip drape, maxillary incisor display, interlabial gap, buccal corridor ratio, maxillary midline offset, and intercommissure width in the frontal plane [Figure 7].[7,10]
Figure 7.

Smile mesh
Direct Biometric Measurement
Direct measurement[11] permits the clinician to quantify resting and dynamic lip – tooth relationships. The measurements such as philtrum height, commissure height, interlabial gap, amount of incisor show at rest, amount of incisor display on smile, crown height, gingival display, smile arc are done.
The philtrum height is measured in millimeters from subspinale (the base of the nose at the midline) to the most inferior portion of the upper lip on the vermilion tip beneath the philtral columns. Commissure height is measured from a line constructed from the alar bases through subspinale and then from the commissures perpendicular to this line. The differential lip growth exhibits as the difference in height in phlitrum and commissural height in adolescents. The interlabial gap is measured as the distance in millimeters between the upper and lower lips when lip incompetence is present.
Crown height is the vertical height of the maxillary central incisors; crown height is normally between 9 and 12 mm in adults (10.6 mm in men and 9.6 mm in women).
The amount of gingival display on smile and the incisor display, along with crown height, helps the deciding how much tooth movement is required to improve the smile index. A gummy smile is often more esthetic than a smile with less tooth display.
The smile arc from the frontal view is the relationship of the curvature of the incisal edges of the maxillary incisors and canines to the curvature of the lower lip in the posed social smile. In an ideal smile arc or in consonant smile, the curvature of the maxillary incisal edge is parallel to the curvature of the lower lip upon smile; in a nonconsonant or flat smile, the maxillary incisal curvature is flatter than the curvature of the lower lip on smile.
Smile Analysis
Smile analysis is traditionally performed in the frontal, oblique, sagittal dimension, and with time.
Ackerman and Ackerman developed a ratio called the smile index (inter commissural width/interlabial gap), to visualize and quantify the frontal smile. The ratio is used for comparing smiles among patients. The lower the smile index, the less youthful the smile appears.
In the oblique view, the contour of the maxillary occlusal plane is noted. The maxillary occlusal plane should be in consonant with the curvature of the lower lip on smile. In sagittal dimension, overjet and incisor angulations are best visualized. Orthodontic correction of overjet involves macro-elements, such as jaw patterns and soft-tissue elements like nasal projection.
According to time, orthodontic patients can be categorized as a preadolescent, adolescent, and adult. The growth, maturation, and aging of the perioral soft-tissues have a profound effect on the appearance of both resting and smiling presentations. Orthodontic cephalometric research indicates that on average, profiles flatten over time.[12]
Components of Smile
Hulsey concluded that a key component present in an esthetic smile was a consonance between the arcs formed between the incisal edges of the maxillary anterior teeth and the curvature of the lower lip.
Various components of a balanced smile are lip line, buccal corridor, smile arc, upper-lip curvature, smile symmetry, frontal occlusal plane, dental components, gingival components
The lip line is the amount of vertical tooth exposure in smiling, that is, the height of the upper-lip relative to the maxillary central incisors.[13,14] It depends on various factors.
In general, female lip lines are an average 1.5 mm higher than male lip lines[15] and with aging, there is a gradual decrease in exposure of the maxillary incisors at rest and to a much lesser degree, in smiling. The upper lip length at rest is about 23 mm in males and 20 mm in females.[12] When the upper-lip is elevated, it displays about 80% of its original length. If a gingival smile is caused by a hypermobile lip, intrusion or impaction surgery would decrease the amount of gingival display and makes the patient look older. When upper-lip length and mobility are normal, a gingival smile with excessive incisor display at rest can be attributed to vertical maxillary excess which is often associated with excessive lower facial height.
The average vertical crown height of the maxillary central incisor is 10.6 mm in males and 9.8 mm in females[15] and a short crown may be due to attrition or excessive gingival encroachment. When all other factors are equal, the incisor exposure at rest determines the vertical position of the incisal edge. Therefore, a deep bite should be corrected by maxillary incisor intrusion in a patient with excessive incisor display at rest and with posterior extrusion and/or lower incisor intrusion in a patient with a normal lip line at rest. An open bite case should be corrected by maxillary incisor extrusion if there is inadequate incisor display at rest, but with the posterior intrusion and/or lower incisor extrusion if the lip line is normal at rest.
Incisor inclination also plays a role in the lip line. Ricketts noted that the upper-lip thickened as the upper incisor was retracted and gave a rule of thumb of 1 mm increase in thickness of the lip for every 3 mm of retraction of the tips of the incisors.
The buccal corridor is the space created between the buccal surface of the posterior teeth and the lip corners when the patient smiles.[14] Orthodontists refer to buccal corridors as “negative" spaces. It is measured from the mesial line angle of the maxillary first premolars to the interior portion of the commissure of the lips. The negative space is affected by the smile, the maxillary arch width, the facial muscles, the position of the buccal surfaces of the posterior maxillary teeth, etc.[12,16] Moore et al. stated that when the buccal corridor is of 28% as medium-narrow, 15% as medium, 10% as medium-broad, and 2% as broad smile fullness.
The smile arc is the relationship between a hypothetical curve drawn along the edges of the maxillary anterior teeth and the inner contour of the lower lip in the posed smile.[14,16,17] The curvature of the incisal edges appears to be more pronounced for women than for men and tends to flatten with age.[7] The archform and the maxillary anterior occlusal plane influence the degree of curvature of the smile arc. The smile arc can be unintentionally flattened during orthodontic treatment by any or all of the following three techniques such as over intrusion of maxillary incisors, improper bracket positioning, and the cant of the occlusal plane. Other factors that can affect the smile arc are attrition due to shortening of the central incisors, habits such as thumb sucking, excessive posterior vertical growth, and the lower-lip musculature.
The upper-lip curvature is assessed from the central position to the corner of the mouth in smiling. Upward and straight lip curvatures are considered more esthetic than downward lip curvatures.[9]
Smile symmetry is the relative positioning of the corners of the mouth in the vertical plane which can be assessed by the parallelism of the commissural and pupillary lines.[18] Myofunctional appliances are recommended when there is a large differential elevation of the upper-lip due to a deficiency of muscular tonus on one side of the face.
The frontal occlusal plane is represented by a line running from the tip of the right canine to the tip of the left canine. A transverse cant can be caused by differential eruption of the maxillary anterior teeth or a skeletal asymmetry of the mandible[12] which can be diagnosed by asking the patient to bite on a tongue blade or a mouth mirror in the premolar area during the clinical examination.
Dental components of the smile include the size, shape, color, and alignment, crown angulations of the teeth, the midline and arch symmetry. Factors that can disturb the continuity of the dental composition include midline diastema and lack of inter proximal contacts.
The gingival components of the smile are the color, contour, texture, and height of the gingiva. Inflammation, blunted papillae, open gingival embrasures (black triangle), and uneven gingival margins detract from the esthetic quality of the smile. The space created by a missing papilla above the central incisor contact point, referred to as a “black triangle,” may be caused by root divergence, triangular teeth, or advanced periodontal disease. Orthodontic root paralleling and flattening of the mesial surfaces of the central incisors, followed by space closure, will lengthen this contact area and move it apically toward the papilla.[13]
Conclusion
In our modern competitive society, a charming smile can open doors and knock down barriers that stand between us and a fuller, richer life. It must be understood that there is no universal “ideal” smile. The most important esthetic goal in orthodontics is to achieve a “balanced” smile. The components of the smile should be considered not as rigid boundaries but as artistic guidelines to help the orthodontist to treat individual patients. It is important for orthodontists to make every effort to develop a harmonious balance that will produce the most attractive smile possible for each patient being treated.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Carnegie D. United States: Simon and Schuster; 1936. How to Win Friends and Influence People. [Google Scholar]
- 2.Tjan AHL, Miller GD. The JGP. Some esthetic factors in a smile. J Pros Dent. 1984;51:24–28. doi: 10.1016/s0022-3913(84)80097-9. [DOI] [PubMed] [Google Scholar]
- 3.Ahmad I. Anterior dental aesthetics: Historical perspective. Br Dent J. 2005;198:737–42. doi: 10.1038/sj.bdj.4812411. [DOI] [PubMed] [Google Scholar]
- 4.Murthy BV, Ramani N. Evaluation of natural smile: Golden proportion, RED or Golden percentage. J Conserv Dent. 2008;11:16–21. doi: 10.4103/0972-0707.43413. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Ali Fayyad M, Jamani KD, Agrabawi J. Geometric and mathematical proportions and their relations to maxillary anterior teeth. J Contemp Dent Pract. 2006;7:62–70. [PubMed] [Google Scholar]
- 6.Ricketts RM. The biologic significance of the divine proportion and Fibonacci series. Am J Orthod. 1982;81:351–70. doi: 10.1016/0002-9416(82)90073-2. [DOI] [PubMed] [Google Scholar]
- 7.Ackerman MB, Ackerman JL. Smile analysis and design in the digital era. J Clin Orthod. 2002;36:221–36. [PubMed] [Google Scholar]
- 8.Ritter DE, Gandini LG, Jr, Pinto Ados S, Ravelli DB, Locks A. Analysis of the smile photograph. World J Orthod. 2006;7:279–85. [PubMed] [Google Scholar]
- 9.Rubin LR, Mishriki Y, Lee G. Anatomy of the nasolabial fold: The keystone of the smiling mchanism. Plast Reconst Surgery. 1989;83:1–8. doi: 10.1097/00006534-198901000-00001. [DOI] [PubMed] [Google Scholar]
- 10.Schabel BJ, Baccetti T, Franchi L, McNamara JA. Clinical photography vs digital video clips for the assessment of smile esthetics. Angle Orthod. 2010;80:490–6. doi: 10.2319/052207-243.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Sarver DM, Ackerman MB. Dynamic smile visualization and quantification: Part 1. Evolution of the concept and dynamic records for smile capture. Am J Orthod Dentofacial Orthop. 2003;124:4–12. doi: 10.1016/s0889-5406(03)00306-8. [DOI] [PubMed] [Google Scholar]
- 12.Sarver DM, Ackerman MB. Dynamic smile visualization and quantification: Part 2. Smile analysis and treatment strategies. Am J Orthod Dentofacial Orthop. 2003;124:116–27. doi: 10.1016/s0889-5406(03)00307-x. [DOI] [PubMed] [Google Scholar]
- 13.Sabri R. The eight components of a balanced smile. J Clin Orthod. 2005;39:155–67. [PubMed] [Google Scholar]
- 14.Mackley RJ. An evaluation of smiles before and after orthodontic treatment. Angle Orthod. 1993;63:183–9. doi: 10.1043/0003-3219(1993)063<0183:AEOSBA>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 15.Peck S, Peck L, Kataja M. Some vertical lineaments of lip position. Am J Orthod Dentofacial Orthop. 1992;101:519–24. doi: 10.1016/0889-5406(92)70126-U. [DOI] [PubMed] [Google Scholar]
- 16.Sarver DM. The importance of incisor positioning in the esthetic smile: The smile arc. Am J Orthod Dentofacial Orthop. 2001;120:98–111. doi: 10.1067/mod.2001.114301. [DOI] [PubMed] [Google Scholar]
- 17.Burstone CJ. Lip posture and its significance in treatment planning. Am J Orthod. 1967;53:262–84. doi: 10.1016/0002-9416(67)90022-x. [DOI] [PubMed] [Google Scholar]
- 18.Janzen EK. A balanced smile – a most important treatment objective. Am J Orthod. 1977;72:359–72. doi: 10.1016/0002-9416(77)90349-9. [DOI] [PubMed] [Google Scholar]