

Abstract
Gestational Diabetes mellitus is the condition of glucose intolerance that begins during pregnancy which is associated with both fetal and maternal complications. The measurement of serum fructosamine and glycated hemoglobin in normal and diabetic pregnancy used to investigate the influence of maternal and gestational age on concentrations of glycated proteins in serum and used to evaluate the patient's treatment. This study was done to measure the level of serum fructosamine and Glycated hemoglobin (HbA1c) in Gestational Diabetes mellitus (GDM) patients and to compare with pregnant women without diabetes and healthy non-pregnant adults, to determine the pattern of change in serum fructosamine, influence of serum fructosamine and HbA1c values and to evaluate the efficacy of patient's treatment. In this study the level of fructosamine was positively correlated to HbA1c during 2nd trimesters of gestational period, implying that the level of fructosamine can be used to screen Gestational diabetes mellitus. Correlation of glycated hemoglobin values with serum fructosamine measurements in the accurate determination of glycaemic control provides confirmation of the utility of fructosamine measurement.
KEY WORDS: Fructosamine, gestational diabetes mellitus, glycated hemoglobin
Diabetes mellitus (DM) is as a metabolic disorder of multiple etiologies characterized by chronic hyperglycemia due to defects in insulin secretion, insulin action, or both. Gestational diabetes, defined as “Carbohydrate intolerance of variable severity with onset or first recognition during pregnancy,” existed as a concept as early as 1946 and was invoked to explain high perinatal mortality rates in pregnancies of women who subsequently developed diabetes.[1]
Women with gestational diabetes mellitus (GDM) have a greater incidence of insulin resistance compared with the insulin resistance seen in normal pregnancies. They also have an impairment of the compensatory increase in insulin secretion; particularly first-phase insulin secretion and this may be a marker for deterioration of β-cell function. Gestational diabetes affects 1-3% of all pregnant women. Prevalence of GDM varies worldwide and among different racial and ethnic groups within a country. The prevalence of GDM in American - white women has been found to be 3.9% and among Asian women it was found to be 8.7%. In Europe the prevalence has been found to be 0.6-3.6%, in Australia 3.6-4.7% (Indian women - 17.7%) and in China the prevalence has been found to be 2.3% compared with 2.9% in Japan.
Gestational diabetes is a treatable condition and women who have adequate control of glucose levels can effectively decrease these risks. The present study was designed to measure the level of serum fructosamine and glycated hemoglobin (HbA1c) in GDM patients and pregnant women without diabetes and to compare with healthy nonpregnant adults. Also to determine the pattern of change in serum fructosamine, and the significance of serum fructosamine and HbA1c values in GDM patients so as to improve the diagnosis and to evaluate the efficacy of patient's treatment.
Materials and Methods
The Study was conducted at SRM Medical College Hospital and Research Centre, Kattankulathur. Study group consisted of 25 patients of pregnant women with diabetes, 25 pregnant women without diabetes and 25 healthy adult volunteers control were between the age group 23-30 years. From each diabetic subjects as well as from controls, their medical history was obtained through a structured questionnaire and an informed consent was obtained. The inclusion criteria include subjects with body mass index of at least 30 kg/m2 and history of gestational diabetes, subjects excluded from the study were type 1 and type 2 DM women of age below 18 years and above 55 years, who were diagnosed as diabetes before pregnancy. Subjects with hepatitis, cirrhosis of liver and thyroid dysfunction were also excluded. Ethylenediaminetetraacetic acid and plain blood samples were collected from study subjects and analyzed for serum fructosamine by nitro blue tetrazolium method (NBT). Glycated hemoglobin by ion exchange resin method and random blood glucose by GOD-POD method.
Results
The study evaluated the role of fructosamine and HbA1c as a screening parameter for GDM. The mean glucose level in control subjects, pregnant women without diabetic and gestational diabetic subjects were found to be 114.5 ± 11.4, 128.12 ± 4.28 and 227.7 ± 31.4 respectively [Table 1]. The fructosamine level in control subjects, pregnant women without diabetic and gestational diabetic subjects were found to be 2.38 ± 0.17, 2.59 ± 0.06 and 4.67 ± 0.58 [Table 2]. HbA1c level in control subjects, pregnant women without diabetic and gestational diabetic subjects were found to be 5.68 ± 0.00, 5.99 ± 0.35 and 9.56 ± 1.0. The blood glucose, fructosamine and HbA1c concentrations were found to be significantly high in hyperglycemic groups (pregnant women without diabetic and gestational diabetic subjects) when compared to healthy subjects [Figure 1].
Table 1.
Level of RBG, fructosamine and HbA1c in study subjects
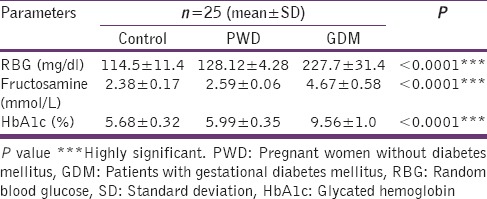
Table 2.
Correlation studies of fructosamine with other variables of blood glucose control
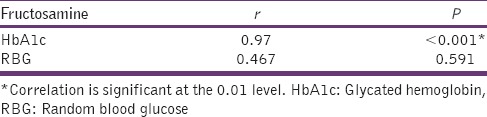
Figure 1.
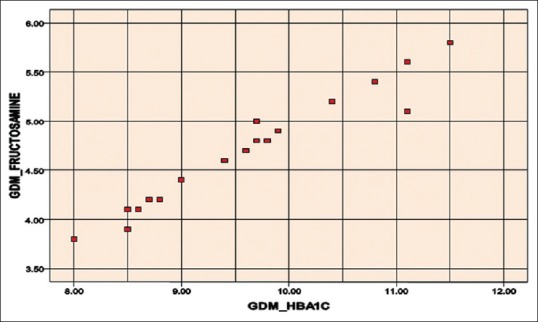
Correlation analysis of fructosamine and glycated haemoglobin (HbA1c) (correlation factor r = 0.97, coefficient of variation for GDM_FRUCTOSAMINE =12.4732, coefficient of variation for GDM_HbA1c =10.5539). GDM: Gestational diabetes mellitus
Correlation analysis
It is well-known that random blood glucose measurements are relatively poor measure of glycemic control.[2] Hence, the correlation for fructosamine or HbA1c to random blood sugar was not found to be significant.
Serum fructosamine level correlated significantly with glycated hemoglobin concentrations (r = 0.97, P < 0.001) in GDM patients compared with healthy control groups. This correlation also provides confirmation of the utility of fructosamine measurement. In this study, the level of fructosamine was positively related to HbA1c during the second trimester of gestational period and was performed on diabetic subjects whose blood glucose value was >120 mg/dl, implying that the level of fructosamine can be used to screen GDM. Serum fructosamine level was not found to be affected by hemoglobin variations or decreasing hemoglobin half-life.
Sensitivity and relative lack of preanalytical interference offer strong evidence that fructosamine assay can be a useful screen for diabetes.
GDM_FRUCTOSAMINE is more consistent. Serum fructosamine concentration correlated significantly with HbA1c concentrations (r = 0.97, P < 0.000). There is a significant difference between fructosamine and HbA1c in the GDM patients and healthy control groups (P < 0.0001).
Discussion
Fructosamine and glycohemoglobin are both used to monitor diabetic control. Each assay provides information for a specific time frame that is related to the analyte being measured. Since the life span of hemoglobin is closer to 6-8 weeks, a glycohemoglobin measurement reflects the average glucose concentration over this longer period.[3] Fructosamine explains the short-term diabetic control as opposed to the longer term for glycohemoglobin.
Chronic hyperglycemia may be the cause of vascular complications of DM, and methods of accurate assessment of glycemic control should be encouraged. The fructosamine assay has been found to be more sensitive than random glucose measurement for glycemic control determinations and contributed a different view of glycemia than that of HbA1c. Since the half-life of albumin and other serum proteins is considerably shorter than that of hemoglobin, the concentration of fructosamine levels can change more rapidly than those of HbA1c.
Fructosamine is measured bichromatically as an end-point reaction based on the ability of glycated proteins to reduce NBT in an alkaline solution. The test requires a small sample volume, and results are resistant to the effects of storage and heat on the specimens. Fructosamine's intermediate picture of glycemic control coupled with confirmation by HbA1c gives a dynamic advantage to both tests and increases the predictive value of the blood profile for glucose intolerance. Samples for fructosamine assay require no pretreatment, and the fructosamine assay has been found to be less expensive than HbA1c assay.
Lower HbA1c levels were observed in diabetic and nondiabetic pregnant women, probably due to lower fasting blood glucose and also a shortened erythrocyte lifespan[4] Vitamins C and E have been reported to lower HbA1c measurements, possibly by inhibiting glycation. Concomitant use of many drugs to treat patients with malignancies, human immunodeficiency virus or hepatitis C virus infection, may have a glycated hemoglobin lowering effect and produce a negative result in the patients with diabetes. Alcoholism, lipidemia, and chronic ingestion of salicylates may also reduce the level of HbA1c.[5]
Glycated hemoglobin levels higher than expected values can be seen in people with a longer red blood cell life span, due to Vitamin B12 or folate deficiency. Kilpatrick et al. has shown evidence of wide fluctuations in HbA1c between individuals that are unrelated to glycemic status, suggesting that there are “low glycators” and “high glycators.”[6] In a study where the HbA1c and fructosamine levels were simultaneously measured, the HbA1c does not accurately reflect glucose control and hence it was suggested that the fructosamine measurement may be routinely used in diabetes practice.[7]
Fructosamine's intermediate picture of glycemic control coupled with conformation by HbA1c gives a dynamic advantage to both tests and increases the predictive value of the blood profile for glucose intolerance. Automation, adaptability, sensitivity and relative lack of the preanalytical interference offer strong evidence that fructosamine analysis may be a useful screen for diabetes and benefit to the proper treatment process.
Conclusion
The present study indicates that the importance of glycemic control during pregnancy through the proper diagnosis of Gestational diabetic patients. This clinical data tend to support the concept that fructosamine assay can provide a good index of glycemic control especially in diabetic pregnant patients. Due to the reliability, technical simplicity, low cost, and reduced analytical time of the fructosamine assay, it can be considered as alternative choice for first - line monitoring of diabetic patients and the fructosamine determination is more consistent when compared to HbA1c. The fructosamine determines the average glucose over the past 2-3 weeks and the assay is not affected by the food eaten during the day. Hence, fructosamine can be measured at any time during the day. It may be a very useful clinical adjunct and indicator for monitoring glycemic control in gestational diabetic patients.
Acknowledgments
I sincerely thank my guide, head of the department and my colleagues for their guidance and constant support throughout my study.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.American Diabetes Association. Position statement-gestational diabetes. Diabetes Care. 1986;9:430–1. [PubMed] [Google Scholar]
- 2.American Diabetes Association. Diabetes Care. 2014;37(Suppl 1):S81–90. doi: 10.2337/dc14-S081. [DOI] [PubMed] [Google Scholar]
- 3.American Diabetes Association. Standards of medical care in diabetes. Diabetes Care. 2004;27:S15–35. doi: 10.2337/diacare.27.2007.s15. [DOI] [PubMed] [Google Scholar]
- 4.Makris K, Spanou L. Is there a relationship between mean blood glucose and glycated hemoglobin? J Diabetes Sci Technol. 2011;5:1572–83. doi: 10.1177/193229681100500634. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Sultanpur CM, Deepa K, Kumar SV. Comprehensive review on HbA1c in diagnosis of diabetes mellitus. International Journal of Pharmaceutical Sciences Review and Research. 2010;3:119–22. [Google Scholar]
- 6.Kilpatrick ES, Maylor PW, Keevil BG. Biological variation of glycated hemoglobin. Implications for diabetes screening and monitoring. Diabetes Care. 1998;21:261–4. doi: 10.2337/diacare.21.2.261. [DOI] [PubMed] [Google Scholar]
- 7.Macdonald DR, Hanson AM, Holland MR, Singh BM. Clinical impact of variability in HbA1c as assessed by simultaneously measuring fructosamine and use of error grid analysis. Ann Clin Biochem. 2008;45:421–5. doi: 10.1258/acb.2008.007259. [DOI] [PubMed] [Google Scholar]