

Abstract
The umbilical cord usually contains two arteries and one vein. The vein carries the oxygenated blood from the placenta to the fetus. The arteries carry the deoxygenated blood and the waste products from the fetus to the placenta. Occasionally, primary agenesis or secondary atrophy of one of the arteries occurs resulting in single umbilical artery.
KEY WORDS: Congenital anomalies, single umbilical artery, two vessel umbilical cord
Case Report
We are presenting a newborn baby born with an isolated single umbilical artery (SUA). Second trimester ultrasound done at 27 weeks showed a SUA and there were no other associated anomalies in the fetus as well as in the placenta. The mother was counseled and closely followed up. The mother had pregnancy induced hypertension and anemia complicating pregnancy. Baby was delivered by emergency cesarean section at 36 weeks of gestation. The indication for C-section was premature rupture of membranes and fetal distress. Baby cried immediately after birth. This was a preterm female baby with a birth weight of 2.2 kg. On examination, the baby was normal, and there were no dysmorphic features or obvious congenital anomalies. The ultrasound abdomen done on day 3 of life showed no anomalies. Both the kidneys were normal. Echocardiography was done as part of routine screening in such babies. There was a small patent foramen ovale. The mother was reassured. The karyotype was done and it was reported normal. The baby is now 1-month old and was brought for review. She is feeding well and gaining weight. Her present weight is 2.6 kg [Figures 1 and 2].
Figure 1.
Cut section-umbilical cord of the baby
Figure 2.
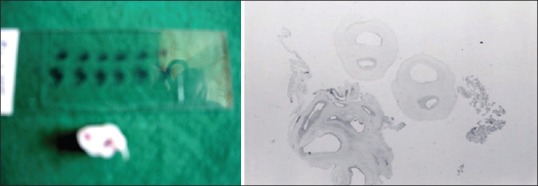
Two vessel cord of the baby-macroscopic and microscopic view
Discussion
The incidence of SUA varies from 0.2% to 0.87%.[1] It is more common in multiple pregnancies. Prenatal ultrasound evaluation for SUA should be done during the second and third trimester of pregnancy.[2] In this case, the second trimester ultrasound which was done at 27 weeks showed a SUA with no other associated anomalies. Isolated SUA is a risk factor for adverse pregnancy outcome. There is an increased risk of intrauterine and intrapartum deaths among fetuses with SUA.[3] There is also an increased risk of intrauterine growth restriction, prematurity and mortality among neonates with SUA when compared with those with a three-vessel cord.[3,4] This baby was also born premature with a low birth weight.
Neonates with SUA are at a higher risk of congenital anomalies and chromosomal abnormalities. The most common congenital anomalies associated with SUA are renal, followed by cardiovascular and musculoskeletal.[3] Screening renal ultrasonography done in our baby was reported to be normal.
Neonates with SUA have a 15 times higher risk of chromosomal abnormalities.[3] However, SUA can also be an isolated finding. Fortunately, this newborn had no congenital anomalies.
A significant proportion of infants with isolated SUA may have occult renal malformations like vesico-ureteric reflux (VUR) grade 2 or more.[5] Hence, these infants need to be followed up regularly, and we need to maintain a low threshold for diagnosing and managing urinary tract infections (UTIs). Once the UTI is treated a micturating cystourethrogram needs to be done to rule out VUR. We are planning to follow up this baby based on the above recommendations.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Vasanthalakshmi GN, Pushpalatha T, Mehta P, Devi SA. Single umbilical artery and pregnancy outcomes: Cause for concern. J S Asian Fed Obstet Gynaecol. 2012;4:103–5. [Google Scholar]
- 2.Chow JS, Benson CB, Doubilet PM. Frequency and nature of structural anomalies in fetuses with single umbilical arteries. J Ultrasound Med. 1998;17:765–8. doi: 10.7863/jum.1998.17.12.765. [DOI] [PubMed] [Google Scholar]
- 3.Murphy-Kaulbeck L, Dodds L, Joseph KS, Van den Hof M. Single umbilical artery risk factors and pregnancy outcomes. Obstet Gynecol. 2010;116:843–50. doi: 10.1097/AOG.0b013e3181f0bc08. [DOI] [PubMed] [Google Scholar]
- 4.Leung AK, Robson WL. Single umbilical artery. A report of 159 cases. Am J Dis Child. 1989;143:108–11. doi: 10.1001/archpedi.1989.02150130118030. [DOI] [PubMed] [Google Scholar]
- 5.Srinivasan R, Arora RS. Do well infants born with an isolated single umbilical artery need investigation? Arch Dis Child. 2005;90:100–1. doi: 10.1136/adc.2004.062372. [DOI] [PMC free article] [PubMed] [Google Scholar]