

Abstract
The use of light and laser in the treatment of acne is increasing as these modalities are safe, effective, and associated with no or minimal complications when used appropriately. These light and laser sources are also being used in combination with pharmacological and/or physical measures to synergize their effects and optimize the therapeutic outcome. This review focuses on optical devices used in treating acne and serves to delineate the current application of various methods, including their utility and efficacy.
Keywords: Acne, blue light, intense pulse light sources, laser, photodynamic therapy, photopneumatic therapy
INTRODUCTION
Acne vulgaris is a chronic inflammatory disorder of the pilosebaceous unit affecting more than 85% of adolescents and often persisting into later adulthood.[1] Conventional therapy with antibiotics and retinoids yield mixed results and can be complicated by antibiotic resistance and adverse treatment profiles. Therefore, newer therapeutic modalities such as light-based therapy have been developed to address the need for acne treatment. A variety of narrowband light sources, intense pulsed light (IPL), lasers, and photodynamic therapy (PDT) have been studied. Treatment with these light sources may offer improvements in inflammatory acne and acne scarring, with more limited benefit for noninflammatory (comedonal) acne.
Mechanism of action of light-based therapies
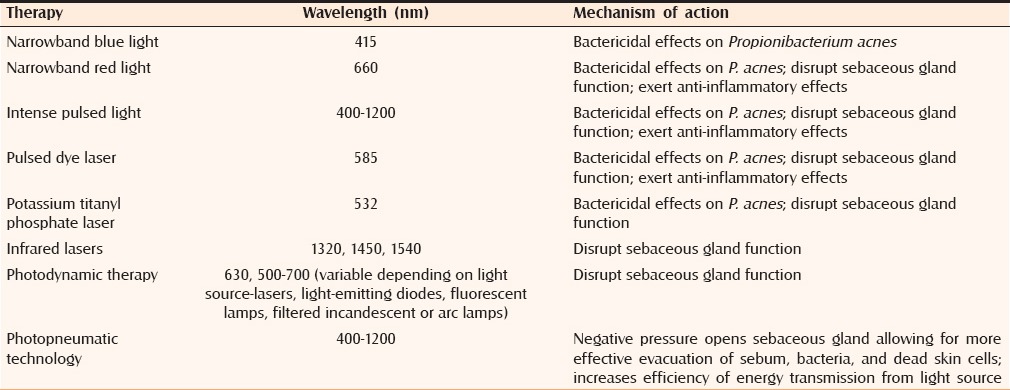
Previous clinical observations and studies have shown that patients experience acne improvement after exposure to natural sunlight but the specific mechanism had not been elucidated.[2] More recently, it has been postulated that light-based therapies work to decrease Propionibacterium acnes level and reduce pilosebaceous unit size and function.[3] Specifically, light is absorbed by porphyrins produced naturally within sebaceous follicles by P. acnes.[4,5] Porphyrins (coproporphyrin III and protoporphyrin IX) absorb light wavelengths between 400 and 700 nm with 415 nm wavelength within the blue light spectrum being most effectively absorbed. Light absorption leads to photo-excitation of porphyrins and subsequent release of singlet oxygen and reactive free radicals that exert bactericidal effects on P. acnes. Longer wavelengths, such as red light, activate porphyrins less effectively but penetrate deeper into the skin where it may directly target sebaceous glands and exert anti-inflammatory properties by influencing cytokine release from macrophages.[6,7] Blue light has also been shown to exert anti-inflammatory effects in keratinocytes.[8] On the other hand, therapy with infrared (IR) lasers (1320, 1450, 1540 nm) and PDT may directly cause phototoxic and photothermal damage to sebaceous glands, resulting in reduced gland size and sebum production.[3] The IPL (400–1200 nm), pulsed dye lasers (PDL, 585–595 nm) and potassium titanyl phosphate lasers (KTP, 532 nm) may also similarly disrupt sebaceous gland function through direct phototoxic and thermal damage, and/or exert bactericidal effects on P. acnes via induction of reactive free radicals [Table 1].
Table 1.
Mechanism of action of light-based therapies
Blue or blue-red light
Thiboutot et al. reviewed 8 studies published between 2000 and 2006 investigating blue light treatment of mild-to-moderate acne and found moderate evidence in support of its efficacy, especially for inflammatory lesions.[3] A systematic review of 25 randomized controlled trials of light therapies for acne up to 2007 concluded that multiple treatments with blue light, blue-red light, or IR radiation were more likely to produce successful outcomes than with yellow, green, or red light.[9]
We summarize studies investigating blue light or blue-red light for acne treatment in Table 2.[10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31] In general, high-intensity narrowband light (405–420 nm) applied for 8–20 min twice weekly for four weeks was reported to reduce inflammatory acne lesion count in the 60%–70% range; noninflammatory acne lesions were less affected. Similarly, a combination of blue-red light has been reported to reduce inflammatory lesions from 69% to 77% with more modest effect on noninflammatory lesions. Sadick reported in a small pilot study that a combination of blue (415 nm) and IR (830 nm) was less effective in reducing inflammatory acne lesions compared with blue and red light combination reported in previous studies.[25] Although most studies on blue or blue-red light were small open label trials with a small sample size, notably a more recent double-blind, randomized controlled trial comparing blue-red light therapy versus sham device in Korean patients found reductions of 77% and 54% in inflammatory and noninflammatory acne at 12 weeks after 2.5 min of twice daily use for four weeks, results that are comparable to earlier open-label trials.[26] In addition, reduced sebum production and sebaceous gland size, and attenuated inflammatory cell infiltrations were noted in the treatment group.
Table 2.
Summary of studies of blue or blue-red light treatment for acne
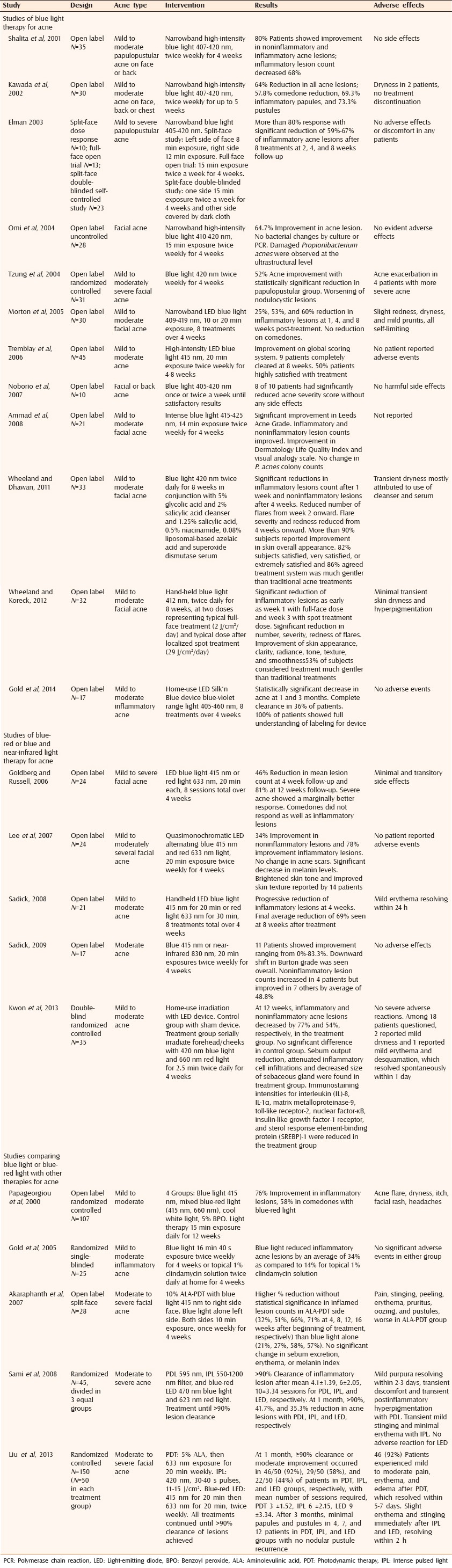
A few studies compared blue or blue-red light treatment to conventional acne therapy. However, Papageorgiou et al. reported a mean improvement of 76% in inflammatory lesions treated with blue-red light compared with benzoyl peroxide or blue light alone.[27] Another study comparing blue light therapy to 1% topical clindamycin solution found an overall 34% reduction in inflammatory acne with blue light compared with 14% for clindamycin.[28]
A few studies have compared efficacy of blue light versus other light therapies in acne clearance. Aminolevulinic acid (ALA) PDT with blue light source resulted in a higher percentage reduction of inflammatory lesions at 8, 12, and 16 weeks follow-up compared with blue light alone; however, the differences were not statistically significant.[29] Another study showed that ALA-PDT with red light source achieved ≥90% acne clearance at one month in more patients (92%) than blue-red light-emitting diode (LED, 44%) or IPL (58%). However, both IPL and LED were much better tolerated with adverse effects (slight erythema and stinging) resolving within two hours compared with PDT adverse effects (mild-to-moderate pain, erythema, and edema) that resolved within 5–7 days.[31]
Overall, the evidence suggests that blue light and blue-red light combination is effective in treating mild to moderate inflammatory acne lesions. However, more trials comparing blue and blue-red light therapy with conventional acne treatments such as topical retinoids and antibiotics, and studying their effects on severe acne are needed. In addition, longer follow-up with delineation of long-term benefits, relapse, and adverse effects would be helpful.
Intense pulsed light
IPL monotherapy
IPL (400–1200 nm) devices employ flashlamps and bandpass filters to produce polychromatic incoherent high-intensity pulsed light of determined wavelength spectrum, fluence, and pulse duration.[32] Absorption of red and blue light can activate porphyrins that reduce P. acnes growth. In addition, endogenous chromophores in the skin absorb broad spectrum light delivered by IPL to achieve damage of blood vessels supplying sebaceous glands, thus reducing sebaceous gland size and/or function. IPL may also exert an anti-inflammatory effect through downregulation of tumor necrosis factor alpha (TNF-α)[33] and upregulation of transforming growth factor-beta1 (TGF-β)/Smad3 signaling.[34] A systematic review of IPL identified 21 studies that investigated the efficacy of IPL in acne treatment.[35] Overall, reported efficacy of IPL for acne treatment ranged from 34% to 88% improvement depending on acne type (inflammatory vs noninflammatory). The level of evidence for IPL efficacy was determined to be moderate based on limiting factors such as lack of high-quality controls in randomized controlled trials.
Kumaresan et al.[36] studied the efficacy of IPL in facial acne treatment with burst-pulse and single-pulse modes of treatment. In the single-pulse mode, fluence is delivered in a single shot or pulse, whereas in the burst-pulse mode the total fluence is divided into a series of pulses with a delay between the pulses (in this case, 5 pulses with delay of 6 ms). Burst-pulse technique allows selective photothermal and phototoxic effect to targeted lesions and can potentially achieve delivery of higher cumulative light doses and selective damage. Burst-pulse technique is applicable to a wide variety of laser and IPL devices. Both single- and burst-pulse modes showed a reduction in acne severity with burst-pulse mode being slightly more efficacious (56%) than the single-pulse mode (40%). Similar promise has been shown in other studies. Kawana et al.[37] demonstrated reduction of noninflammatory and inflammatory acne to 11%–12% of baseline in Asian skin treated with IPL at 400–700 nm and 870–1200 nm. In contrast, Chang et al.[38] studied the utility of IPL equipped with a 530–750 nm filter for inflammatory acne treatment in 30 Asian female patients with mild-to-moderate acne. Results showed that this wavelength band of IPL was safe and effective in improving red macules, irregular pigmentation, and altered skin tone associated with acne but did not show significant improvement in inflammatory acne lesions.
Several studies examined the effectiveness of IPL compared with other therapeutic light modalities. Sami et al.[30] demonstrated that patients treated with IPL required a mean of six sessions to reach a ≥90% clearance of their inflammatory lesions compared with four sessions for PDL and 10 sessions for LED blue-red light. At the mid-point evaluation, the percentage reduction in acne lesions treated with the IPL was 41.7% compared with 90% for PDL and 35% for LED blue-red light. Similarly, in a randomized trial comparing IPL, PDT, and blue-red LED in Chinese subjects, Liu et al.[31] reported that 58% of subjects treated with IPL achieved ≥90% acne clearance at 1 month compared with 92% for PDT and 44% for blue-red LED. The results of these studies demonstrate IPL monotherapy as a promising treatment option for facial acne, although it is less effective compared with PDL and PDT but more effective than blue-red LED. In addition, Choi et al.[39] reported that although IPL induced initially faster and better response than PDL for inflammatory acne, it was associated with rebound aggravation after treatment termination.
A few studies have compared IPL alone versus conventional therapies. One study reported IPL to be inferior to 5% benzyl peroxide gel in treating mild to severe inflammatory acne.[40]
IPL in combination with other modalities
Most studies investigating IPL in combination with other modalities have examined IPL with a photosensitizing agent. Taub compared the effectiveness of ALA-PDT with activation by IPL (600–850 nm) versus a combination of IPL (580–980 nm) and bipolar RF versus blue light (417 nm) in treating acne vulgaris in a randomized trial.[41] Results at one month and at the end of three months showed that IPL activation of ALA-PDT provided greater, longer-lasting, and more consistent improvement than the other modalities. Santos et al.[42] have also demonstrated promising results in their study comparing ALA with IPL versus IPL monotherapy. At the end of the fourth week of their split-face study, patients showed visible improvement of facial acne that was more significant on the ALA IPL side of the face persisting until the eighth week post-treatment, whereas the side treated with IPL alone returned to baseline. Shaaban et al. compared the efficacy of intralesional ALA with IPL versus IPL monotherapy in patients with nodulocystic and inflammatory acne and found that intralesional ALA with IPL was significantly more effective in reducing both number of acne lesions and recurrence than IPL alone.[43] Mei et al. compared ALA-IPL versus IPL alone in treatment of moderate-to-severe acne in Chinese patients and reported a mean reduction of acne lesion counts of 75% in ALA-IPL-treated patients compared with 51% in IPL monotherapy group.[44] On the other hand, Yeung et al. did not find significant improvement in moderate inflammatory acne in his study that involved the use of methylaminolevulinic (MAL) PDT with IPL.[45] Hong et al. found that MAL combined with red light or IPL produced similar improvement in both inflammatory and noninflammatory acne, although MAL-red light combination produced faster response.[46]
In general, adverse effects were more severe and longer lasting when IPL is used in combination with a photosensitizing agent. Reported adverse effects include edematous erythema, crusting with exfoliation, post-treatment hyperpigmentation, and monomorphic acneiform eruptions that resolved spontaneously within 1–10 days.
Relatively few studies have examined IPL combined with conventional acne treatments. Faghihi et al.[47] found that IPL combined with topical erythromycin 2% solution was more effective than topical erythromycin 2% solution in reducing macular and erythematous inflammatory acne lesion remnants.
Overall, most clinical trials employing IPL in acne treatment have shown efficacious results, with more promising results for IPL used in combination with ALA than IPL monotherapy.
Laser sources including the KTP laser, PDL, and IR lasers
Potassium titanyl phosphate laser
In contrast to nonlaser light sources, lasers can selectively target endogenous or exogenous tissue chromophores by delivering coherent light of high radiance. KTP green light laser (532 nm) has traditionally been used to treat vascular lesions such as rosacea and telangiectasia.[48] More recently, KTP has been employed for acne therapy with minimal side effects.[49] Selective photothermolysis of blood vessels supplying sebaceous glands and/or a photodynamic reduction of P. acnes may underlie the therapeutic efficacy of KPT laser. Baugh et al. conducted a split-face study to determine the effectiveness of weekly treatment with KTP laser in 26 patients and reported a 35% and 21% reduction in acne severity at 1 and 4 weeks postfinal treatments, respectively.[50] No adverse effects were experienced, demonstrating that KTP laser was both safe and effective. Another study by Yilmaz et al. examined safety and efficacy of once a week versus twice weekly application of KTP laser in treating mild-to-moderate acne in 38 patients and found no significant difference.[51] A small open-label split-face study comparing safety and efficacy of ALA plus KTP laser to KTP laser alone found that combined use of ALA and KTP laser was associated with greater acne improvement (52%) compared with KTP laser alone (32%).[52]
Pulsed dye laser
The 585 nm PDL, similar to KTP laser, has been primarily used for the selective photothermolysis of vascular lesions but more recently has been used for inflammatory cutaneous disorders. A systematic review of PDL treatment for inflammatory conditions revealed nine studies on PDL treatment for acne with evidence that PDL may be an effective treatment for acne.[53] PDL has also been used for the treatment of hypertrophic facial acne scars.[54] PDL was thought to act by reducing P. acnes or sebaceous gland activity. However, Seaton et al. demonstrated that the PDL did not have any effect on the degree of P. acnes colonization or sebum production and found that the efficacy of this laser is likely through its local anti-inflammatory effects via upregulation of TGF-β.[55] In another study, Seaton et al. examined the utility of PDL for inflammatory acne in a randomized controlled trial involving 41 adults.[56] At week 12, the average total lesion count fell by 53% in patients treated with the PDL compared with 9% in the sham control group. Similarly, the inflammatory lesion counts fell by 49% in PDL-treated patients compared with 10% in control group. In a smaller split-face study comparing PDL with untreated control in 10 patients, single treatment of PDL resulted in visible therapeutic improvement in 50% of patients at six weeks post-treatment, although two patients had worsening of acne.[57] However, a randomized single-blind, controlled, split-face study by Orringer et al. involving 40 patients did not show significant improvement in facial acne with the nonpurpuric PDL therapy at the end of 12 weeks.[58]
A limited number of studies examined PDL compared with or in combination with conventional acne therapy. Shariff et al. reported safety and efficacy of PDL combined with multiple medical therapies in a female patient with severe acne vulgaris and a history of medical comorbidities, which contraindicated the use of most conventional first line therapies.[59] In another study, a group of 15 patients were treated with PDL and compared with 15 patients who received topical treatments (topical vitamin A acid, benzoyl peroxide) and another 15 patients who received chemical peels (trichloroacetic acid 25%).[60] Improvement of acne lesions was noted in all three groups with no significant difference in improvement between the three treatment protocols. However, PDL was associated with higher remission in the follow-up period. In a randomized controlled single-blinded trial, efficacy of adjuvant PDL treatment when combined with proven topical treatment (fixed-combination clindamycin 1% and benzoyl peroxide 5% hydrating gel) was examined in 80 patients.[61] Although topical treatment alone and topical treatment combined with PDL both produced acne improvement, there was no significant difference in the extent of improvement. Taken together, there is limited evidence of increased benefit of PDL either used alone or in combination with conventional therapies for acne treatment when compared with conventional therapies alone.
Two studies have examined efficacy of PDL in combination with photodynamic therapy. In a randomized controlled trial involving 15 patients, Haedersdal et al. compared long-PDL (LPDL) alone versus LPDL with MAL.[62] Inflammatory acne lesion counts were reduced more significantly on the MAL-LPDL site than LPDL site alone at 4 weeks (70% vs 50%) and 12 weeks (80% vs 67%). Orringer et al. conducted a randomized, controlled, split-face, single-blind clinical trial of 44 patients comparing ALA with PDL with an untreated control side.[63] Global acne severity improved bilaterally, although improvement was statistically significantly greater in ALA-PDL-treated skin than in untreated skin. Erythematous macules from previous active inflammatory lesions also decreased in treated skin. Notably, however, no statistically significant difference in any other acne subtype counts was noted between treated and untreated sides. More patients experienced improvement in inflammatory lesion counts than in noninflammatory lesion counts (30% vs 7% of patients.)
Infrared laser
IR laser (1320, 1450, and 1540 nm) is commonly used for nonablative facial skin rejuvenation but several studies have examined its utility in treating acne.[64]
1320 nm laser
In a randomized, controlled, single-blind, split-face clinical trial of 46 patients with facial acne, a series of three nonablative laser treatments with 1320 nm neodymium: yttrium–aluminum–garnet (Nd: YAG) laser resulted in transient but significant improvement in open comedones counts (27% decrease) compared with untreated control (12% decrease), but no difference in papule, pustule, and closed comedone counts or sebum production.[65] A later pilot study of 35 patients with moderate-to-severe acne treated with fractional 1320 nm Nd: YAG laser therapy reported 57% reduction in inflammatory lesions and 35% reduction of noninflammatory lesions as well as significant reduction of sebum level by 30%.[66]
1450 nm diode laser
In an early pilot study without a control group, 19 patients with inflammatory facial acne were treated with 1450 nm diode laser at 4- and 6-week intervals.[67] All patients had a reduction in acne lesions with 37%, 58%, and 83% decrease in lesion counts after one, two, and three treatments, respectively. The treatment was well tolerated. In a follow-up study, Jih et al. evaluated dose response of a 1450 nm diode laser for treatment of facial acne, sebum production, and acne scarring using two laser fluences, and examined long-term remission after completion of laser treatment.[68] Both fluences (14 or 16 J/cm2) resulted in reductions in the mean acne lesion counts after 1 and 3 treatments, with persistent reduction of 70.5%–76.1% reduction at 12-month follow-up indicating significant long-term remission. In addition, there was improvement in acne scarring and sebum production, supporting the hypothesis that therapeutic mechanism of this laser involves reduced sebaceous gland activity. However, in a randomized split-face, investigator-blinded study, treatment with 1450 nm laser did not reduce inflammatory lesion count or acne grade compared with untreated control side.[69]
Three studies examined the efficacy of 1450 nm laser combined with another modality for treatment of acne. One study reported a reduction of acne lesional counts on the upper back at six months after four treatments with 1450 nm laser and cryogen (mean reduction 98%) compared with cryogen alone (mean reduction 6%).[70] In contrast, the combination of microdermabrasion plus 1450 nm laser (55.6% reduction in acne lesions) was not significantly different from 1450 nm laser alone (53.5% reduction in acne lesion) in inflammatory facial acne clearance.[71] Glaich et al. studied the combined use of 595 nm PDL and the 1450 nm diode IR laser in 15 patients with inflammatory facial acne and found a significant mean decrease in lesional count by 52%, 63%, and 84% after one, two, and three treatments.[72] This demonstrated the use of combination lasers as a safe and effective modality for the treatment of inflammatory facial acne, acne scarring, and post-inflammatory erythema. However, the effects of the PDL or the 1450 nm diode laser used alone are undetermined.
1540 nm erbium laser
Several studies have examined the effect of a 1540 nm erbium glass laser treatment on acne. Bogel et al. reported 78% improvement in acne at 6-month post-treatment in 15 patients with moderate to severe inflammatory facial acne receiving laser therapy four times at 2-week intervals.[73] There was no change in sebum production. Angle et al. found evidence of long-term acne remission after four laser treatments performed at 4-week intervals.[74] The mean percent reduction of acne was 71%, 79%, and 73% at 6-month, 1-year, and 2-year follow-ups.
Taken together, studies of IR lasers on acne treatment have produced mixed results with unclear benefits. In addition, several studies are limited by small sample size or lack of controls. No studies have compared IR lasers to conventional therapy. More studies with increased sample size, randomization, and controls will be needed to clearly delineate benefits of IR lasers as an acne therapy.
Photodynamic therapy
PDT works via application of a photosensitizing agent immediately prior to light exposure. Commonly used photosensitizers include ALA or MAL. New photosensitizers include indocyanine green (ICG) and indole-3-acetic acid. A photosensitizer is absorbed by pilosebaceous units and upon activation by light of an appropriate wavelength, is converted via the heme biosynthetic pathway to protoporphyrin IX and subsequently produces reactive oxygen species that exert bactericidal effects on P. acnes and damage the pilosebaceous units. Light sources include lasers, LED, fluorescent lamps, and filtered incandescent or arc lamps.[3,64,75]
A 2009 systematic review of laser and light therapies for treatment of acne analyzed data from two trials comparing PDT to placebo, which showed a significant reduction in inflammatory lesion counts in the PDT group compared with placebo.[9] The two studies showed a reduction in inflammatory lesions of 27.6%, 37.9%, and 41.9% at 1, 3, and 6 months using ALA with 630 nm light for mild-to-moderate acne, and 68% at 12 weeks for MAL with 630 nm light for moderate-to-severe acne.[76,77] More recently, in a large self-controlled multicenter trial with 397 patients in China, low-dose ALA (5% gel) with one hour incubation and 633 nm LED light resulted in overall clearance rates of 82.1% after three or four treatment sessions.[78] The efficacy of ALA-PDT was noted to increase with corresponding baseline acne severity.
Several studies comparing the effectiveness of PDT versus light therapy alone have found increased benefit of PDT over light therapy alone. Hongcharu et al. compared four treatment protocols: ALA plus red light (550–700 nm), ALA alone, red light alone, and untreated control for back acne.[79] ALA plus red light showed clinically and statistically significant clearance of inflammatory acne for up to 20 weeks after multiple treatments and for up to 10 weeks after a single treatment. No improvement was noted for ALA alone, red light alone, or untreated sites. Similar results showing a significant reduction in inflammatory acne lesions for ALA-PDT (69% at three weeks follow up) but none for ALA alone, 635 nm light alone, or untreated sites were obtained in a smaller study by Pollock et al.[80] In contrast, in a split-face trial comparing 500–700 nm light plus ALA versus light alone, Rojanamatin et al. found improvement of inflammatory facial acne in both ALA-PDT and light alone treated.[81] However, lesions decreased significantly after one treatment on the ALA-PDT site compared with after two treatments on the light monotherapy site and ALA-PDT was associated with greater mean acne reduction (87.7%) compared with light monotherapy (66.8%) at 12 weeks. Other studies have found increased benefit of MAL-PDT compared with light alone, and ICG-PDT compared with light or ICG alone.[82,83,84] In addition, MAL-PDT-treated skin had decreased amounts of sebocytes and lipids along with atrophic sebaceous glands.
According to the authors’ experience and pilot study (n = 5, unpublished data), ALA-PDT for moderate inflammatory acne demonstrated global clearance of 70%–80% with single treatment and up to 95% for two or three sessions that were performed sequentially every 4–6 weeks. In these protocols, ALA (Levulan, Kerastick) was applied per standard protocols with incubation time 120–180 min, and PDT was activated through a split-face approach with long PDL (595 nm, Candela) versus blue light at 417 + 5 nm (BLU U, DUSA). Both methods induced typical postoperative photobiological responses with redness followed by skin peeling and complete healing within 7–10 day follow-up. PDT mediated with PDL provides the possibility for application of pulse stalking during treatment, in order to address more difficult-to-treat areas. In these series, the patients held topical therapies 48 h prior to therapy (including, and not limited to, topical retinoids) and resumed their topical regimens once peeling and redness was resolved. According to authors’ observations, PDT facilitated better acne control under regular topical regimen with significant delay of inflammatory acne flare-ups in a time period of 12–18 months.
In general, evidence supports that PDT therapy can improve acne lesions, has increased benefit when compared with light therapy alone, and that inflammatory lesions have a more robust response.
Photopneumatic technology
Photopneumatic technology for acne treatment is relatively a new therapy that has not been extensively studied. Photopneumatic devices combine gentle negative pressure with broad band pulsed light (400–1200 nm).[85,86] The negative pressure creates suction, which raises target structures in the dermis closer to the surface of skin prior to light exposure thus allowing more efficient energy transmission. Moreover, this suction pressure also helps to open the sebaceous gland allowing it to evacuate sebum, bacteria, and dead skin cells. Photopneumatic technology may also act by decreasing sebaceous gland activity. Omi et al. reported ultrastructural evidence of thermal injury to bacteria and pilosebaceous units in eight patients treated with photopneumatic therapy.[77]
There have been a small number of studies evaluating photopneumatic technology for acne treatment. A small study with 11 patients by Gold et al. evaluated the use of photopneumatic technology for the treatment of mild-to-moderate acne.[87] Patients received four treatments at 3-week intervals. They reported a reduction in both inflammatory (78.8%) and noninflammatory lesion counts (57.8%) at three months post-treatment. A larger study with 20 patients with mild to severe facial acne reported modest reduction in acne lesion counts and global clinical improvement after four treatments 2-week intervals.[88] In a split-face study, efficacy of photopneumatic therapy compared with untreated control was evaluated in 20 patients mild to moderate facial acne after receiving four treatments at 2-week intervals. There was a significant decrease in both inflammatory and noninflammatory acne lesion counts at three months postfinal treatment (37.5% and 41.38%, respectively).[89] Treatment was well tolerated with a few patients experience transient erythema, purpura, and/or exacerbation of pre-existing acne. Finally, in a retrospective multicenter study, clinical data was collected from 56 patients with mild-to-severe acne who had been treated 2–4 times with a portable photopneumatic device. Results of this study demonstrated that the median physician-rated clearance increased from 50% after a single treatment to 90% after the fourth treatment, whereas the median patient-rated clearance improved from 50% after a single treatment to 78% after the fourth treatment.[90]
Based on the limited number of studies, photopneumatic technology is safe and does demonstrate some efficacy in treatment of acne both in terms of short-term benefits as well as sustained remission. However, more studies involving larger numbers of subjects with longer follow-up periods, as well comparing photopneumatic technology to other therapy modalities, are required to validate the currently available evidence.
Self-use devices
Several US Food and Drug Administration (FDA)-approved optical devices for the treatment of acne exist. However, the approval process for devices may not follow the same stringent process as for pharmaceutical agents.[3] Therefore, clinicians should not assume the same level of safety or efficacy for approved optical devices as for approved pharmaceutical agents.
One study investigated safety and efficacy of at-home treatment of mild to moderate inflammatory acne with a FDA-approved blue light device (412 nm) at 2 J/cm2/day (equivalent to typical full-face treatment) or 29 J/cm2/day (equivalent to typical dose after localized spot treatment).[20] Results showed that blue light at both doses were effective in reducing the number of inflammatory lesions and acne flares and associated with improved cosmesis. In addition, 53% of subjects found blue light treatment to be much gentler than conventional acne treatment and 61% reported satisfaction with the treatment. Gold et al. reported a significant decrease in mild to moderate inflammatory acne at 1 and 3 months with home use of Silk’n Blue LED device (405–460 nm) in 17 patients.[21] Patients demonstrated a good understanding of device labeling and experienced no adverse events. Another study evaluated the efficacy of a combination of blue light (415 nm) with red light (633 nm) in reducing inflammatory acne lesions with mild-to-moderate acne after eight 20–30 minute self-administered treatments with a hand-held unit over four weeks.[24] Lesion counts were reduced 69% at eight weeks post-treatment course.
Complications of light and laser based therapies
In general, light- and laser-based treatments are safe in trained hands and are not associated with long-term complications. Many of the immediate post-treatment phenomena such as mild-to-moderate pain, erythema, or minimal edema are transient and resolve spontaneously requiring no treatment.[9,64] Blue and blue-red light therapy is well tolerated. Short-term adverse effects such as mild redness, dryness, itchiness, or stinging are self-resolving. No studies have studied long-term adverse effects.
Nonablative lasers achieve limited penetration depth in skin and therefore adverse reactions mostly involve operative discomfort and postoperative skin pigment changes. Discomfort during and shortly after treatment is described as burning, tingling, or itching. The most common adverse effects are mild discomfort, erythema, purpura, edema, blistering, and crusting, which usually spontaneously resolve within 48 h.[25] PDT has been found in some patients to be associated with considerable treatment-related pain and post-treatment erythema, pustular reactions, and epithelial exfoliation.[64] These reactions were found to be both short lasting and self-limited.
During procedures, the authors have found that implementation of different cooling methods, which may be incorporated into the light device or achieved by cool mist spray, ice, or cool air, to be helpful in alleviating discomfort. Topical anesthetic creams can be applied. As the majority of light devices target hemoglobin, and in the case of PDT oxygen supply plays a key role, topical anesthetics that may cause vasoconstriction are applied in moderation because they can decrease efficiency. Nerve blocks have also been used when extensive areas are treated. Patient feedback during procedures can be a good indication for navigating the settings of our devices. Application of topical steroids is limited to only in cases where pronounced skin irritation and intense pruritus are present shortly after the procedure. Postoperative discomfort due to nonablative light devices, if any, can further be managed with low-to-moderate doses of acetaminophen.
Post-treatment hyper- and hypopigmentation are also possible. Strict avoidance of sunlight for at least 24 h is necessary after treatment with ALA-PDT as light can provoke further porphyrin activation and lead to a phototoxic reaction.[3] Although the use of nonablative lasers in darker skin types may involve higher risks for inducing postinflammatory pigment changes, optimal operative settings in experienced hands reduce significantly the risks for permanent adverse reactions. Moreover, right candidate selection and patient compliance are fundamental to achieve the optimal outcome. Pretreatment with topical application of hydroquinone as well as strict sun protection and sunscreen application daily play a significant role in preventing skin pigment changes. A detailed counseling on sun avoidance or sun protection with broad spectrum sunscreen along with postoperative skin care instructions can be provided in writing.
For light-based devices such as PDT that work via selective photothermolysis of sebaceous glands, some concerns have been raised over its long-term safety as the pilosebaceous units may serve an important role in the immune system of the skin.[9] However, more studies are needed to examine long-term safety of PDT and other light-based devices.
SUMMARY
Significant progress has been made so far in light-based treatment of acne. The strongest evidence for efficacy of light-based therapies for acne is for blue and blue-red light, with the greatest effect on mild to moderate inflammatory acne lesions. There is also evidence that PDT is effective in treating inflammatory acne lesions, although the adverse effects, mostly short term and self-resolving, tend to be more severe than blue light. However, many of the clinical studies have small numbers of enrolled patients, are short in duration, and lack sufficient controls. There is also insufficient data to determine the precise optimal device, dosing, and number of treatments required in using these procedures for acne treatment. In addition, conclusions on the efficacy of light-based therapies are limited by the few number of studies comparing light-based treatments with standard pharmaceutical treatments such as antibiotics and retinoids. Going forward, as the most effective devices such as blue or visible light primarily reduce inflammatory lesions, more effective treatment of acne may be achieved if light therapy is combined with agents with anticomedogenic and comedolytic properties such as topical retinoids.
No specific studies have conducted a cost-analysis of light-based versus conventional therapies for acne. Most patients in the studies received light therapy as part of a trial in a clinic-based setting; although reimbursement by medical insurance can be received sometimes, it remains unclear whether these patients in reported trials provided out-of-pocket payments or received insurance coverage. Acne is a chronic condition that can require multiple medical visits and a wide spectrum of therapeutic modalities in combination in order to achieve management and stable results. Pertinent data supports that light devices can achieve control of acne flares when used as monotherapies or in combination with other modalities. As the vast majority of the applied devices are cleared by FDA, it remains hopeful that light devices may be approved by medical insurance plans for acne therapies in the near future. Finally, the recent development of various home-use devices may be more cost effective as they involve a one-time payment with unlimited usage; however, their efficacy and cost effectiveness compared with conventional therapies has not been studied.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.James WD. Clinical practice. Acne. N Engl J Med. 2005;352:1463–72. doi: 10.1056/NEJMcp033487. [DOI] [PubMed] [Google Scholar]
- 2.Berg M. Epidemiological studies of the influence of sunlight on the skin. Photodermatol. 1989;6:80–4. [PubMed] [Google Scholar]
- 3.Thiboutot D, Gollnick H, Bettoli V, Dreno B, Kang S, Leyden JJ, et al. Global Alliance to Improve Outcomes in Acne. New insights into the management of acne: An update from the Global Alliance to Improve Outcomes in Acne Group. J Am Acad Dermatol. 2009;60(Suppl):S1–50. doi: 10.1016/j.jaad.2009.01.019. [DOI] [PubMed] [Google Scholar]
- 4.Ashkenazi H, Malik Z, Harth Y, Nitzan Y. Eradication of Propionibacterium acnes by its endogenic porphyrins after illumination with high intensity blue light. FEMS Immunol Med Microbiol. 2003;35:17–24. doi: 10.1111/j.1574-695X.2003.tb00644.x. [DOI] [PubMed] [Google Scholar]
- 5.Melø TB. Uptake of protoporphyrin and violet light photodestruction of Propionibacterium acnes. Z Naturforsch C. 1987;42:123–8. doi: 10.1515/znc-1987-1-220. [DOI] [PubMed] [Google Scholar]
- 6.Elman M, Lebzelter J. Light therapy in the treatment of acne vulgaris. Dermatol Surg. 2004;30:139–46. doi: 10.1111/j.1524-4725.2004.30053.x. [DOI] [PubMed] [Google Scholar]
- 7.Young S, Bolton P, Dyson M, Harvey W, Diamantopoulos C. Macrophage responsiveness to light therapy. Lasers Surg Med. 1989;9:497–505. doi: 10.1002/lsm.1900090513. [DOI] [PubMed] [Google Scholar]
- 8.Shnitkind E, Yaping E, Geen S, Shalita AR, Lee WL. Anti-inflammatory properties of narrow-band blue light. J Drugs Dermatol. 2006;5:605–10. [PubMed] [Google Scholar]
- 9.Hamilton FL, Car J, Lyons C, Car M, Layton A, Majeed A. Laser and other light therapies for the treatment of acne vulgaris: Systematic review. Br J Dermatol. 2009;160:1273–85. doi: 10.1111/j.1365-2133.2009.09047.x. [DOI] [PubMed] [Google Scholar]
- 10.Shalita AR, Harthy Y, Elman M. Acne phototherapy using UV free high intensity narrow band blue light-3 center clinical study. Proc SPIE. 2001;4244:61–73. [Google Scholar]
- 11.Kawada A, Aragane Y, Kameyama H, Sangen Y, Tezuka T. Acne phototherapy with a high-intensity, enhanced, narrow-band, blue light source: An open study and in vitro investigation. J Dermatol Sci. 2002;30:129–35. doi: 10.1016/s0923-1811(02)00068-3. [DOI] [PubMed] [Google Scholar]
- 12.Elman M, Slatkine M, Harth Y. The effective treatment of acne vulgaris by a high-intensity, narrow band 405-420 nm light source. J Cosmet Laser Ther. 2003;5:111–7. [PubMed] [Google Scholar]
- 13.Omi T, Bjerring P, Sato S, Kawana S, Hankins RW, Honda M. 420 nm intense continuous light therapy for acne. J Cosmet Laser Ther. 2004;6:156–62. doi: 10.1080/14764170410023785. [DOI] [PubMed] [Google Scholar]
- 14.Tzung TY, Wu KH, Huang ML. Blue light phototherapy in the treatment of acne. Photodermatol Photoimmunol Photomed. 2004;20:266–9. doi: 10.1111/j.1600-0781.2004.00109.x. [DOI] [PubMed] [Google Scholar]
- 15.Morton CA, Scholefield RD, Whitehurst C, Birch J. An open study to determine the efficacy of blue light in the treatment of mild to moderate acne. J Dermatolog Treat. 2005;16:219–23. doi: 10.1080/09546630500283664. [DOI] [PubMed] [Google Scholar]
- 16.Tremblay JF, Sire DJ, Lowe NJ, Moy RL. Light-emitting diode 415 nm in the treatment of inflammatory acne: An open-label, multicentric, pilot investigation. J Cosmet Laser Ther. 2006;8:31–3. doi: 10.1080/14764170600607624. [DOI] [PubMed] [Google Scholar]
- 17.Noborio R, Nishida E, Kurokawa M, Morita A. A new targeted blue light phototherapy for the treatment of acne. Photodermatol Photoimmunol Photomed. 2007;23:32–4. doi: 10.1111/j.1600-0781.2007.00268.x. [DOI] [PubMed] [Google Scholar]
- 18.Ammad S, Gonzales M, Edwards C, Finlay AY, Mills C. An assessment of the efficacy of blue light phototherapy in the treatment of acne vulgaris. J Cosmet Dermatol. 2008;7:180–8. doi: 10.1111/j.1473-2165.2008.00386.x. [DOI] [PubMed] [Google Scholar]
- 19.Wheeland RG, Dhawan S. Evaluation of self-treatment of mild-to-moderate facial acne with a blue light treatment system. J Drugs Dermatol. 2011;10:596–602. [PubMed] [Google Scholar]
- 20.Wheeland RG, Koreck A. Safety and effectiveness of a new blue light device for the self-treatment of mild-to-moderate acne. J Clin Aesthet Dermatol. 2012;5:25–31. [PMC free article] [PubMed] [Google Scholar]
- 21.Gold MH, Biron JA, Sensing W. Clinical and usability study to determine the safety and efficacy of the Silk’n Blue Device for the treatment of mild to moderate inflammatory acne vulgaris. J Cosmet Laser Ther. 2014;16:108–13. doi: 10.3109/14764172.2013.854638. [DOI] [PubMed] [Google Scholar]
- 22.Goldberg DJ, Russell BA. Combination blue (415 nm) and red (633 nm) LED phototherapy in the treatment of mild to severe acne vulgaris. J Cosmet Laser Ther. 2006;8:71–5. doi: 10.1080/14764170600735912. [DOI] [PubMed] [Google Scholar]
- 23.Lee SY, You CE, Park MY. Blue and red light combination LED phototherapy for acne vulgaris in patients with skin phototype IV. Lasers Surg Med. 2007;39:180–8. doi: 10.1002/lsm.20412. [DOI] [PubMed] [Google Scholar]
- 24.Sadick NS. Handheld LED array device in the treatment of acne vulgaris. J Drugs Dermatol. 2008;7:347–50. [PubMed] [Google Scholar]
- 25.Sadick N. A study to determine the effect of combination blue (415 nm) and near-infrared (830 nm) light-emitting dioded (LED) therapy for moderate acne vulgaris. J Cosmet Laser Ther. 2009;11:125–8. doi: 10.1080/14764170902777349. [DOI] [PubMed] [Google Scholar]
- 26.Kwon HH, Lee JB, Yoon JY, Park SY, Ryu HH, Park BM, et al. The clinical and histological effect of home-use, combination blue-red LED phototherapy for mild-to-moderate acne vulgaris in Korean patients: A double-blind, randomized controlled trial. Br J Dermatol. 2013;168:1088–94. doi: 10.1111/bjd.12186. [DOI] [PubMed] [Google Scholar]
- 27.Papageorgiou P, Katsambas A, Chu A. Phototherapy with blue (415 nm) and red (660 nm) light in the treatment of acne vulgaris. Br J Dermatol. 2000;142:973–8. doi: 10.1046/j.1365-2133.2000.03481.x. [DOI] [PubMed] [Google Scholar]
- 28.See comment in PubMed Commons below. Gold MH, Rao J, Goldman MP, Bridges TM, Bradshaw VL, Boring MM, et al. A multicenter clinical evaluation of the treatment of mild to moderate inflammatory acne vulgaris of the face with visible blue light in comparison to topical 1% clindamycin antibiotic solution. J Drugs Dermatol. 2005;4:64–70. [PubMed] [Google Scholar]
- 29.Akaraphanth R, Kanjanawanitchkul W, Gritiyarangsan P. Efficacy of ALA-PDT vs blue light in the treatment of acne. Photodermatol Photoimmunol Photomed. 2007;23:186–90. doi: 10.1111/j.1600-0781.2007.00303.x. [DOI] [PubMed] [Google Scholar]
- 30.Sami NA, Attia AT, Badawi AM. Phototherapy in the treatment of acne vulgaris. J Drugs Dermatol. 2008;7:627–32. [PubMed] [Google Scholar]
- 31.Liu LH, Fan X, An YX, Zhang J, Wang CM, Yang RY. Randomized trial of three phototherapy methods for the treatment of acne vulgaris in Chinese patients. Photodermatol Photoimmunol Photomed. 2014;30:246–53. doi: 10.1111/phpp.12098. [DOI] [PubMed] [Google Scholar]
- 32.Babilas P. Light-assisted therapy in dermatology: The use of intense pulsed light (IPL) Med Laser Appl. 2010;25:61–9. [Google Scholar]
- 33.Taylor M, Porter R, Gonzalez M. Intense pulsed light may improve inflammatory acne through TNF-α down-regulation. J Cosmet Laser Ther. 2014;16:96–103. doi: 10.3109/14764172.2013.864198. [DOI] [PubMed] [Google Scholar]
- 34.Ali MM, Porter RM, Gonzalez ML. Intense pulsed light enhances transforming growth factor beta1/Smad3 signaling in acne-prone skin. J Cosmet Dermatol. 2013;12:195–203. doi: 10.1111/jocd.12045. [DOI] [PubMed] [Google Scholar]
- 35.Wat H, Wu DC, Rao J, Goldman MP. Application of intense pulsed light in the treatment of dermatologic disease: A systematic review. Dermatol Surg. 2014;40:359–77. doi: 10.1111/dsu.12424. [DOI] [PubMed] [Google Scholar]
- 36.Kumaresan M, Srinivas CR. Efficacy of IPL in treatment of acne vulgaris: Comparison of single- and burst-pulse mode in IPL. Indian J Dermatol. 2010;55:370–2. doi: 10.4103/0019-5154.74550. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Kawana S, Tachihara R, Kato T, Omi T. Effect of smooth pulsed light at 400 to 700 and 870 to 1,200 nm for acne vulgaris in Asian skin. Dermatol Surg. 2010;36:52–7. doi: 10.1111/j.1524-4725.2009.01380.x. [DOI] [PubMed] [Google Scholar]
- 38.Chang SE, Ahn SJ, Rhee DY, Choi JH, Moon KC, Suh HS, et al. Treatment of facial acne papules and pustules in Korean patients using an intense pulsed light device equipped with a 530- to 750-nm filter. Dermatol Surg. 2007;33:676–9. doi: 10.1111/j.1524-4725.2007.33142.x. [DOI] [PubMed] [Google Scholar]
- 39.Choi YS, Suh HS, Yoon MY, Min SU, Lee DH, Suh DH. Intense pulsed light vs. pulsed-dye laser in the treatment of facial acne: A randomized split-face trial. J Eur Acad Dermatol Venereol. 2010;24:773–80. doi: 10.1111/j.1468-3083.2009.03525.x. [DOI] [PubMed] [Google Scholar]
- 40.El-Latif AA, Hassan FA, Elshahed AR, Mohamed AG, Elsaie ML. Intense pulsed light versus benzoyl peroxide 5% gel in treatment of acne vulgaris. Lasers Med Sci. 2014;29:1009–15. doi: 10.1007/s10103-013-1440-0. [DOI] [PubMed] [Google Scholar]
- 41.Taub AF. A comparison of intense pulsed light, combination radiofrequency and intense pulsed light, and blue light in photodynamic therapy for acne vulgaris. J Drugs Dermatol. 2007;6:1010–6. [PubMed] [Google Scholar]
- 42.Santos MA, Belo VG, Santos G. Effectiveness of photodynamic therapy with topical 5-aminolevulinic acid and intense pulsed light versus intense pulsed light alone in the treatment of acne vulgaris: Comparative study. Dermatol Surg. 2005;31:910–5. doi: 10.1097/00042728-200508000-00004. [DOI] [PubMed] [Google Scholar]
- 43.Shaaban D, Abdel-Samad Z, El-Khalawany M. Photodynamic therapy with intralesional 5-aminolevulinic acid and intense pulsed light versus intense pulsed light alone in the treatment of acne vulgaris: A comparative study. Dermatol Ther. 2012;25:86–91. doi: 10.1111/j.1529-8019.2012.01427.x. [DOI] [PubMed] [Google Scholar]
- 44.Mei X, Shi W, Piao Y. Effectiveness of photodynamic therapy with topical 5-aminolevulinic acid and intense pulsed light in Chinese acne vulgaris patients. Photodermatol Photoimmunol Photomed. 2013;29:90–6. doi: 10.1111/phpp.12031. [DOI] [PubMed] [Google Scholar]
- 45.Yeung CK, Shek SY, Bjerring P, Yu CS, Kono T, Chan HH. A comparative study of intense pulsed light alone and its combination with photodynamic therapy for the treatment of facial acne in Asian skin. Lasers Surg Med. 2007;39:1–6. doi: 10.1002/lsm.20469. [DOI] [PubMed] [Google Scholar]
- 46.Hong JS, Jung JY, Yoon JY, Suh DH. Acne treatment by methyl amniolevulinate photodynamic therapy with red light vs. intense pulsed light. Int J Dermatol. 2013;52:614–9. doi: 10.1111/j.1365-4632.2012.05673.x. [DOI] [PubMed] [Google Scholar]
- 47.Faghihi G, Isfahani AK, Hosseini SM, Radan MR. Efficacy of intense pulsed light combined with topical erythromycin solution 2% versus topical erythromycin solution 2% alone in the treatment of persistent facial erythematous acne macules. Adv Biomed Res. 2012;1:70. doi: 10.4103/2277-9175.102974. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Ting PT, Rao J. Vascular lesions. Curr Probl Dermatol. 2011;42:67–80. doi: 10.1159/000328264. [DOI] [PubMed] [Google Scholar]
- 49.Nouri K, Ballard CJ. Laser therapy for acne. Clin Dermatol. 2006;24:26–32. doi: 10.1016/j.clindermatol.2005.10.020. [DOI] [PubMed] [Google Scholar]
- 50.Baugh WP, Kucaba WD. Nonablative phototherapy for acne vulgaris using the KTP 532 nm laser. Dermatol Surg. 2005;31:1290–6. doi: 10.1111/j.1524-4725.2005.31205. [DOI] [PubMed] [Google Scholar]
- 51.Yilmaz O, Senturk N, Yuksel EP, Aydin F, Ozden MG, Canturk T, et al. Evaluation of 523-nm KTP laser treatment efficacy on acne vulgaris with once and twice weekly applications. J Cosmet Laser Ther. 2011;13:303–7. doi: 10.3109/14764172.2011.630087. [DOI] [PubMed] [Google Scholar]
- 52.Sadick N. An open-label, split-face study comparing the safety and efficacy of levulan kerastick (aminolevulonic acid) plus a 532 nm KTP laser to a 532 nm KTP laser alone for the treatment of moderate facial acne. J Drugs Dermatol. 2010;9:229–33. [PubMed] [Google Scholar]
- 53.Erceg A, de Jong EM, van de Kerkhof PC, Seyger MM. The efficacy of pulsed dye laser treatment for inflammatory skin diseases: A systematic review. J Am Acad Dermatol. 2013;69:609–15.e8. doi: 10.1016/j.jaad.2013.03.029. [DOI] [PubMed] [Google Scholar]
- 54.Alster TS, McMeekin TO. Improvement of facial acne scars by the 585 nm flashlamp-pumped pulsed dye laser. J Am Acad Dermatol. 1996;35:79–81. doi: 10.1016/S0190-9622(96)90501-0. [DOI] [PubMed] [Google Scholar]
- 55.Seaton ED, Mouser PE, Charakida A, Alam S, Seldon PM, Chu AC. Investigation of the mechanism of action of nonablative pulsed-dye laser therapy in photorejuvenation and inflammatory acne vulgaris. Br J Dermatol. 2006;155:748–55. doi: 10.1111/j.1365-2133.2006.07429.x. [DOI] [PubMed] [Google Scholar]
- 56.Seaton ED, Charakida A, Mouser PE, Grace I, Clement RM, Chu AC. Pulsed-dye laser treatment for inflammatory acne vulgaris: Randomised controlled trial. Lancet. 2003;362:1347–52. doi: 10.1016/s0140-6736(03)14629-6. [DOI] [PubMed] [Google Scholar]
- 57.Jasim ZF, Al-Qargaz F, Handley JM. To the editor: Effect of single pulsed dye laser treatment on acne vulgaris. Dermatol Surg. 2005;31:1483. doi: 10.1097/00042728-200511000-00025. [DOI] [PubMed] [Google Scholar]
- 58.Orringer JS, Kang S, Hamilton T, Schumacher W, Cho S, Hammerberg C, et al. Treatment of acne vulgaris with a pulsed dye laser: A randomized controlled trial. JAMA. 2004;291:2834–9. doi: 10.1001/jama.291.23.2834. [DOI] [PubMed] [Google Scholar]
- 59.Shariff A, Keck L, Zlotoff B. Acne vulgaris in the context of complex medical co-morbidities: The management of severe acne vulgaris in a female with retinitis pigmentosa-utilizing pulse dye laser in conjunction with medical therapy. Dermatol Online J. 2014;20 pii: doj_21763. [PubMed] [Google Scholar]
- 60.Leheta TM. Role of the 585-nm pulsed dye laser in the treatment of acne in comparison with other topical therapeutic modalities. J Cosmet Laser Ther. 2009;11:118–24. doi: 10.1080/14764170902741329. [DOI] [PubMed] [Google Scholar]
- 61.Karsai S, Schmitt L, Raulin C. The pulsed-dye laser as an adjuvant treatment modality in acne vulgaris: A randomized controlled single-blinded trial. Br J Dermatol. 2010;163:395–401. doi: 10.1111/j.1365-2133.2010.09806.x. [DOI] [PubMed] [Google Scholar]
- 62.Haedersdal M, Togsverd-Bo K, Wiegell SR, Wulf HC. Long-pulsed dye laser versus long-pulsed dye laser-assisted photodynamic therapy for acne vulgaris: A randomized controlled trial. J Am Acad Dermatol. 2008;58:387–94. doi: 10.1016/j.jaad.2007.11.027. [DOI] [PubMed] [Google Scholar]
- 63.Orringer JS, Sachs DL, Bailey E, Kang S, Hamilton T, Voorhees JJ. Photodynamic therapy for acne vulgaris: A randomized, controlled, split-face clinical trial of topical aminolevulinic acid and pulsed dye laser therapy. J Cosmet Dermatol. 2010;9:28–34. doi: 10.1111/j.1473-2165.2010.00483.x. [DOI] [PubMed] [Google Scholar]
- 64.Rai R, Natarajan K. Laser and light based treatments of acne. Indian J Dermatol Venereol Leprol. 2013;79:300–9. doi: 10.4103/0378-6323.110755. [DOI] [PubMed] [Google Scholar]
- 65.Orringer JS, Kang S, Maier L, Johnson TM, Sachs DL, Karimipour DJ, et al. A randomized, controlled, split-face clinical trial of 1320-nm Nd: YAG laser therapy in the treatment of acne vulgaris. J Am Acad Dermatol. 2007;56:432–8. doi: 10.1016/j.jaad.2006.10.978. [DOI] [PubMed] [Google Scholar]
- 66.Deng H, Yuan DF, Yan CL, Ding XA. Fractional 1320 nm Nd: YAG laser in the treatment of acne vulgaris: A pilot study. Photodermatol Photoimmunol Photomed. 2009;25:278–9. doi: 10.1111/j.1600-0781.2009.00451.x. [DOI] [PubMed] [Google Scholar]
- 67.Friedman PM, Jih MH, Kimyai-Asadi A, Goldberg LH. Treatment of inflammatory facial acne vulgaris with the 1450-nm diode laser: A pilot study. Dermatol Surg. 2004;30:147–51. doi: 10.1111/j.1524-4725.2004.30062.x. [DOI] [PubMed] [Google Scholar]
- 68.Jih MH, Friedman PM, Goldberg LH, Robles M, Glaich AS, Kimyai-Asadi A. The 1450-nm diode laser for facial inflammatory acne vulgaris: Dose-response and 12-month follow-up study. J Am Acad Dermatol. 2006;55:80–7. doi: 10.1016/j.jaad.2006.02.018. [DOI] [PubMed] [Google Scholar]
- 69.Darne S, Hiscutt EL, Seukeran DC. Evaluation of the clinical efficacy of the 1,450 nm laser in acne vulgaris: A randomized split-face, investigator-blinded clinical trial. Br J Dermatol. 2011;165:1256–62. doi: 10.1111/j.1365-2133.2011.10614.x. [DOI] [PubMed] [Google Scholar]
- 70.Paithankar DY, Ross EV, Saleh BA, Blair MA, Graham BS. Acne treatment with a 1,450 nm wavelength laser and cryogen spray cooling. Lasers Surg Med. 2002;31:106–14. doi: 10.1002/lsm.10086. [DOI] [PubMed] [Google Scholar]
- 71.Wang SQ, Counters JT, Flor ME, Zelickson BD. Treatment of inflammatory facial acne with the 1,450 nm diode laser alone versus microdermabrasion plus the 1,450 nm laser: A randomized, split-face trial. Dermatol Surg. 2006;32:249–55. [PubMed] [Google Scholar]
- 72.Glaich AS, Friedman PM, Jih MH, Goldberg LH. Treatment of inflammatory facial acne vulgaris with combination 595-nm pulsed-dye laser with dynamic-cooling-device and 1,450-nm diode laser. Lasers Surg Med. 2006;38:177–80. doi: 10.1002/lsm.20209. [DOI] [PubMed] [Google Scholar]
- 73.Bogle MA, Dover JS, Arndt KA, Mordon S. Evaluation of the 1,540-nm erbium: Glass laser in the treatment of inflammatory facial acne. Dermatol Surg. 2007;33:810–7. doi: 10.1111/j.1524-4725.2007.33174.x. [DOI] [PubMed] [Google Scholar]
- 74.Angel S, Boineau D, Dahan S, Mordon S. Treatment of active acne with an Er: Glass (1.54 microm) laser: A 2-year follow-up study. J Cosmet Laser Ther. 2006;8:171–6. doi: 10.1080/14764170600915985. [DOI] [PubMed] [Google Scholar]
- 75.Morton CA, Szeimies RM, Sidoroff A, Braathen LR. European guidelines for topical photodynamic therapy part 1: Treatment delivery and current indications-actinic keratoses, Bowen's disease, basal cell carcinoma. J Eur Acad Dermatol Venereol. 2013;27:536–44. doi: 10.1111/jdv.12031. [DOI] [PubMed] [Google Scholar]
- 76.Hong SB, Lee MH. Topical aminolevulinic acid-photodynamic therapy for the treatment of acne vulgaris. Photodermatol Photoimmunol Photomed. 2005;21:322–5. doi: 10.1111/j.1600-0781.2005.00181.x. [DOI] [PubMed] [Google Scholar]
- 77.Wiegell SR, Wulf HC. Photodynamic therapy of acne vulgaris using methyl aminolaevulinate: A blinded, randomized, controlled trial. Br J Dermatol. 2006;154:969–76. doi: 10.1111/j.1365-2133.2005.07107.x. [DOI] [PubMed] [Google Scholar]
- 78.Ma L, Xiang LH, Yu B, Yin R, Chen L, Wu Y, et al. Lose-dose topical 5-aminolevulinic acid photodynamic therapy in the treatment of different severity of acne vulgaris. Photodiagnosis Photodyn Ther. 2013;10:583–90. doi: 10.1016/j.pdpdt.2013.06.007. [DOI] [PubMed] [Google Scholar]
- 79.Hongcharu W, Taylor CR, Chang Y, Aghassi D, Suthamjariya K, Anderson RR. Topical ALA-photodynamic therapy for the treatment of acne vulgaris. J Invest Dermatol. 2000;115:183–92. doi: 10.1046/j.1523-1747.2000.00046.x. [DOI] [PubMed] [Google Scholar]
- 80.Pollock B, Turner D, Stringer MR, Bojar RA, Goulden V, Stables GI, et al. Topical aminolaevulinic acid-photodynamic therapy for the treatment of acne vulgaris: A study of clinical efficacy and mechanism of action. Br J Dermatol. 2004;151:616–22. doi: 10.1111/j.1365-2133.2004.06110.x. [DOI] [PubMed] [Google Scholar]
- 81.Rojanamatin J, Choawawanich P. Treatment of inflammatory facial acne vulgaris with intense pulsed light and short contact of topical 5-aminolevulinic acid: A pilot study. Dermatol Surg. 2006;32:991–7. doi: 10.1111/j.1524-4725.2006.32221.x. [DOI] [PubMed] [Google Scholar]
- 82.Hörfelt C, Funk J, Frohm-Nilsson M, Wiegleb Edström D, Wennberg AM. Topical methyl aminolaevulinate photodynamic therapy for treatment of facial acne vulgaris: Results of a randomized, controlled study. Br J Dermatol. 2006;155:608–13. doi: 10.1111/j.1365-2133.2006.07340.x. [DOI] [PubMed] [Google Scholar]
- 83.Pinto C, Schafer F, Orellana JJ, Gonzalez S, Hasson A. Efficacy of red light alone and methyl-aminolaevulinate-photodynamic therapy for the treatment of mild and moderate facial acne. Indian J Dermatol Venereol Leprol. 2013;79:77–82. doi: 10.4103/0378-6323.104673. [DOI] [PubMed] [Google Scholar]
- 84.Tuchin VV, Genina EA, Bashkatov AN, Simonenko GV, Odoevskaya OD, Altshuler GB. A pilot study of ICG laser therapy of acne vulgaris: Photodynamic and photothermolysis treatment. Lasers Surg Med. 2003;33:296–310. doi: 10.1002/lsm.10211. [DOI] [PubMed] [Google Scholar]
- 85.Omi T. Photopneumatic technology in acne treatment and skin rejuvenation: Histological assessment. Laser Ther. 2012;21:113–23. doi: 10.5978/islsm.12-OR-07. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Omi T, Munavalli GS, Kawana S, Sato S. Ultrastructural evidence for thermal injury to pilosebaceous units during the treatment of acne using photopneumatic (PPX) therapy. J Cosmet Laser Ther. 2008;10:7–11. doi: 10.1080/14764170701762427. [DOI] [PubMed] [Google Scholar]
- 87.Gold MH, Biron J. Efficacy of a novel combination of pneumatic energy and broadband light for the treatment of acne. J Drugs Dermatol. 2008;7:639–42. [PubMed] [Google Scholar]
- 88.Wanitphakdeedecha R, Tanzi EL, Alster TS. Photopneumatic therapy for the treatment of acne. J Drugs Dermatol. 2009;8:239–41. [PubMed] [Google Scholar]
- 89.Lee EJ, Lim HK, Shin MK, Suh DH, Lee SJ, Kim NI. An open-label, split-face trial evaluation efficacy and safety of photopneumatic therapy for the treatment of acne. Ann Dermatol. 2012;24:280–6. doi: 10.5021/ad.2012.24.3.280. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Shamban AT, Enokibori M, Narurkar V, Wilson D. Photopneumatic technology for the treatment of acne vulgaris. J Drugs Dermatol. 2008;7:139–45. [PubMed] [Google Scholar]