

Abstract
Background:
Depigmented skin lesions are of great concern in the society, especially in the Indian subcontinent. These comprise many infective and inflammatory conditions that cause apprehension and anxiety among patients due to the social stigma attached to these conditions. Idiopathic guttate hypomelanosis (IGH) appears similar to many depigmented lesions and differentiation of IGH from these conditions is difficult clinically as well as histopathologically.
Methods:
Clinically suspected IGH were included in the study. All IGH lesions were confirmed by histopathology. Clinical data and dermoscopic patterns were analyzed and presented in proportions and percentages.
Results:
Thirty patients were included in the study with 16 females and 14 males. Dermoscopy showed amoeboid, feathery, petaloid and nebuloid patterns in 12, 7, 6 and 1 patients respectively. Four patients had combination of these patterns.
Conclusion:
Dermoscopy of IGH revealed consistent patterns. Hence, we propose these patterns were specific to IGH and help clinician to differentiate many depigmented skin lesions from IGH in clinical practice. However, histopathology must be done for confirmation of diagnosis. Further studies on dermoscopy of IGH with histopathology correlation are proposed.
Keywords: Dermoscopy, idiopathic guttate hypomelanosis, pattern
INTRODUCTION
Depigmented skin lesions are commonly encountered in day-to-day practice, and they pose a diagnostic challenge for the clinician. Many of them appear similar clinically. One has to differentiate depigmented lesions from vitiligo as it carries tremendous social implications as social stigma, especially in India.[1] Idiopathic guttate hypomelanosis (IGH) is one such depigmented skin condition whos incidence in India is about 20% in patients below the age of 30 years, and it shoots up to 80% of patients over the age of 70 years.[2] Morphologically, IGH looks similar to other depigmented skin lesions including vitiligo making it difficult to diagnose and differentiate IGH from other conditions on clinical grounds [Figure 1]. Therefore, there is a need for standardized criteria or patterns to differentiate these conditions. IGH is commonly seen in elderly patients with obscure etiopathogenesis and characterized by hypopigmented or depigmented macules and patches clinically.[3] Authors thought dermoscopy may fill this gap making the possibility of clinical diagnosis of IGH. Dermoscopy, a noninvasive, in vivo technique for the microscopic examination of pigmented skin lesions, has the potential to improve the diagnostic accuracy.[4]
Figure 1.
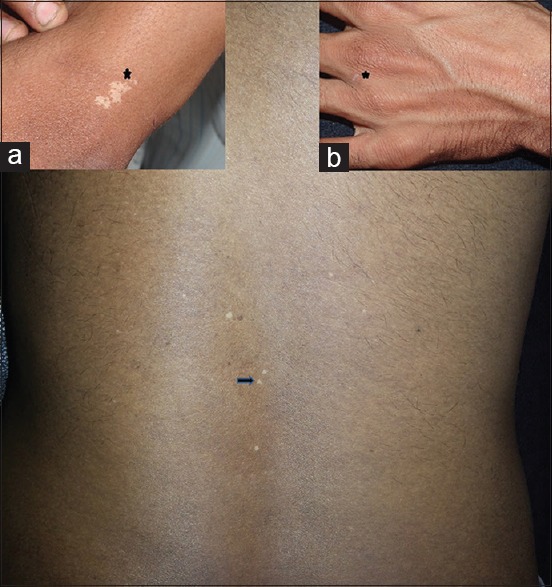
Well demarcated macules and patches of idiopathic guttate hypomelanosis (IGH) on the back. Panels show IGH on wrist (a) and on hand (b)
Although dermoscopy is widely used in the differential diagnosis of pigmented lesions, it has expanded its applications in dermatology. Alternative applications of dermoscopy include inflammatory diseases, parasitoses, hair and nail abnormalities.[5] Studies on dermoscopy of IGH a lesions are not reported in the literature. Hence, a study on dermoscopic observation of IGH lesions was carried out wherein authors could find particular dermoscopic patterns that were consistently seen in IGH.
MATERIALS AND METHODS
Ethics
Written informed consent was taken from patients. The ethical clearance for the study was obtained by the Institutional Ethical Committee.
Patients
This study was carried out among 30 patients attending Department of Dermatology in a tertiary care hospital attached to S. Nijalingappa Medical College at Bagalkot, South India between January and July 2013. Thirty patients with IGH lesions were subjected for a complete history and dermatological examination. Demographic and clinical data was documented.
Dermoscopic examination
Dermlite 3 dermoscope (3Gen, LLC, 31521 Rancho Veijo Road Suite104, San Jaun Capistran,CA 92675, USA) with polarized light (×10 magnification) was employed in the study. Sony Cybershot camera DSC-W800 (Sony Electronics Inc., San Diego, California, USA) was attached to save the images. Initially, ultrasound gel was applied either on the faceplate of the dermoscope or on the skin lesions and then lesions were observed through the eyepiece of dermoscopy. Although polarized dermoscopy was employed, ultrasound gel was applied for clarity of images and to lessen distortions associated with light.
Skin biopsy
All IGH lesions were subjected to skin biopsy, and histopathological examination was done to confirm the diagnosis.
Statistical analysis
Data were collected, analyzed and tabulated. The results were statistically described in terms of distribution and duration of lesions, mean ± standard deviation (±SD) and frequency of dermoscopic patterns when appropriate.
RESULTS
There were 16 females and 14 males in the study. Average age of the patients was 54.5 years with a range of 24 years to 85 years. The distribution of IGH lesions according to age groups and sex is shown in Figure 2. Dermoscopy demonstrated amoeboid, feathery, petaloid and nebuloid patterns in 14 (46.66%), 12 (40%), 7 (23.33%) and one patient (03.33%) respectively [Figure 3]. The amoeboid pattern [Figure 4] with amoeba-like pseudopods extending at periphery was commonly observed. Feathery pattern [Figure 5] having feather-like striations extending into surrounding skin, petaloid pattern [Figure 6] with well-defined borders and nebuloid pattern [Figure 7] with indistinct margins, merging into surrounding skin were demonstrated in the decreasing order. Age of the patients and mean duration of IGH lesions is presented in Table 1. Distribution of dermoscopic patterns among different age groups is depicted in Figure 8. Feathery pattern (50.4 ± 10.9) was observed in smaller age groups and amoeboid (50.86 ± 17.6), petaloid (52.6 ± 15.3) and nebuloid (55) were seen in older age groups. The distribution of dermoscopic patterns according to duration of IGH lesions is given in Figure 9. The feathery pattern (8.93 ± 6.97) was seen in patients with longer duration of skin lesions, and nebuloid pattern (6.00) was observed in patients with lesser duration of skin lesions. The basket-weave hyperkeratosis was observed in 40% corresponding to whitish areas in feathery pattern and loss of melanin globules was seen in 100% corresponding to depigmentation in all patterns in histopathology [Figure 10].
Figure 2.

Distribution of idiopathic guttate hypomelanosis lesions according to age and sex
Figure 3.

Dermoscopic patterns among idiopathic guttate hypomelanosis lesions
Figure 4.

Dermoscopy showing amoeboid pattern with peripheries resembling pseudopods (yellow arrow) of amoeba
Figure 5.

Dermoscopy showing feathery pattern with feather-like (yellow arrow) margins and white areas (yellow diamond)
Figure 6.

Dermoscopy showing the petaloid pattern with well-defined petal-like (yellow arrow) borders
Figure 7.

Dermoscopy showing nebuloid pattern with indistinct borders
Table 1.
Describing age of the patients and mean duration of IGH lesions

Figure 8.

Trend of occurrence of dermoscopic patterns among different age groups
Figure 9.

Trend of occurrence of dermoscopic patterns according to duration of idiopathic guttate hypomelanosis lesions
Figure 10.

Histopathology showing basket-weave hyperkeratosis, flattening of rete ridges and loss of melanin globules in epidermis (H and E, ×10)
DISCUSSION
Idiopathic guttate hypomelanosis is an acquired leukoderma of unknown cause found in all races.[6] Its pathogenesis may depend on various factors such as patient age and sun-exposure.[7] Clinically, the lesions are porcelain-white macules, usually 2–6 mm in size, but sometimes they are larger. The borders are sharply defined, often angular and irregular with normal skin markings.[8] It is also known as disseminate lenticular leukoderma and can be mistaken for vitiligo.[9] IGH has to be distinguished in clinical practice from other depigmented and hypopigmented conditions such as leprosy, vitiligo, pityriasis alba, and pityriasis versicolor. The histological findings associated with IGH are hyperkeratosis, an atrophic epidermis, and flattened rete ridges and decreased melanin content, and reduced numbers of melanocytes.[7] However, at times, it becomes difficult to differentiate IGH from guttate vitiligo due to similar histopathological changes. Dermoscopy visualizes the color patterns in the epidermis, dermo-epidermal junction and papillary dermis; when these patterns are observed consistently in a given disease, they could aid in its diagnosis.[10] Although clinicoepidemiological and histopathological studies of IGH abound in the literature, studies on dermoscopic evaluation are rare. Bambroo et al. appreciated four patterns dermoscopy of IGH namely nebuloid, petaloid, feathery and amoeboid.[1] Similar patterns were observed in our study. Nebuloid pattern of IGH was observed in lesions of recent onset and also among older patients. Feathery, amoeboid, and petaloid patterns were more commonly seen in older lesions of IGH. Histopathology confirmed the clinical diagnosis in our study. The authors believe that the whitish areas (yellow diamond) in the center of feathery patterned lesions correlate with hyperkeratosis on histopathology, and denote longstanding disease. Understanding this relationship may help in the diagnosis of IGH.[11] Angular, irregular and convex borders on clinical examination also appear as distinct patterns in dermoscopy. It may be stated that patterns documented here by authors are dermoscopic variants of IGH, not histopathological variants.
CONCLUSION
A study of dermoscopic patterns in IGH will aid the clinician in making a correct diagnosis thus ameliorating anxiety and apprehension associated with depigmented lesions in the society. Larger studies of IGH incorporating histopathological correlation, and comparison with the dermoscopic appearances in vitiligo are recommended.
ACKNOWLEDGMENTS
Authors acknowledge the help of Dr. Manjula Kashinakunti for her statistical assistance.
Footnotes
Source of Support: Nil
Conflict of Interest: Authors declare no conflict of interest.
REFERENCES
- 1.Bambroo M, Pande S, Khopkar U. Dermoscopy in the differentiation of idiopathic guttate hypomelanosis (IGH) and Guttate vitiligo. In: Khopkar S, editor. Dermoscopy and Trichoscopy in Diseases of the Brown Skin. Atlas and Short Text. 1st ed. New Delhi: Jaypee Brothers Ltd; 2012. pp. 97–103. [Google Scholar]
- 2.Patange VS, Fernandez RJ. A study of geriatric dermatoses. Indian J Dermatol Venereol Leprol. 1995;61:206–8. [PubMed] [Google Scholar]
- 3.Shin MK, Jeong KH, Oh IH, Choe BK, Lee MH. Clinical features of idiopathic guttate hypomelanosis in 646 subjects and association with other aspects of photoaging. Int J Dermatol. 2011;50:798–805. doi: 10.1111/j.1365-4632.2010.04743.x. [DOI] [PubMed] [Google Scholar]
- 4.Kittler H, Pehamberger H, Wolff K, Binder M. Diagnostic accuracy of dermoscopy. Lancet Oncol. 2002;3:159–65. doi: 10.1016/s1470-2045(02)00679-4. [DOI] [PubMed] [Google Scholar]
- 5.Micali G. Introduction. In: Micali G, Lacarrubba F, editors. Dermatoscopy in Clinical Practice-Beyond Pigmented Lesion. 1st ed. London: Informa Healthcare; 2010. pp. 1–2. [Google Scholar]
- 6.Goldust M, Mohebbipour A, Mirmohammadi R. Treatment of idiopathic guttate hypomelanosis with fractional carbon dioxide lasers. J Cosmet Laser Ther. 2013 doi: 10.3109/14764172.2013.803369. [DOI] [PubMed] [Google Scholar]
- 7.Kim SK, Kim EH, Kang HY, Lee ES, Sohn S, Kim YC. Comprehensive understanding of idiopathic guttate hypomelanosis: Clinical and histopathological correlation. Int J Dermatol. 2010;49:162–6. doi: 10.1111/j.1365-4632.2009.04209.x. [DOI] [PubMed] [Google Scholar]
- 8.Anstey AV. Rook's, Textbook of Dermatology. 8th ed. West Sussex: Wiley-Blackwell; 2010. Disorders of skin colour; pp. 58.1–59. [Google Scholar]
- 9.Argnelles-Casals D, Gonzalez D. La leucoderme lenticulaire disséminée. Ann Dermatol Syphiligr. 1969;96:283–6. [PubMed] [Google Scholar]
- 10.Nischal KC, Khopkar U. Dermoscope. Indian J Dermatol Venereol Leprol. 2005;71:300–3. doi: 10.4103/0378-6323.16633. [DOI] [PubMed] [Google Scholar]
- 11.Bowling J. In: Diagnostic Dermoscopy-The Illustrated Guide. 1st ed. Bowling S, editor. West Sussex: Wiley-Blackwell; 2012. pp. 2–14. [Google Scholar]