

Abstract
Objectives:
The aim of this study was to investigate the prevalence and distribution of hypodontia in the permanent teeth among a group of the Qatari sample and to compare the present results with findings from other populations.
Materials and Methods:
Records of 1269 Qatari patients (674 females; mean age 11.8 ± 2.3 and 595 males; mean age 11.4 ± 2.2) which included panoramic radiographs were examined to identify hypodontia. All permanent teeth were investigated except third molars.
Results:
The prevalence of hypodontia was 6.2% (females 8% and males 4.2%; P < 0.05). The majority of patients had one or two missing teeth. There were no significant differences between right and left sides for any particular tooth. The most frequently missing teeth were maxillary lateral incisors (36.2%), followed by mandibular second premolar (32.6%) and maxillary second premolar (20.2%). Hypodontia was more commonly found unilaterally than bilaterally (63.2% and 44.3%; respectively).
Conclusions:
The prevalence of hypodontia in a group of the Qatari population was within the average value of the majority of published studies in the literature. Hypodontia was significantly more prevalent in females. Although less prevalent, considerable cases of bilateral missing were found in the present study, which necessitates the urgent need for intervention and multi-disciplinary team approach for management.
Keywords: Hypodontia, patient, prevalence, Qatari
INTRODUCTION
Among the most important elements in assessing patient's oral health prior to any clinical intervention is to determine the number of teeth. By definition, congenitally missing teeth are those that fail to erupt in the oral cavity and remain invisible in a radiograph, which implies that this is caused by disturbances during the early stages of tooth development.[1] Hypodontia, a commonly used term to describe the absence of one to six teeth, is one of the most common dental developmental anomalies in human. The absence of more than six teeth is called oligodontia.[2]
Hypodontia could be found in different inheritance modes. It can occur as an isolated condition (nonsyndromic hypodontia)[3] or can be associated with systematic condition or syndrome (syndromic hypodontia).[4] Less frequently, hypodontia could be caused by environmental factors such as; infection, early irradiation of tooth germs, chemical substances or drugs, trauma in the dentoalveolar process, disturbances in the jaw innervations or accidental removal of a tooth germ during the extraction of a primary tooth.[5]
Several genes have been investigated to understand the genetic processes of tooth agenesis. A familial autosomal dominant point mutation in the MSX1 gene has been demonstrated with second premolar and third molar agenesis.[6] PAX9 gene in chromosome 14 has been also identified as responsible for autosomal dominant oligodontia.[3] Other studies reported that, in addition to MSX1 and PAX9 genes, a regulatory molecule in the mesenchyme, called transforming growth factor alpha, could result in isolated forms of dental agenesis.[7] Although tooth agenesis has been most frequently reported as inherited in an autosomal dominant or recessive fashions,[8,9] some reports demonstrated to be inherited as X-linked and polygenic fashions.[10]
The prevalence of hypodontia has been reported in different populations. Variation in the distribution and location has been reported across ethnic groups. A recent systematic review reported that the overall prevalence was 6.4% with the highest in Africa followed by Europe, Asia, and Australia. Lower prevalence was found in North America and Latin America and Caribbean. Hypodontia was found more frequently in females than males.[11]
Whilst hypodontia is not a common dental anomaly, it represents a clinical problem which requires multi-disciplinary approach due to complications that might arise such as, esthetic problems, periodontal damage, disturbances in occlusion and alveolar bone deficiency. Until date, there have been no published studies investigating the prevalence and distribution of hypodontia in the state of Qatar. Therefore, the aim of this study was to investigate the prevalence and distribution of hypodontia in the permanent teeth among a group of Qatari sample and to compare the present results with findings from other populations.
MATERIALS AND METHODS
This retrospective study examined the records of 1269 Qatari patients who attended the Pediatric Dentistry and Orthodontic Clinics during the period (2009–2014) at the Department of Dentistry, at Hamad Medical Corporation, Doha-State of Qatar. The inclusion criteria were patients of Qatari origin, no history of medical problem or any type of syndromes and developmental anomalies, the presence of panoramic radiograph with good quality and patients who aged between 8 and 20 years.
Ethical approval was obtained from the Medical Research Center at Hamad Medical Corporation, Doha-State of Qatar (Project number: 14077/14).
All permanent teeth except third molars were investigated using the panoramic radiographs. A tooth was recorded as congenitally missing when no trace could be found on the panoramic radiograph. Treatment records from patients’ files were checked to confirm that the tooth had not been extracted due to caries, periodontal disease, trauma or orthodontic extraction. Four experienced dentists who have at least 5 years of clinical experience examined all the radiographs over a period of 6 months. All radiographs were evaluated on viewers in a dark room.
Data obtained from panoramic radiographs and patients’ records were recorded according to gender, age, type and number of missing teeth, maxillary versus mandibular agenesis, right versus left side and unilateral versus bilateral.
All descriptive and comparative analyses were performed using the Statistical Package for the Social Sciences (version 20.0, SPSS Inc., Chicago, IL, USA). Student's t-test was employed to compare the chronological ages between male and female patients. To test the difference between male and female patients, maxillary versus mandibular agenesis, right versus left side and unilateral versus bilateral, Chi-square or Fisher's exact tests were employed. To test data quality, 10% of the data were randomly selected and reevaluated by one of the investigators 2 weeks after the initial examination so that 100% reproducibility was assured in the identification of congenital missing teeth. The level of significance was set at 0.05.
RESULTS
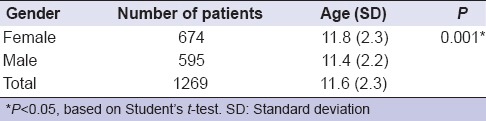
The study comprised of 674 female and 595 male patients. The mean age of female patients was 11.8 (±2.3) and for male patients was 11.4 (±2.2) [Table 1].
Table 1.
Descriptive data of patients included in the study
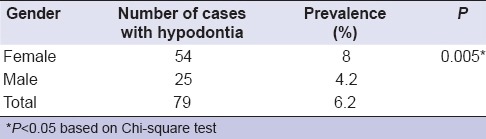
The prevalence of hypodontia was 6.2%. The difference between genders was statistically significant with female hypodontia prevalence higher than males (8% and 4.2%; respectively) [Table 2]. The teeth which showed statistical significance were maxillary right and left lateral incisors and maxillary right permanent second premolar.
Table 2.
Distribution of hypodontia by gender
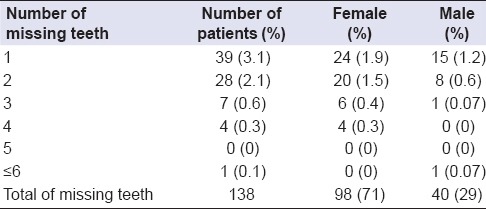
A total of 138 teeth were missing in 79 patients (98 in females [71%] and 40 in males [29%]). The average number of missing teeth per patient was 1.7. Of all patients, 39 had one missing tooth, 28 missing two, 7 missing three, 4 missing four and only one male patient with missing six or more teeth [Table 3].
Table 3.
Distribution of numbers of missing teeth among patients with hypodontia
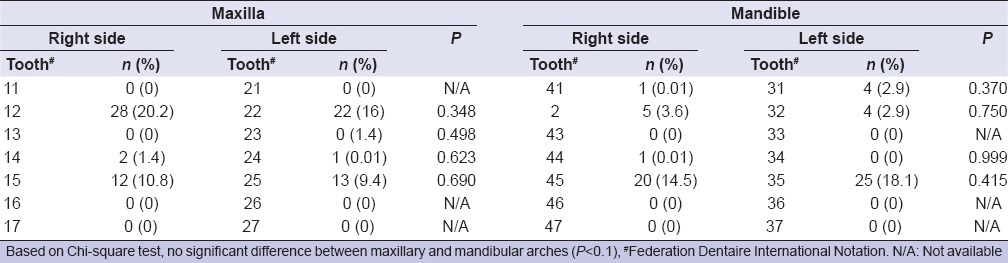
The most commonly missing teeth were maxillary lateral incisors (36.2%), followed by mandibular second premolars (32.6%) and maxillary second premolars (20.2%). However, there were no significant differences between right and left sides for any particular tooth [Table 4]. Hypodontia was more common in the maxilla (56.5%) than in the mandible (43.5%). However, this difference was not statistically significant (P < 0.1).
Table 4.
Frequency of missing teeth and test results in relation to right and left sides for a particular tooth in both arches
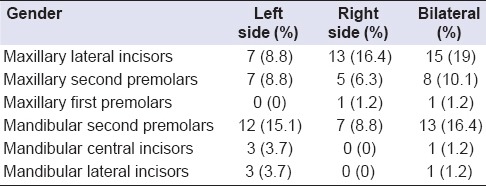
Bilateral missing teeth were found in 35 cases (44.3%). The most common bilateral missing teeth were maxillary lateral incisors (42.8%), followed by mandibular second premolar (37.1%). The maxillary lateral incisor was the most frequently unilaterally missing tooth (40%), followed by the mandibular second premolar (38%) [Table 5].
Table 5.
Frequency of missing teeth in relation to unilateral versus bilateral
DISCUSSION
Tooth development and morphogenesis is a complex process that involves interactions of different types of cell layers. This process is regulated by the presence of transcription factors and growth factors alongside their receptors.[12] Disruption of any part of this process will result in tooth anomaly. Hypodontia is one of the most common dental developmental disorders that require early diagnosis and management at an early age in order to prevent future complications. Many studies across different ethnic backgrounds reported on the prevalence and distribution of hypodontia. However, no data exist specific to the Qatari population. Hence, it was the aim of this study to investigate the prevalence and distribution of hypodontia in the permanent teeth among a group of the Qatari sample and to compare the present results with findings from other populations.
According to the present study, the prevalence of hypodontia was 6.2% which is similar to the findings of a recent systematic review conducted across populations in all continents.[11] When compared to other populations within the same region, this finding is higher with a maximum difference of 2%.[13,14,15] The reason for this difference could be due to lower sample sizes in other populations, which might affected the overall prevalence. As in most studies, the general prevalence of hypodontia was significantly higher in females (8%) than males (4.2%; P < 0.005).[4,16] The higher prevalence of hypodontia in female patients could be attributed to biological factors and the higher percentage of female patients attending the orthodontic and pediatric Dentistry clinics. However, few reports revealed no difference between both genders.[13,15]
The average number of missing teeth for each patient was 1.7%. Eighty-five percent of affected patients had one or two missing teeth. This is in agreement with other populations within the same region.[15] The fact that almost 15% of affected patients had at least 3 or more missing teeth could pose a clinical challenge with respect to management and will require a multi-disciplinary approach to correct functional and esthetic problems.
The most frequently missing tooth was the maxillary lateral incisor (36.2%), followed by mandibular second premolar (32.6%) and maxillary second premolar (20.2%). This finding is consistent with other previously reported data and confirms the general popular pattern in which the most distal tooth of any particular type is the most likely to be affected.[15,17] In contrast to these findings, several studies found that the most frequently missing tooth is the mandibular second premolar, followed by either maxillary second premolar or maxillary lateral incisor.[18,19,20] Other reports found that mandibular lateral incisor is the most commonly affected tooth, in particular, Asian populations.[21] These differences could be as a result of ethnicity or due to recruiting patients from different settings whether clinical or from the general population. For example, missing maxillary lateral incisor could be more frequently found in orthodontic clinics than from the general population.[22] In the present study, there were no significant differences between right and left sides for any particular tooth, which is in accordance with the majority of studies.[17,22] Furthermore, no significant difference was observed between both the maxillary and mandibular arches although hypodontia was more prevalent in the maxilla. This finding is consistent with most studies from the literature.[2] On the other hand, Mallineni et al.,[19] found that missing teeth in the mandibular arch was greater than the maxillary arch.
In the present study, bilateral missing of a particular tooth was found in 44.3% of affected cases. Although less prevalent than unilateral missing, this finding necessitates the urgent need for intervention and multi-disciplinary team approach for management. This finding was in agreement with a meta-analysis, which evaluated tooth agenesis of permanent teeth across different populations.[2] On the other hand, Amini et al.,[15] found that bilateral missing was observed about twice as frequently as unilateral missing. Bilateral missing was commonly seen in the maxillary lateral incisor followed by mandibular second premolar and maxillary second premolar (42.8%, 37.1% and 22.8%; respectively). This finding was consistent with previous reports.[15,22,23]
The results of the present study could have been confounded by several factors. The minimum age of the sample was 8 years old. In some individuals, delayed development of premolars might occur which may lead to uncertainty whether they are congenitally missing or not. Wisth et al.,[24] found that this uncertainty could be resolved when recruiting individuals at 9 years. A further limitation of the present study relates to the generalizability of the findings. Investigating the prevalence from general population will result in more reliable results and closer to the actual values. However, taking radiographs for the general population to identify hypodontia without any medical reason or indication would be unethical.
CONCLUSIONS
The prevalence of hypodontia in a group of the Qatari population was 6.2%, which was within the normal range of the majority of other populations. Hypodontia was more significantly prevalent in females as compared to males. The most commonly missing teeth were maxillary lateral incisors followed by mandibular second premolars. The majority of affected individuals had one or two missing teeth. Hypodontia was more commonly found unilaterally than bilaterally. There were no significant differences between right and left sides for any particular tooth.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared
REFERENCES
- 1.Hunstadbraten K. Hypodontia in the permanent dentition. ASDC J Dent Child. 1973;40:115–7. [PubMed] [Google Scholar]
- 2.Polder BJ, Van’t Hof MA, Van der Linden FP, Kuijpers-Jagtman AM. A meta-analysis of the prevalence of dental agenesis of permanent teeth. Community Dent Oral Epidemiol. 2004;32:217–26. doi: 10.1111/j.1600-0528.2004.00158.x. [DOI] [PubMed] [Google Scholar]
- 3.Frazier-Bowers SA, Guo DC, Cavender A, Xue L, Evans B, King T, et al. A novel mutation in human PAX9 causes molar oligodontia. J Dent Res. 2002;81:129–33. [PubMed] [Google Scholar]
- 4.Vastardis H. The genetics of human tooth agenesis: New discoveries for understanding dental anomalies. Am J Orthod Dentofacial Orthop. 2000;117:650–6. [PubMed] [Google Scholar]
- 5.Cakur B, Dagistan S, Miloglu O, Bilge M. Nonsyndromic oligodontia in permenant dentition: Three siblings. Internet J Dent Sci. 2006;3:2. [Google Scholar]
- 6.Vastardis H, Karimbux N, Guthua SW, Seidman JG, Seidman CE. A human MSX1 homeodomain missense mutation causes selective tooth agenesis. Nat Genet. 1996;13:417–21. doi: 10.1038/ng0896-417. [DOI] [PubMed] [Google Scholar]
- 7.Neubüser A, Peters H, Balling R, Martin GR. Antagonistic interactions between FGF and BMP signaling pathways: A mechanism for positioning the sites of tooth formation. Cell. 1997;90:247–55. doi: 10.1016/s0092-8674(00)80333-5. [DOI] [PubMed] [Google Scholar]
- 8.Alvesalo L, Portin P. The inheritance pattern of missing, peg-shaped, and strongly mesio-distally reduced upper lateral incisors. Acta Odontol Scand. 1969;27:563–75. doi: 10.3109/00016356909026309. [DOI] [PubMed] [Google Scholar]
- 9.Ahmad W, Brancolini V, ul Faiyaz MF, Lam H, ul Haque S, Haider M, et al. A locus for autosomal recessive hypodontia with associated dental anomalies maps to chromosome 16q12.1. Am J Hum Genet. 1998;62:987–91. doi: 10.1086/301799. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Erpenstein H, Pfeiffer RA. Sex-linked-dominant hereditary reduction in number of teeth. Humangenetik. 1967;4:280–93. doi: 10.1007/BF00292201. [DOI] [PubMed] [Google Scholar]
- 11.Khalaf K, Miskelly J, Voge E, Macfarlane TV. Prevalence of hypodontia and associated factors: A systematic review and meta-analysis. J Orthod. 2014;41:299–316. doi: 10.1179/1465313314Y.0000000116. [DOI] [PubMed] [Google Scholar]
- 12.Thesleff I, Nieminen P. Tooth morphogenesis and cell differentiation. Curr Opin Cell Biol. 1996;8:844–50. doi: 10.1016/s0955-0674(96)80086-x. [DOI] [PubMed] [Google Scholar]
- 13.al-Emran S. Prevalence of hypodontia and developmental malformation of permanent teeth in Saudi Arabian schoolchildren. Br J Orthod. 1990;17:115–8. doi: 10.1179/bjo.17.2.115. [DOI] [PubMed] [Google Scholar]
- 14.Albashaireh ZS, Khader YS. The prevalence and pattern of hypodontia of the permanent teeth and crown size and shape deformity affecting upper lateral incisors in a sample of Jordanian dental patients. Community Dent Health. 2006;23:239–43. [PubMed] [Google Scholar]
- 15.Amini F, Rakhshan V, Babaei P. Prevalence and pattern of hypodontia in the permanent dentition of 3374 Iranian orthodontic patients. Dent Res J (Isfahan) 2012;9:245–50. [PMC free article] [PubMed] [Google Scholar]
- 16.Fekonja A. Hypodontia in orthodontically treated children. Eur J Orthod. 2005;27:457–60. doi: 10.1093/ejo/cji027. [DOI] [PubMed] [Google Scholar]
- 17.Sisman Y, Uysal T, Gelgor IE. Hypodontia. Does the prevalence and distribution pattern differ in orthodontic patients? Eur J Dent. 2007;1:167–73. [PMC free article] [PubMed] [Google Scholar]
- 18.Behr M, Proff P, Leitzmann M, Pretzel M, Handel G, Schmalz G, et al. Survey of congenitally missing teeth in orthodontic patients in Eastern Bavaria. Eur J Orthod. 2011;33:32–6. doi: 10.1093/ejo/cjq021. [DOI] [PubMed] [Google Scholar]
- 19.Mallineni SK, Nuvvula S, Cheung A, Kunduru R. A comprehensive review of the literature and data analysis on hypo-hyperdontia. J Oral Sci. 2014;56:295–302. doi: 10.2334/josnusd.56.295. [DOI] [PubMed] [Google Scholar]
- 20.Aslan BI, Akarslan ZZ. Teeth number anomalies in permanent dentition among non-syndromic dental patients. Coll Antropol. 2013;37:115–20. [PubMed] [Google Scholar]
- 21.Chung CJ, Han JH, Kim KH. The pattern and prevalence of hypodontia in Koreans. Oral Dis. 2008;14:620–5. doi: 10.1111/j.1601-0825.2007.01434.x. [DOI] [PubMed] [Google Scholar]
- 22.Silva Meza R. Radiographic assessment of congenitally missing teeth in orthodontic patients. Int J Paediatr Dent. 2003;13:112–6. doi: 10.1046/j.1365-263x.2003.00436.x. [DOI] [PubMed] [Google Scholar]
- 23.Karadas M, Celikoglu M, Akdag MS. Evaluation of tooth number anomalies in a subpopulation of the North-East of Turkey. Eur J Dent. 2014;8:337–41. doi: 10.4103/1305-7456.137641. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Wisth PJ, Thunold K, Böe OE. Frequency of hypodontia in relation to tooth size and dental arch width. Acta Odontol Scand. 1974;32:201–6. doi: 10.3109/00016357409002548. [DOI] [PubMed] [Google Scholar]