

Abstract
Objective:
This prospective study investigated moderator variable models of the interrelationships among stressful events, coping motives for drinking, and current alcohol use on subsequent alcohol use across a 5-year window with middle-aged adults.
Method:
Data from women (n = 716; Mage = 55.29 years at baseline) and men (n = 505; Mage = 57.57 years at baseline) were used to examine theory-guided hypotheses that current levels of alcohol use would interact with stressful events and coping motives for drinking to predict higher levels of alcohol use across time. Analyses were conducted separately for men and women.
Results:
After we controlled for several potentially important covariates (i.e., age, educational level, family income, and marital status), prospective regression analyses supported moderator effects for current alcohol use and stressful events as predictors of changes in alcohol use, and a somewhat weaker consistency of moderator effects for current alcohol use and coping motives for drinking as predictors of changes in alcohol use. For example, higher levels of baseline alcohol involvement in conjunction with higher levels of stress predicted higher levels of alcohol use and alcohol problems 5 years later. Similarly, higher levels of coping motives and higher levels of heavy episodic drinking predicted higher levels of heavy episodic drinking among women 5 years later.
Conclusions:
The findings were discussed from an alcohol–stress vulnerability model of affect regulation and a positive regulatory feedback loop perspective wherein conditional relationships among baseline alcohol use indicators, stressful events, and coping drinking motives predicted greater alcohol involvement, especially problematic use, across time.
Considerable evidence has been marshaled supporting significant associations between stress and alcohol use, as well as alcohol problems and relapse (Pohorecky, 1991; Sayette, 1999; Wills & Shiffman, 1985). To explain the alcohol–stress relationship, conceptual models such as the Tension Reduction Hypothesis (Conger, 1956) and the affect regulation model (Cooper et al., 1995; Wills & Shiffman, 1985) have proposed that people consume alcohol to reduce the tension (e.g., anxiety, depression, distress) associated with stressful events (Cooper et al., 1997). To the extent that alcohol reduces the negative affect associated with stress, the consumption of alcohol serves as a positive reinforcer that may be learned and fostered across time.
The conceptual orientation used in this study builds on this prior research on alcohol and stress and is referred to as the alcohol–stress vulnerability model. This model has its origins historically in the diathesis–stress model of psychopathology (Zuckerman, 1999) and has been a prominent model used in research on depression and substance use disorders (Hankin & Abramson, 2001; Windle, 2010). The fundamental notion underlying this model is that people vary in their individual responses (vulnerabilities) to stressful events in systematic ways that are related to the probability of occurrence of outcomes such as depression, or in our case, increased alcohol use. The adoption of an alcohol–stress vulnerability model is consistent with considerable prior research and theorizing related to substance use disorders about how the use of alcohol (and other substances) may reduce stress via self-medication and the regulation of positive and negative affective states (Cooper et al., 1992a; Khantzian, 1997; Wills & Shiffman, 1985).
Of interest in the current study are the potentially moderating effects of both coping motives for drinking and current (baseline) alcohol use on the prospective alcohol–stress relationship. These two moderating variables are conceptualized as vulnerability factors that will interact with stressful events to predict higher levels of alcohol use across time. Coping motives for drinking reflect endorsements by participants that they use alcohol in response to aversive life events to reduce and regulate negative affect (Cooper, 1994; Cooper et al., 1992b, 1995). Previous research has found that individuals who use alcohol as a coping mechanism are at increased risk both to consume larger quantities of alcohol and to experience more negative consequences associated with their alcohol use (Holahan et al., 2003; Windle, 2000). Level of alcohol involvement (i.e., from use to heavy use to problematic use), especially problematic involvement, is also viewed as a potential vulnerability factor in that the current stress–alcohol relationship may have been preceded by a history of reciprocal relationships between stress and alcohol. That is, current levels of alcohol and stress may represent a “snapshot” in time of an ongoing positive regulatory feedback loop (or an escalating iterative pattern) of stress→alcohol use→increased stress→increased alcohol use, etc.
Current study
Based on the alcohol–stress vulnerability model, we investigated how individual vulnerabilities (i.e., baseline alcohol involvement and coping motives) may interact with stressors to predict future alcohol involvement. We used data from a two-wave, 5-year-interval prospective study with a community sample of middle-aged adults. We used longitudinal regression analyses to investigate relationships among three alcohol use indicators (i.e., quantity–frequency index [QFI] of alcohol use, heavy episodic drinking [HED], and alcohol problems), stressful events, and coping motives for drinking, along with their interactions, in the prediction of alcohol use indicators 5 years later. Although the three alcohol indicators used in this study are significantly correlated, considerable research supports unique relationships between predictors such as coping motives for drinking and alcohol problems (e.g., Cooper, 1994; Windle, 2000), as well as stressful events and problematic alcohol use (Holahan et al., 2001).
Several methodological features of this study will advance the literature in important ways. First, our study complements and extends the current literature by expanding the time window to investigate the relationships of interest across a longer term (5-year) window than extant cross-sectional and shorter term longitudinal studies. Second, studies have investigated either the alcohol–stress relationship (Brennan et al., 1999, 2005; Kuipers et al., 2012) or the drinking-to-cope–alcohol relationship (Crutzen et al., 2013; Holahan et al., 2001); our study includes three alcohol indicators, stressful events, and coping drinking motives in a prospective study of middle-aged adults. The study of drinking practices and their causes is of importance in middle age because heavier alcohol use among this population has been associated with a host of medical conditions, including cardiovascular and cerebrovascular diseases, cancer, and gastrointestinal disorders (Roerecke & Rehm, 2012), as well as compromised psychological functioning (Choi & DiNitto, 2011a, 2011b). Moreover, health behaviors (e.g., the consumption of alcohol) in middle age portend cognitive, physical, and emotional functioning and health in older adulthood (Lachman, 2004), thereby suggesting their importance to a developmental orientation of disease prevention and health promotion across the life span. Third, a number of studies have indicated sex differences in alcohol–stress relationships (Brennan et al., 1999, 2005; Cooper et al., 1992a; Glass et al., 1995; Kuipers et al., 2012); as such, we conducted analyses separately for men and women.
Study hypotheses
Based on the alcohol–stress vulnerability model, our hypotheses reflect the notion that individual vulnerabilities (conceptualized as baseline alcohol involvement and baseline coping motives for drinking) will interact with stressors (conceptualized as being strongly related to negative affect regulation) to prospectively predict alcohol use outcomes 5 years later (Cooper et al., 1992a; Glass et al., 1995). The three hypotheses are as follows.
Hypothesis 1.
The vulnerability factor of higher levels of baseline alcohol involvement in conjunction with higher levels of stress will predict higher levels of alcohol outcomes.
Hypothesis 2.
Higher levels of baseline coping motives and alcohol involvement will predict higher levels of alcohol outcomes.
Hypothesis 3.
Higher levels of baseline coping motives in conjunction with higher levels of stress will predict higher levels of alcohol outcomes.
For each of the aforementioned hypotheses, we propose that these interactions will be of a higher magnitude for problematic alcohol involvement indicators (i.e., HED, alcohol problems) relative to QFI (Cooper, 1994; Kuntsche et al., 2005; Windle 2000).
Method
Participants
The data used in this study were collected from a sample of middle-aged men and women who participated at Waves 6 and 7 of a larger, seven-wave, 23-year prospective study focused on risk factors for adolescent and young adult substance use and mental health (see Windle et al., 2005). The men and women in the current study are the parents of the adolescent/young adult target sample. Primary caregiver’s participation during Wave 1–Wave 4 was limited to reporting on potential risk factors for adolescents (e.g., family income, parent’s education levels) via mail surveys (adolescents were assessed in school settings). During Waves 5–7 (three waves of assessment at 5-year intervals), the primary targets for study were expanded to include not only the adolescents as they transitioned to young adulthood, but also the parents of these young adult children, and interviews were conducted with each participating member. This study was reviewed and approved by the Institutional Review Board of the University at Buffalo. Signed informed consent was obtained from participants before each wave of assessment.
The participation rate for the adolescent sample was 76% (n = 1,205), which is relatively high for in-school assessments that require active informed consent (Tigges, 2003). At Waves 5–7, the study retained 87% of the adolescent sample (n = 1,050); participants were lost primarily because of difficulties in contacting them and because of refusals. Among this sample of 1,050 adolescents, the following data refer to their parents who were contacted for participation at Waves 5–7.
For women (mothers of the adolescents), 47 (4.5%) died at some point between Waves 5 and 7, 156 (14.8%) did not participate, and 847 (80.7%) participated during the 10-year follow-up, yielding a participation rate of 84% if the deceased are excluded from the denominator. For men (fathers of the adolescents), analogous statistics were 103 (9.8%) were deceased, 350 (33.3%) did not participate, and 597 (56.9%) participated during the 10-year follow-up, thus yielding a participation rate of 63% if the deceased are excluded from the denominator. Although this reflects a lower participation rate for fathers than preferred, it exceeds the standard rate of participation by fathers in behavioral science studies of families (Phares & Compas, 1992). Across the three waves of assessment, the retention rate for men was 72% (Waves 5–6) and 86% (Waves 6–7); the retention rate for women was 73% (Waves 5–6) and 85% (Waves 6–7).
A criterion for inclusion in this study was that participants had to have reported having a drink in the previous 6 months (this was necessary because respondents could not report on coping motives for drinking if they did not drink). This resulted in the deletion of 88 women and 48 men who had not consumed alcohol in the past 6 months at Wave 6. In addition, 43 women and 44 men were excluded because of missing data.
Extensive attrition analyses were conducted comparing several of the exclusion groups (e.g., parents who died across the course of the study; parents who were excluded because they did not consume alcohol in the past 6 months at Wave 6) with those who participated. These analyses, described in more detail elsewhere (Windle & Windle, 2014), provided no evidence of selective dropout with regard to alcohol use, stressful events, or sociodemographic variables.
Procedure
At Wave 6, one-on-one interviews were conducted either in the subjects’ homes or at the investigators’ host institute. Subjects were paid $40 to complete an interview that lasted approximately 2 hours. Computer-assisted personal interviews were used to collect data. At Wave 7, because of budgetary cuts to the research project, mail surveys (rather than face-to-face interviews) were completed by participants and returned in self-addressed, stamped envelopes. Participants were paid $20 for completion of the mail survey, which took approximately 45–60 minutes to complete.
Measures
Middle-aged adults’ sociodemographic variables.
In their individual interviews and the completion of mail surveys, participants were asked about their age, number of years of education completed, family income, and other status indicators (e.g., marital and occupational status).
Stressful life events.
Stressful life events were assessed with an adaptation of the Holmes and Rahe scale (1967). Participants were asked to report on stressful events that occurred within the past 12 months. Forty-six events were scored as an aggregate measure of stressors, with events covering domains of work stressors, interpersonal stressors, health concerns–self, health concerns–others, financial stressors, and criminal/legal stressors.
Coping motives for drinking.
Coping motives for drinking was assessed using a five-item subscale from the self-report measure developed by Cooper et al. (1992b). Items included “drinking to forget your worries” and “drinking because it helps when you feel depressed or nervous.” Internal consistency estimates across waves of assessment ranged from .88 to .92 for women and .89 to .90 for men. Although coping motives for drinking could vary as a function of treatment and other state-like influences (e.g., variability in number or intensity of stressors), in community samples they are relatively stable dispositions across time, as indicated by a test–retest Pearson correlation of .71 across the 5-year interval in this study.
Alcohol use (Quantity–Frequency Index).
Alcohol use was measured at each wave with a standard QFI that assessed consumption of beer, wine, and distilled spirits in the past 6 months (Armor & Polich, 1982). Respondents were asked how often they usually had each beverage in the last 6 months (1 = never to 7 = every day) and, when they had the beverage, on average how much they usually drank (10-point scale from 1 = none to 10 = more than eight cans, bottles, or glasses, depending on the beverage). The resulting index provides a measure of the average number of ounces of ethanol consumed per month over the past 6 months. A logarithmic transformation was applied to the resulting consumption values.
Heavy episodic drinking.
HED was assessed at each wave with questions about the frequency of drinking six or more alcoholic beverages on a single occasion over the past 6 months. HED was assessed for each alcoholic beverage (i.e., beer, wine, distilled spirits), and a summed score was created to measure the number of occasions of HED. Our “six or more drinks” threshold for HED was consistently used throughout the course of this long-term longitudinal study that was initiated before the more recent 5 (for men) and 4 (for women) HED thresholds used in current research. As such, the prevalence of HED may be underrepresented in this study.
Alcohol problems.
Alcohol problems were assessed somewhat differently across Wave 6 and Wave 7. At Wave 6, alcohol problems were assessed via 15 items that were designed to assess a range of undesirable consequences of drinking alcohol during the previous 6 months. Items measured experiences during or as a consequence of alcohol use in the domains of work (e.g., drinking during work, missing work), conflict in social relationships (e.g., with spouse/fiancé, with strangers, with the police), compulsive drinking style (drinking alone, drinking to cure a hangover, drinking on consecutive days, drinking to forget troubles), and loss of behavioral control (e.g., passing out, thinking about the need to cut down, regretting things done while drinking). At Wave 7, we reduced the number of alcohol problems presented to participants from 15 to 7. This was done in an effort to reduce the burden on participants completing the mail survey.
Eight items were deleted at Wave 7 based on their low prevalence rate at Wave 6. The seven items maintained at Wave 7 covered domains of conflict in social relationships, loss of behavioral control, and compulsive drinking style. At Wave 6, each item used a 5-point Likert scale (0 times, 1–2, 3–5, 6–10, >10 times). At Wave 7, each item used a 3-point Likert scale (0 times, 1–2 times, ≥3 times). Internal consistency estimates across waves of assessment ranged from .75 to .73 for women and .88 to .65 for men.
Statistical analyses plan
For those participants included in the current study (716 women and 505 men), missing value estimation using the expectation-maximization algorithm was used to estimate the missing data under the missing-at-random assumption; approximately 20% of the data were estimated. (Note that we excluded from the analyses participants who died between Wave 5 and Wave 7 [n = 150]; those who did not drink alcohol in the past 6 months [n = 136]; and those who completed some components of the data collection protocol, such as the psychiatric diagnostic section, but not other components, such as the alcohol and drinking motives section [n = 87].)
For the primary analyses, hierarchical multiple regression analyses were conducted for the Wave 6–Wave 7 relationships. We controlled for sociodemographic variables, prior alcohol use, stressful events, and coping motives in each of these prospective regression equations. Controlling for these variables in the regression equations was important for two reasons: (a) we controlled for possible covariates and predictors that could otherwise provide alternative explanations for the prospective moderator relationships findings, and (b) we controlled for the covariates and predictors, allowing us to interpret significant findings of moderator effects as predicting changes (e.g., increases) in alcohol use time.
Results
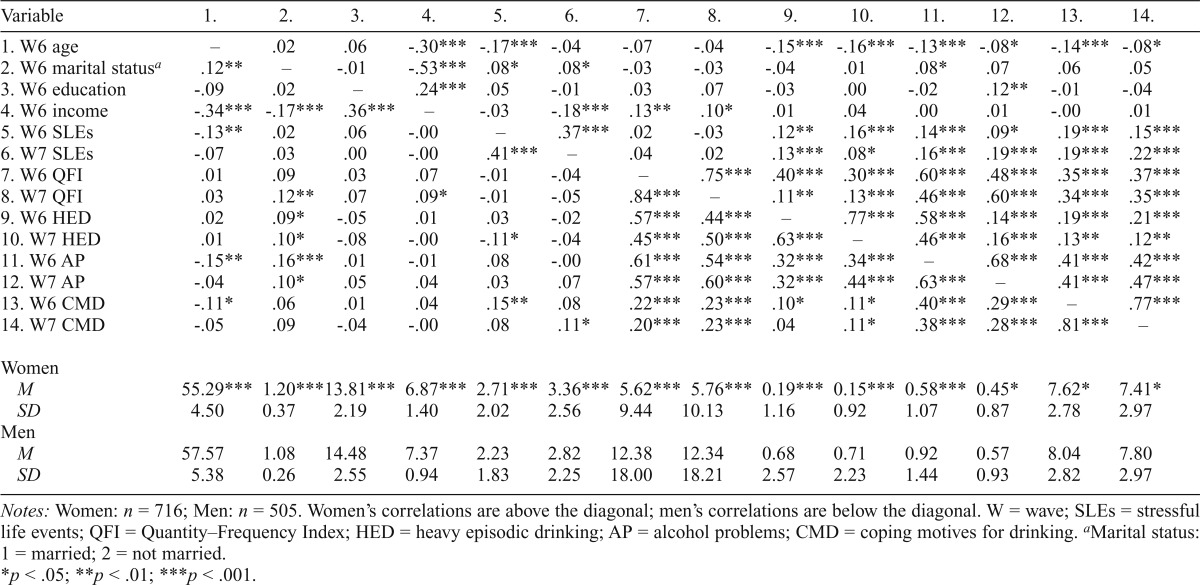
Table 1 provides the correlation matrix and means and standard deviations for the variables used in the regression analyses in this study. Men and women differed significantly with regard to mean level comparisons on all variables (see bottom of table). In addition, although not shown in the table, more than 50% of the sample reported the use of alcohol to cope, with 53% of women and 64% of men using alcohol to cope at least sometimes and 10% of women and 14% of men reporting the use of coping motives for drinking fairly often or almost always.
Table 1.
Correlations and descriptive statistics for study variables
| Variable | 1. | 2. | 3. | 4. | 5. | 6. | 7. | 8. | 9. | 10. | 11. | 12. | 13. | 14. |
| 1. W6 age | . – | .02 | .06 | -.30*** | -.17*** | -.04 | -.07 | -.04 | -.15*** | -.16*** | -.13*** | -.08* | -.14*** | -.08* |
| 2. W6 marital statusa | .12** | . – | -.01 | -.53*** | .08* | .08* | -.03 | -.03 | -.04 | .01 | .08* | .07 | .06 | .05 |
| 3. W6 education | -.09 | .02 | . – | .24*** | .05 | -.01 | .03 | .07 | -.03 | .00 | -.02 | .12** | -.01 | -.04 |
| 4. W6 income | -.34*** | -.17*** | .36*** | . – | -.03 | -.18*** | .13** | .10* | .01 | .04 | .00 | .01 | -.00 | .01 |
| 5. W6 SLEs | -.13** | .02 | .06 | -.00 | . – | .37*** | .02 | -.03 | .12** | .16*** | .14*** | .09* | .19*** | .15*** |
| 6. W7 SLEs | -.07 | .03 | .00 | -.00 | .41*** | . – | .04 | .02 | .13*** | .08* | .16*** | .19*** | .19*** | .22*** |
| 7. W6 QFI | .01 | .09 | .03 | .07 | -.01 | -.04 | – | .75*** | .40*** | .30*** | .60*** | .48*** | .35*** | .37*** |
| 8. W7 QFI | .03 | .12** | .07 | .09* | -.01 | -.05 | .84*** | – | .11** | .13*** | .46*** | .60*** | .34*** | .35*** |
| 9. W6 HED | .02 | .09* | -.05 | .01 | .03 | -.02 | .57*** | .44*** | – | .77*** | .58*** | .14*** | .19*** | .21*** |
| 10. W7 HED | .01 | .10* | -.08 | -.00 | -.11* | -.04 | .45*** | .50*** | .63*** | – | .46*** | .16*** | .13** | .12** |
| 11. W6 AP | -.15** | .16*** | .01 | -.01 | .08 | -.00 | .61*** | .54*** | .32*** | .34*** | – | .68*** | .41*** | .42*** |
| 12. W7 AP | -.04 | .10* | .05 | .04 | .03 | .07 | .57*** | .60*** | .32*** | .44*** | .63*** | – | .41*** | .47*** |
| 13. W6 CMD | -.11* | .06 | .01 | .04 | .15** | .08 | .22*** | .23*** | .10* | .11* | .40*** | .29*** | – | .77*** |
| 14. W7 CMD | -.05 | .09 | -.04 | -.00 | .08 | .11* | .20*** | .23*** | .04 | .11* | .38*** | .28*** | .81*** | .– |
| Women | ||||||||||||||
| M | 55.29*** | 1.20*** | 13.81*** | 6.87*** | 2.71*** | 3.36*** | 5.62*** | 5.76*** | 0.19*** | 0.15*** | 0.58*** | 0.45* | 7.62* | 7.41* |
| SD | 4.50 | 0.37 | 2.19 | 1.40 | 2.02 | 2.56 | 9.44 | 10.13 | 1.16 | 0.92 | 1.07 | 0.87 | 2.78 | 2.97 |
| Men | ||||||||||||||
| M | 57.57 | 1.08 | 14.48 | 7.37 | 2.23 | 2.82 | 12.38 | 12.34 | 0.68 | 0.71 | 0.92 | 0.57 | 8.04 | 7.80 |
| SD | 5.38 | 0.26 | 2.55 | 0.94 | 1.83 | 2.25 | 18.00 | 18.21 | 2.57 | 2.23 | 1.44 | 0.93 | 2.82 | 2.97 |
Notes: Women: n = 716; Men: n = 505. Women’s correlations are above the diagonal; men’s correlations are below the diagonal. W = wave; SLEs = stressful life events; QFI = Quantity–Frequency Index; HED = heavy episodic drinking; AP = alcohol problems; CMD = coping motives for drinking.
Marital status: 1 = married; 2 = not married.
p < .05;
p < .01;
p < .001
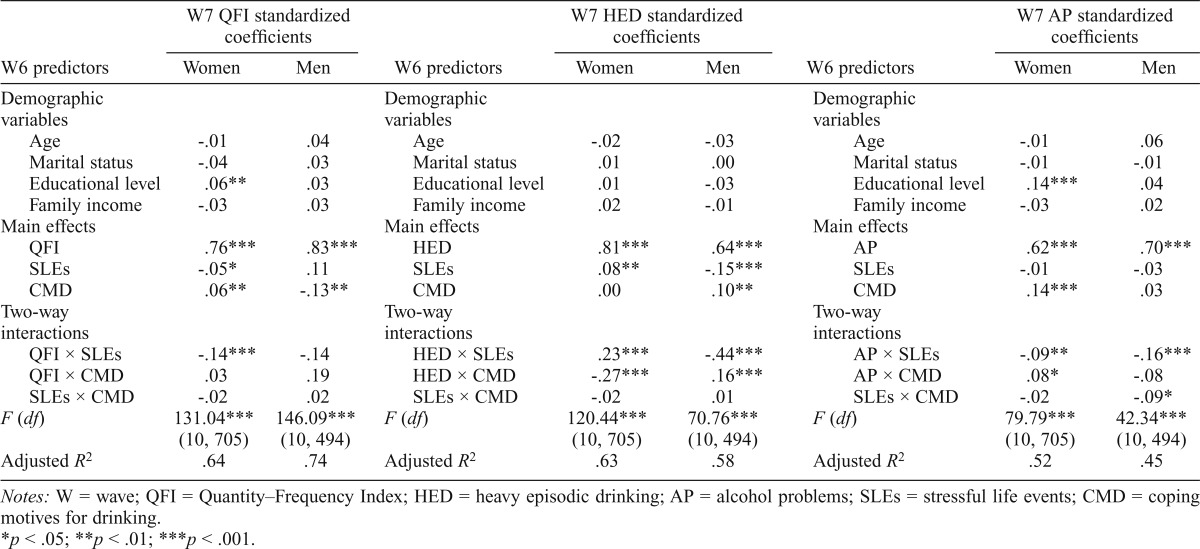
The findings for the longitudinal multiple regression analyses are summarized in Table 2. Of the 18 interactions tested (9 for women and 9 for men), 9 were statistically significant (5 for women and 4 for men). The directionality and plotting of the statistically significant interactions indicated two general patterns. First, for those beta coefficients that were negative (6 of the 9 significant interactions), the general pattern indicated that higher levels of the moderator variable (e.g., alcohol use indicator) in combination with higher levels of the independent variable (e.g., stressful events) were associated with greater increases in the alcohol outcome variables. This pattern is illustrated in Figure 1 for women, where higher levels of Wave 6 QFI, in combination with higher levels of Wave 6 stressful events, yielded higher levels of Wave 7 QFI and an increased acceleration rate of change (i.e., the slope is increasing more rapidly), similar to the well-known stress exacerbation effect.
Table 2.
Results from regression analyses for women’s and men’s Wave 6 predictors → Wave 7 alcohol outcomes
| W6 predictors | W7 QFI standardized coefficients |
W6 predictors | W7 QFI standardized coefficients |
W6 predictors | W7 AP standardized coefficients |
|||
| Women | Men | Women | Men | Women | Men | |||
| Demographic variables | Demographic variables | Demographic variables | ||||||
| Age | -.01 | .04 | Age | -.02 | -.03 | Age | -.01 | .06 |
| Marital status | -.04 | .03 | Marital status | .01 | .00 | Marital status | -.01 | -.01 |
| Educational level | .06** | .03 | Educational level | .01 | -.03 | Educational level | .14*** | .04 |
| Family income | -.03 | .03 | Family income | .02 | -.01 | Family income | -.03 | .02 |
| Main effects | Main effects | Main effects | ||||||
| QFI | .76*** | .83*** | HED | .81*** | .64*** | AP | .62*** | .70*** |
| SLEs | -.05* | .11 | SLEs | .08** | -.15*** | SLEs | -.01 | -.03 |
| CMD | .06** | -.13** | CMD | .00 | .10** | CMD | .14*** | .03 |
| Two-way interactions | Two-way interactions | Two-way interactions | ||||||
| QFI × SLEs | -.14*** | -.14 | HED × SLEs | .23*** | -.44*** | AP × SLEs | -.09** | -.16*** |
| QFI × CMD | .03 | .19 | HED × CMD | -.27*** | .16*** | AP × CMD | .08* | -.08 |
| SLEs × CMD | -.02 | .02 | SLEs × CMD | -.02 | .01 | SLEs × CMD | -.02 | -.09* |
| F (df) | 131.04*** (10, 705) | 146.09*** (10, 494) | F (df) | 120.44*** (10, 705) | 70.76*** (10, 494) | F (df) | 79.79*** (10, 705) | 42.34*** (10, 494) |
| Adjusted R2 | .64 | .74 | Adjusted R2 | .63 | .58 | Adjusted R2 | .52 | .45 |
Notes: W = wave; QFI = Quantity–Frequency Index; HED = heavy episodic drinking; AP = alcohol problems; SLEs = stressful life events; CMD = coping motives for drinking.
p < .05;
p < .01;
p < .001
Figure 1.

Women’s Wave 6 (W6) Stressful Life Events × W6 Quantity–Frequency Index (QFI) interaction predicting Wave 7 (W7) QFI. No. = number.
In contrast, lower levels of Wave 6 QFI and higher levels of Wave 6 stressful events yielded lower levels of Wave 7 QFI and a less rapid acceleration rate of change (i.e., the slope is increasing more slowly), similar to the well-known stress-buffering effect. Following standard regression procedures (Aiken & West, 1991), we plotted the simple slopes at ±1 SD from the intercepts, and the beta coefficients for the respective slopes were both statistically significant (p < .01 for Wave 6 High QFI; p < .05 for Wave 6 Low QFI). A similar pattern was indicated for alcohol problems and stressful events for both men and women, for HED and stressful events for men, and for HED and coping motives for women. For example, higher levels of the Wave 6 alcohol variable in combination with higher stressful events were associated with higher levels and a more rapid rate of increase for the Wave 7 alcohol outcome variable. By contrast, lower levels of the Wave 6 alcohol variable in combination with higher stressful events were associated with lower levels and a slower rate of increase for the Wave 7 alcohol outcome variable.
This general pattern associated with significant negative interaction terms was also indicated for men with regard to the Stressful Events × Coping Motives interaction on Alcohol Problems (Figure 2). Those at higher levels of Wave 6 coping motives and higher levels of stressful events had higher levels of and a more rapid rate of increase of Wave 7 alcohol problems. By contrast, those at lower levels of Wave 6 coping motives and higher levels of stressful events had lower levels of and a slower rate of increase of Wave 7 alcohol problems. The simple slopes at ±1 SD from the intercepts and the beta coefficients for the respective slopes were both statistically significant (p < .01).
Figure 2.

Men’s Wave 6 (W6) Stressful Life Events × W6 Coping Motives for Drinking (CMD) interaction predicting Wave 7 (W7) alcohol problems (AP)
The second general pattern was for those beta coefficients that were positive (three of the nine significant interactions). This general pattern indicated that lower levels of the moderator variable in combination with higher levels of the independent variable were associated with higher, rather than lower, levels of increases in the alcohol outcome variables. This pattern is illustrated in Figure 3 for women, where lower levels of Wave 6 alcohol problems in combination with higher levels of Wave 6 coping motives yielded higher levels of Wave 7 alcohol problems and a greater acceleration rate of change (i.e., the slope is increasing more rapidly). By contrast, for those with higher levels of Wave 6 alcohol problems and higher levels of Wave 6 coping motives, there was only a small increase in the levels of Wave 7 alcohol problems and a slower acceleration with regard to the rate of change (i.e., the slope is increasing more slowly). The simple slopes at ±1 SD from the intercepts and the beta coefficients for the respective slopes were both statistically significant (p < .05 for Wave 6 high alcohol problems and p < .01 for Wave 6 low alcohol problems).
Figure 3.

Women’s Wave 6 (W6) Coping Motives for Drinking × W6 Alcohol Problems (AP) interaction predicting Wave 7 (W7) AP
This pattern was also indicated for women with regard to HED and stressful events. That is, for women with lower levels of Wave 6 HED and higher stressful events, there was a greater increase in levels of HED at Wave 7 than for women at higher levels of Wave 6 HED and higher stressful events. Likewise, this pattern was indicated for men with regard to HED and coping motives. For men with lower levels of Wave 6 HED and higher coping motives, there was a greater increase in levels of HED at Wave 7 than for men at higher levels of Wave 6 HED and higher coping motives. The simple slopes at ±1 SD from the intercepts and the beta coefficients for the respective slopes of these regression equations were both statistically significant (p < .01).
Discussion
Epidemiologic studies have indicated that the majority of middle-aged and older adults who consume alcohol do so at low to moderate levels, but that there is a subset whose high levels of alcohol use and HED result in adverse consequences (e.g., social, health) for themselves and others (Windle & Windle, 2014). As such, it is important to understand longitudinal patterns of alcohol use and moderators of accelerated use that result in higher levels of unhealthy use among middle-aged and older adults.
In the current study, an alcohol–stress vulnerability model was used to derive hypotheses and interpret findings related to the alcohol–stress relationship for a middle-aged sample. We posited that individual-level vulnerabilities, such as initial heavy alcohol involvement (i.e., HED and alcohol problems) and a reliance on alcohol to cope, in interaction with stressful events, would predict higher levels of maladaptive alcohol involvement across time. The findings indicated that the model was generally supported.
Using prospective regression analyses that included tests of moderators, 9 of 18 two-way interactions were significant predictors of levels of alcohol involvement approximately 5 years later among middle-aged adults. With some notable exceptions (discussed below), this study’s hypotheses related to interactions between baseline alcohol indicators by stressful events and baseline alcohol indicators by coping motives were supported. That is, two patterns of significant interactions were indicated—one pattern with negative interactions and one with positive interactions.
First, with regard to the negative interactions, in support of our study hypotheses, four negative interactions represented a longitudinal pattern of alcohol use by which higher levels of the baseline alcohol indicator interacted with higher stressful events to predict higher levels and more rapid increases in subsequent alcohol use. Two additional negative interactions indicated that, within the context of higher levels of HED (for women) and higher levels of stressful events (for men), middle-aged adults who at baseline reported a reliance on the use of alcohol as a coping mechanism reported more problematic alcohol use (HED for women and alcohol problems for men) 5 years later. These findings are consistent with an alcohol–stress vulnerability model in that they support moderators (vulnerabilities) that interact with stress to predict higher levels of problematic alcohol use across time.
This pattern of alcohol involvement is also consistent with a positive regulatory feedback loop in that middle-aged adults who reported greater alcohol involvement at baseline may have used alcohol to cope with the negative affect associated with stressors, which, in turn, resulted in higher levels of alcohol involvement across time. In support of this contention, Brennan et al. (1999) found reciprocal relations between stressful events and alcohol problems across a 4-year period. Holahan et al. (2001) found that drinking to cope was concurrently and prospectively (1 year later) related to high levels of alcohol consumption and alcohol problems among a mixed-sex sample. In addition, alcohol involvement and drinking to cope increased and decreased synchronously across the 10- year period of this study.
Wills and Shiffman (1985) raised a cautionary note regarding the use of substances as a coping strategy when they wrote, “Although substances may provide short-term changes in affect, a reliance on this approach for dealing with environmental stressors reduces the probability of learning and practicing alternative coping responses; in the long run this would tend to reduce social competence and increase overall stress levels” (p. 8). Not only might a reliance on an alcohol-use coping response lead to a loss of social competence and to higher stress levels, but as indicated in the current findings, it also leads to significantly higher levels of HED and alcohol problems across time.
Second, with regard to the positive interactions, three significant positive interactions ran contrary to our hypotheses. That is, among adults who initially reported lower levels of HED and alcohol problems, their baseline alcohol involvement interacted with high baseline levels of coping motives and stressful events that resulted in a greater acceleration of the alcohol indicators 5 years later. Thus, for these interactions, lower levels of the baseline alcohol indicator did not operate as a stress-buffering mechanism.
Three important points should be noted in relation to these findings. The first important point to consider is that the data indicated that a plausible explanation for these positive interactions is a statistical ceiling effect. Thus, for each interaction, those adults who reported high baseline levels of the alcohol indicators experienced minimal rates of increase in their alcohol involvement across time independent of baseline levels of coping motives and stressful events. That is, they were already at initially high levels of alcohol use, and therefore the change in their levels of alcohol involvement was negligible across the 5 years. In contrast, those who reported lower levels of alcohol involvement at baseline, in conjunction with high levels of coping motives or stressful events, experienced a greater rate of increase in the alcohol indicators (although their levels of alcohol involvement 5 years later never attained the level of the heavier alcohol users).
The second important point to consider is that, from a theoretical perspective, there is coherence to the notion that individuals who report initially low levels of alcohol involvement within the context of risk factors such as high levels of coping motives and stressful events might increase their alcohol use across time. That is exactly what the positive interactions reflect. Thus, although these findings run counter to our hypotheses, they are nevertheless theoretically plausible. The third important point to consider is that, although we do not have an explanation for why the directionality of the interactions for these specific variables (relative to the other six significant negative interactions) ran counter to our expectations, we contend that it is the pattern of the interactions that is important to recognize. That is, in some instances, high levels of coping motives and stressful events represent significant risk factors for future unhealthy levels of alcohol use even among those middle-aged adults whose alcohol involvement is initially at lower levels.
Our third hypothesis that the interaction between baseline coping motives and stressful events would predict an accelerated rate of increase in the alcohol outcomes was not supported, except for one interaction. As shown in Figure 2, men with higher levels of baseline coping motives and stressful events experienced a significant rate of increase of alcohol problems 5 years later. A possible explanation for the lack of overall support for our third hypothesis was that variance associated with this effect could already have been captured, or accounted for, by the Alcohol Use × Stressful Events interaction. That is, the Alcohol Use × Stressful Events interaction may have incorporated longer term patterns of regulatory relationships, including coping motives; as such, the Coping Motives × Stressful Events interaction terms added no unique variance in the prospective equations.
Included in all three hypotheses was the notion that the interaction terms would be more consistently and robustly associated with problematic alcohol use, that is, HED and alcohol problems, relative to the more general QFI measure of alcohol use (Cooper, 1994; Holahan et al., 2001). In support of this hypothesis, only one of the interaction terms, the Baseline QFI × Stressful Events interaction for women, predicted higher alcohol use at follow-up (Figure 1). The absence of significant interaction effects on the QFI measure suggested that nonproblematic alcohol use is a more “benign” indicator of alcohol involvement. That is, we concur with Brennan et al. (1999), who suggested that this pattern of more normative drinking may indicate that alcohol consumption in some contexts (e.g., drinking within the social context of friends, greater attendance at social outlets such as parties and weddings where drinking occurs) reflects better adaptation and integration into social networks among middle-aged adults. By contrast, coping motives and alcohol–stress findings have been associated with more alcohol problems and problem drinking (Cooper, 1994; Kuntsche et al., 2005).
Last, although we did not have a priori hypotheses related to gender differences, our findings were consistent in suggesting that the negative and positive patterns of interactions were significant for men and women, despite significant differences across gender with regard to mean levels of the study variables (see bottom of Table 1). That is, of the nine significant interaction terms, five were significant for women and four were significant for men. These findings suggest that patterns of alcohol use that involve higher levels of coping motives and stressful events represent risk factors for unhealthy levels of alcohol use for both men and women.
There are several limitations to note when interpreting the findings of this study. First, the sample was predominantly White and middle class; thus, generalizability to other populations awaits further study. Second, our measure of stressful events used an aggregated index rather than disaggregated, domain-specific indexes that may have provided greater specificity to the obtained relationships. Third, only 9 of the 18 interactions were significant, and it is unclear why 9 were not significant, although inconsistencies in interaction findings are common in this literature (Kuntsche et al., 2005). In addition, of the nine nonsignificant interaction terms, five were predicting the Wave 7 QFI outcome. As noted earlier, we hypothesized that the interaction terms would be more robust predictors of the problematic alcohol outcomes relative to the QFI outcome. Fourth, although the 5-year interval between waves of assessment expanded the longitudinal scope for the investigation of these relationships, it would also be beneficial to have longitudinal designs with shorter intervals (e.g., daily reporting) to better understand the “coupling” of alcohol use and stress, and the establishment of positive regulatory patterns (Dvorak et al., 2014; Hussong et al., 2005).
Footnotes
This study was supported by National Institute on Alcohol Abuse and Alcoholism Grant Nos. R21AA020047 and K05AA021143 (awarded to Michael Windle). The contents are solely the responsibility of the authors and do not necessarily represent the official views of the National Institutes of Health.
References
- Aiken L. S., West S. G. Multiple regression: Testing and interpreting interactions. Thousand Oaks, CA: Sage; 1991. [Google Scholar]
- Armor D. J., Polich M. J. Measurement of alcohol consumption. In: Pattison E. M., Kaufman E., editors. Encyclopedic handbook of alcoholism. New York, NY: Gardner Press; 1982. pp. 72–80. [Google Scholar]
- Brennan P. L., Schutte K. K., Moos R. H. Reciprocal relations between stressors and drinking behavior: A three-wave panel study of late middle-aged and older women and men. Addiction. 1999;94:737–749. doi: 10.1046/j.1360-0443.1999.94573712.x. [DOI] [PubMed] [Google Scholar]
- Brennan P. L., Schutte K. K., Moos R. H. Pain and use of alcohol to manage pain: Prevalence and 3-year outcomes among older problem and non-problem drinkers. Addiction. 2005;100:777–786. doi: 10.1111/j.1360-0443.2005.01074.x. [DOI] [PubMed] [Google Scholar]
- Choi N. G., DiNitto D. M. Heavy/binge drinking and depressive symptoms in older adults: Gender differences. International Journal of Geriatric Psychiatry. 2011a;26:860–868. doi: 10.1002/gps.2616. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Choi N. G., DiNitto D. M. Psychological distress, binge/heavy drinking, and gender differences among older adults. American Journal on Addictions. 2011b;20:420–428. doi: 10.1111/j.1521-0391.2011.00149.x. [DOI] [PubMed] [Google Scholar]
- Conger J. J. Alcoholism: Theory, problem and challenge. II. Reinforcement theory and the dynamics of alcoholism. Quarterly Journal of Studies on Alcohol. 1956;17:296–305. [PubMed] [Google Scholar]
- Cooper M. L. Motivations for alcohol use among adolescents: Development and validation of a four-factor model. Psychological Assessment. 1994;6:117–128. [Google Scholar]
- Cooper M. L., Frone M. R., Russell M., Mudar P. Drinking to regulate positive and negative emotions: A motivational model of alcohol use. Journal of Personality and Social Psychology. 1995;69:990–1005. doi: 10.1037//0022-3514.69.5.990. [DOI] [PubMed] [Google Scholar]
- Cooper M. L., Frone M. R., Russell M., Peirce R. S. Gender, stress, coping, and alcohol use. In: Wilsnack R. W., Wilsnack S. C., editors. Gender and alcohol: Individual and social perspectives. New Brunswick, NJ: Rutgers Center of Alcohol Studies; 1997. pp. 199–224. [Google Scholar]
- Cooper M. L., Russell M., Skinner J. B., Frone M. R., Mudar P. Stress and alcohol use: Moderating effects of gender, coping, and alcohol expectancies. Journal of Abnormal Psychology. 1992a;101:139–152. doi: 10.1037//0021-843x.101.1.139. [DOI] [PubMed] [Google Scholar]
- Cooper M. L., Russell M., Skinner J. B., Windle M. Development and validation of a three-dimensional measure of drinking motives. Psychological Assessment. 1992b;4:123–132. [Google Scholar]
- Crutzen R., Kuntsche E., Schelleman-Offermans K. Drinking motives and drinking behavior over time: A full cross-lagged panel study among adults. Psychology of Addictive Behaviors. 2013;27:197–201. doi: 10.1037/a0029824. [DOI] [PubMed] [Google Scholar]
- Dvorak R. D., Pearson M. R., Day A. M. Ecological momentary assessment of acute alcohol use disorder symptoms: Associations with mood, motives, and use on planned drinking days. Experimental and Clinical Psychopharmacology. 2014;22:285–297. doi: 10.1037/a0037157. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Glass T. A., Prigerson H., Kasl S. V., Mendes de Leon C. F. The effects of negative life events on alcohol consumption among older men and women. The Journals of Gerontology: Series B, Psychological Sciences and Social Sciences. 1995;50B:S205–S216. doi: 10.1093/geronb/50b.4.s205. [DOI] [PubMed] [Google Scholar]
- Hankin B. L., Abramson L. Y. Development of gender differences in depression: An elaborated cognitive vulnerability-transactional stress theory. Psychological Bulletin. 2001;127:773–796. doi: 10.1037/0033-2909.127.6.773. [DOI] [PubMed] [Google Scholar]
- Holahan C. J., Moos R. H., Holahan C. K., Cronkite R. C., Randall P. K. Drinking to cope, emotional distress and alcohol use and abuse: A ten-year model. Journal of Studies on Alcohol. 2001;62:190–198. doi: 10.15288/jsa.2001.62.190. [DOI] [PubMed] [Google Scholar]
- Holahan C. J., Moos R. H., Holahan C. K., Cronkite R. C., Randall P. K. Drinking to cope and alcohol use and abuse in unipolar depression: A 10-year model. Journal of Abnormal Psychology. 2003;112:159–165. [PubMed] [Google Scholar]
- Holmes T. H., Rahe R. H. The Social Readjustment Rating Scale. Journal of Psychosomatic Research. 1967;11:213–218. doi: 10.1016/0022-3999(67)90010-4. [DOI] [PubMed] [Google Scholar]
- Hussong A. M., Galloway C. A., Feagans L. A. Coping motives as a moderator of daily mood-drinking covariation. Journal of Studies on Alcohol. 2005;66:344–353. doi: 10.15288/jsa.2005.66.344. [DOI] [PubMed] [Google Scholar]
- Khantzian E. J. The self-medication hypothesis of substance use disorders: A reconsideration and recent applications. Harvard Review of Psychiatry. 1997;4:231–244. doi: 10.3109/10673229709030550. [DOI] [PubMed] [Google Scholar]
- Kuipers M. A. G., van Poppel M. N. M., van den Brink W., Wingen M., Kunst A. E. The association between neighborhood disorder, social cohesion and hazardous alcohol use: A national multilevel study. Drug and Alcohol Dependence. 2012;126:27–34. doi: 10.1016/j.drugalcdep.2012.04.008. [DOI] [PubMed] [Google Scholar]
- Kuntsche E., Knibbe R., Gmel G., Engels R. Why do young people drink? A review of drinking motives. Clinical Psychology Review. 2005;25:841–861. doi: 10.1016/j.cpr.2005.06.002. [DOI] [PubMed] [Google Scholar]
- Lachman M. E. Development in midlife. Annual Review of Psychology. 2004;55:305–331. doi: 10.1146/annurev.psych.55.090902.141521. [DOI] [PubMed] [Google Scholar]
- Phares V., Compas B. E. The role of fathers in child and adolescent psychopathology: Make room for daddy. Psychological Bulletin. 1992;111:387–412. doi: 10.1037/0033-2909.111.3.387. [DOI] [PubMed] [Google Scholar]
- Pohorecky L. A. Stress and alcohol interaction: An update of human research. Alcoholism: Clinical and Experimental Research. 1991;15:438–459. doi: 10.1111/j.1530-0277.1991.tb00543.x. [DOI] [PubMed] [Google Scholar]
- Roerecke M., Rehm J. Alcohol intake revisited: Risks and benefits. Current Atherosclerosis Reports. 2012;14:556–562. doi: 10.1007/s11883-012-0277-5. [DOI] [PubMed] [Google Scholar]
- Sayette M. A. Does drinking reduce stress? Alcohol Research & Health. 1999;23:250–255. [PMC free article] [PubMed] [Google Scholar]
- Tigges B. B. Parental consent and adolescent risk behavior research. Journal of Nursing Scholarship. 2003;35:283–289. doi: 10.1111/j.1547-5069.2003.00283.x. [DOI] [PubMed] [Google Scholar]
- Wills T. A., Shiffman S. Coping and substance use: A conceptual framework. In: Shiffman S., Wills T. A., editors. Coping and substance use. Orlando, FL: Academic Press; 1985. pp. 3–24. [Google Scholar]
- Windle M. Parental, sibling, and peer influences on adolescent substance use and alcohol problems. Applied Developmental Science. 2000;4:98–110. [Google Scholar]
- Windle M. A multilevel developmental contextual approach to substance use and addiction. Biosocieties. 2010;5:124–136. doi: 10.1057/biosoc.2009.9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Windle M., Windle R. C. A prospective study of alcohol use among middle-aged adults and marital partner influences on drinking. Journal of Studies on Alcohol and Drugs. 2014;75:546–556. doi: 10.15288/jsad.2014.75.546. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Windle M., Mun E. Y., Windle R. C. Adolescent-to-young adulthood heavy drinking trajectories and their prospective predictors. Journal of Studies on Alcohol. 2005;66:313–322. doi: 10.15288/jsa.2005.66.313. [DOI] [PubMed] [Google Scholar]
- Zuckerman M. Vulnerability to psychopathology: A biosocial model. Washington, DC: American Psychological Association; 1999. [Google Scholar]