

Abstract
Context:
Oral health awareness and oral care are crucial aspects of oncology nursing practice. However very few studies concentrate on the oral care of cancer patients undergoing cancer treatment and nursing practice in the Indian subcontinent. Most of the published studies have been conducted in the Western and European countries.
Aim:
This study aimed to determine the nurses’ knowledge and education about oral care in cancer patient undergoing chemotherapy and radiation therapy.
Setting and design:
A cross sectional descriptive survey was conducted among 158 staff nurses working in oncology related areas from 4 different hospitals of Dakshina Kannada district and Udupi district of Karnataka state, India.
Statistical Analysis:
descriptive and inferential statistics was used by using SPSS 16 version.
Results:
Majority 81 (51.3%) of the staff nurses had poor knowledge of oral care in cancer patients whereas 87 (55.1%) reported that knowledge acquired through basic education in oral care is not sufficient. Most of the staff nurses 115 (72.8%) did not receive basic education in oral care of cancer patients. There was significant association between knowledge and variables such as designation (.005), years of work experience (.040) and years of experience in cancer wards (.000) at 0.05 levels.
Conclusion:
Lack of knowledge suggest the need to develop and implement continuing nursing education programs on oral care specifically for patients receiving cancer treatments, for improving knowledge of staff nurses’ in order to render comprehensive care to the patients. This study also recommends the importance of inclusion of cancer patient specific oral care in the curriculum which can enhance competency of the qualified nurses in cancer wards.
Keywords: Cancer patients, Chemotherapy, Education, Knowledge, Oral care, Radiation therapy, Staff nurses
INTRODUCTION
Worldwide around 500,000 new cases of head and neck cancers are projected annually.[1] Treatment for head and neck cancers primarily involves three modalities: Surgery, radiation, and chemotherapy, administered alone or in combination. Innovative treatments for head and neck cancers, including the use of advanced radiotherapy and chemotherapy, may deliver better regional tumor control rates; however, patients may experience more recurrent and more severe toxicities that result in considerable morbidity and mortality. Radiotherapy for head and neck cancers and chemotherapy for cancers in general are known to cause various deleterious effects on the oral structures leading to development of mucositis, candida infection, xerostomia, loss of taste sensation, radiation caries, and osteochemo/radionecrosis. These oral changes further cause pain and discomfort and difficulty in speaking and swallowing. Oral care is essential before and during cancer treatment to prevent oral complications. Nurses have the crucial role in providing bedside supportive care to patients suffering from cancer. However, to a large extent, nurses lack the necessary knowledge and skill in oral care of cancer patients.[2,3,4]
BACKGROUND
Good oral hygiene maintenance before and during cancer therapy can minimize the complications associated with the treatment and provide greater comfort to patients.[5] Maintenance of oral care of cancer patients requires a combined effort from the attending oncologist, dental surgeon, oncology ward nurse, and the patient's caregiver at home. However, very little is known about the nurses’ knowledge and practices of oral care in patients undergoing treatment for oral cancer.[6]
In a study carried out to determine nurses’ knowledge and education about oral care and oral health assessment of patients’ undergoing cancer treatment, it was seen that oncology ward nurses did not have sufficient knowledge to identify signs and symptoms associated with cancer therapy. Also, they did not have substantial oral care education during their preregistration education. This study suggested that nurses require more education if they have to manage the oral care of patients with cancer effectively.[3]
In the literature, the most frequently suggested intervention for managing oral side effects of chemotherapy and radiation therapy is by providing good oral care employing predetermined oral care protocols, with the assumption that nurses have adequate knowledge and skills to perform oral care appropriately. However, most nurses reported that they provided what would be considered less than optimal care for their patients, particularly the dentate population. It was not clear whether this oversight was a result of a lack of time, knowledge, or personal attitudes of the nursing staff.
In previous studies, the most significant lacunae in the nursing staff's understanding of oral care were evident in their self-reported knowledge and the objective evaluation of knowledge.[3,7]
Over 83% of the nursing staff felt that they had good to excellent knowledge of oral health. However, correct answers were obtained for only 64% of the specific questions asked regarding oral care. The highest correct response rate for individual topics was 87% with respect to denture care. This highlights an important lacuna that must be addressed because a large number of patients are likely to retain their natural dentition.
It is also interesting to note that in a research study based in Mississippi, nursing home staff though had at least a high school diploma and majority with some training beyond this basic level had very little knowledge regarding dental health. We believe that, this can to some extent be attributed to failure in the structure of the training program.
Also, it is imperative that dental professionals should be encouraged to participate in the teaching program of nursing schools and advanced training certification programs for nursing staff.[7]
In this context, we felt the need to study the nurses’ knowledge regarding oral care for patients receiving cancer treatment in the Indian scenario.
MATERIALS AND METHODS
The aim of the study was to assess nurses’ knowledge regarding oral care of cancer patients receiving chemotherapy and radiation therapy.
A descriptive cross-sectional survey was conducted between July 2013 to October 2013 among 158 nurses working in oncology wards from selected four hospitals of Udupi and Dakshina Kannada District in Karnataka State. Registered staff nurses having at least 1 year of experience of caring for cancer patients undergoing cancer treatment and consenting to participate were included in the study. Non-random purposive sampling technique was used for sample selection.
Data collection and analysis
Following the institutional review board approval, the participants were informed about the study and a written informed consent was obtained.
The self-administered anonymous questionnaire was used for the study, which included demographic data, a structured knowledge questionnaire, and education-related information. Information in the demographic data sheet was related to staff nurses’ age, gender, qualification, special education, experience, and experience in oncology areas. Knowledge questionnaire [Figure 1] focused on oral care, oral complications of chemotherapy and radiation therapy, and evidence-based interventions. Knowledge questionnaire consisted of 24 items. Each right answer was awarded 1 mark and was categorized further as good knowledge [score 18 and above (75%)], average knowledge [12 to 15 (50-74%)], poor knowledge [11 and below (less than 50%)]. Another tool regarding education included information regarding basic and continuing education, protocols, or policies related to oral care of cancer patients.
Figure 1.
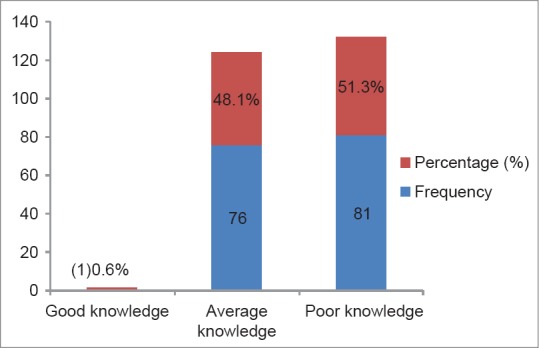
Bar diagram showing the distribution of the knowledge scores n= 158
Data was analyzed using descriptive and inferential statistics [SPSS (Statistical Package for the Social Sciences) 16.0 version]. Content validity of the questionnaire was established by giving the instrument to five experts from different fields such as Nursing, Oncology, and Oral Medicine Departments. Reliability of the knowledge questionnaire was established by split half method and the tool was found to be reliable (0.73).
RESULTS
Of the 200 nurses approached, a total of 158 staff nurses, 8 male, and 150 female participated in this study, producing a return rate of 79%.
Socio-demographic information about participants
Most of the staff nurses 86 (54.4%) were in the age-group of 18–25 years. Majority 150 (94.9%) were females. Majority 94 (59.5%) of the staff nurses had General Nursing Midwifery as their qualification, whereas only 16 (10.12%) were nurses with a graduate degree. Among them, 14 were nurses with BSc (bachelors in science degree) and 2 were nurses with Post Basic bachelors in science degree (PCBSc). There were 3 Auxillary Nurse Midwives (ANMs). Only 2 (0.12%) of the staff nurses had a diploma in cancer nursing. Most, 134 (78.5%) of the participants were staff nurses while 20 (12.7%) were working as ward incharge. A majority, 98 (62%) of the staff nurses had experience of 1–5 years. Among them, 119 (75.3%) had 1–5 years’ experience in caring for cancer patients.
Majority 74 (46.83%) of the staff nurses were working in medical oncology wards, whereas 34 (21.51%) were form radiation oncology, 22 (13.92%) from oncology outpatient department, 21 (13.39%) from special/private wards, and 7 (4.43%) were from day-care units [Figure 2].
Figure 2.
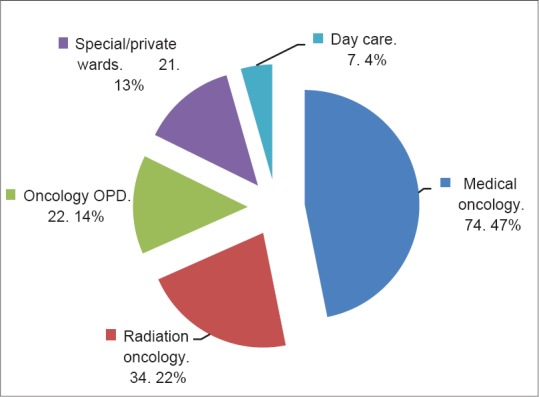
Pie chart showing distribution of work area of the participants area of work n=158
Nurses knowledge of oral care in cancer patients
The present study showed that the majority 81 (51.3%) of the staff nurses had poor knowledge of oral care in cancer patients [Figure 1].
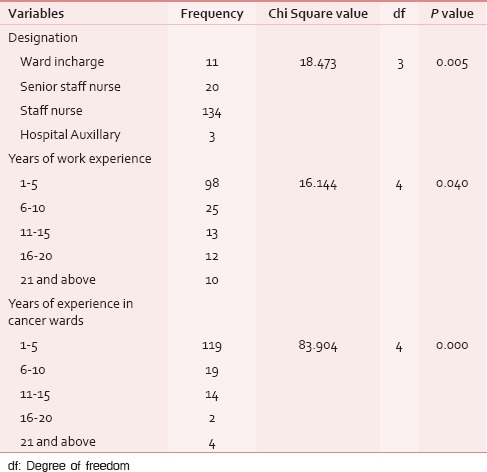
The present study showed association between knowledge and selected demographic variables such as designation, years of work experience, and years of experience in cancer wards at 0.05 levels, whereas there was no association found between knowledge and selected demographic variables such as age, gender, qualification, special education, and area of work [Table 1].
Table 1.
Association between knowledge and selected demographic variables n=158
Basic and continuing education on oral care of cancer patients
Only 43 (27.2%) of the staff nurses reported to have received basic education in oral care of cancer patients. Thirty-one (19.62%) of the staff nurse reported that knowledge acquired through basic education in oral care is sufficient. Majority 128 (81%) of the respondents said to have acquired enough knowledge of oral care in general, but not for patients on cytotoxic drugs or radiation therapy. Most 114 (72.2%) of the respondents said that they received only theoretical training, whereas only 42 (26.6%) expressed that they had received both theoretical and clinical training.
Around 33 (20.9%) of the respondents expressed that they had attended regular continuing education in oral care, whereas majority 128 (81%) of them expressed that there is a need for continuing education in oral care.
Nursing curriculum evaluation
Curriculum of Auxillary Nursing Midwifery (ANM), General Nursing midwifery (GNM), BSc Nursing, and MSc Nursing (oncology nursing) were reviewed by the researcher. All the courses did contain a topic on basic oral care in theory and practical log books, but they were specifically related to general oral care of patients. The curriculum did not contain anything specific related to oral care in cancer patients receiving cancer treatments. The curriculum of MSc Nursing (oncology nursing) had detailed areas of cancer treatments, its side effects, complications, and management but did not had a definite aspect of oral care plan especially for patients with potential side effects of cancer treatments in theory and practical experiences.
This clearly indicates that the majority of nurses who are working with the cancer patients did not receive any specific training in oral care of cancer patients. Oral care is performed in the cancer wards either by routine practice or by instruction of the physician.
DISCUSSION
The present study showed that majority of the staff nurses 81 (51.3%) had poor knowledge of oral care in cancer patients. Certain studies have also reported that qualified nurses lack adequate knowledge related to oral health, resulting in inadequate oral care of patients.[2]
In a similar study conducted among nurses to determine their knowledge and education revealed that general nurses demonstrated less knowledge in oral care and examination of the oral cavity compared to nurses working in cancer wards.[3] The self-rated knowledge was poorest on fluorides and oral signs and symptoms and highest on tooth brushing and cleaning dentures.[6]
Among the respondents, 67 (79.1%) stated that they had not attended regular continuing education in oral care, whereas most of them, 128 (81%) expressed that there is a need for continuing education in oral care. Another similar study shows that most nurses seemed to agree that they need to have updates in oral care (85.3%). Half of the respondents (50%) stated that updates should take place every 6 months to a year. Staff should also be encouraged to keep up-to-date with current research findings.[2] In a study conducted among oncology nurses to determine their knowledge and education, 94% of the participants stated a need for continuous education.[3] Only 13% had attended a regular continuing education course in oral care, and 32% had not received any continuing education.[6]
In our study, only 43 (27.2%) of the staff nurses reported to have received basic education in oral care of cancer patients. Sixty-nine (80.38%) of the staff nurse reported that knowledge acquired through basic education in oral care is sufficient. Majority, 128 (81%) of the respondents said to have acquired enough knowledge of oral care in general, but not for patients on cytotoxic drugs or radiation therapy. In a similar study carried out to determine nurses’ knowledge and education reported that 56.9% of the participants had not received any education in oral care of patient with cytotoxic drug and radiation treatment. Only 45.8% had received basic education in oral care of cancer patients.[3] None of the nurses and four of the enrolled nurses reported that they had received substantial education in oral care during their basic training.[6]
Most, 114 (72.2%) of the respondents said that they received only theoretical training, whereas only 42 (26.6%) expressed that they have received both theoretical and clinical training. In a similar study conducted among nurses to determine their knowledge and education stated that around 45.8% of the participants received both theoretical and clinical education, whereas 43.1% had received no education at all and 9.7% had received a lot of education in oral care.[3] Fifty-six percent had received theoretical raining only, 8% clinical training, and 36% both theoretical and clinical training.[6]
In the present study, curriculum evaluation revealed some of the drawbacks in the current syllabus such as lack of emphasis on educational material on oral care of cancer patients. The practical training of the existing nurses was also inadequate due to insufficient number of training programs. Data from another study conducted among 172 directors of education revealed that 27% (32) were post-registration Nurse Training Establishments (NTEs) do not teach oral care in their training. Seventy-nine percent (67) of these had no dental input. Twenty-eight percent (24) taught the use of an oral care assessment form, 38% (32) discussed dental plaque. Thirty-eight percent (32) had no exclusive lectures on oral care. Of 31 textbooks, only 1 had comprehensive coverage of the subject. This study reported the deficiencies in the syllabus regarding oral care.[8] Variations in participants’ knowledge may indicate variations in educational provision across different countries.[9]
Since the present study reported that nurses lack specific training on oral care of cancer patients, it would be appropriate to develop a training module for oral care in cancer patients undergoing treatment. Continuing nursing education units in hospitals should train all nurses working in cancer wards regarding oral care and ensure effective implementation of oral care practices with frequent documentation audits and patient outcomes with respect to oral problems. Nurses need to keep abreast of the latest knowledge in oral care of cancer patients, assessment of oral cavity, oral care agents, and evidence-based interventions in care of cancer patients undergoing chemotherapy and radiation therapy.
This study emphasizes the need for developing more suitable material for systematic assessment of the oral cavity and analysis of existing oral care protocols. There is an immediate need for development of a specific protocol including evidence based interventions and recommendation from the regulatory bodies for oral care applicable to patients undergoing head and neck radiation and chemotherapy. Existing practices should be thoroughly assessed for effectiveness to develop uniform standards of oral care. Patient education material should be made an essential component of oral care regimen.
Development and implementation of more specific oral care protocol can lead to promotion of oral health by health care professionals, ensuring that oral care is performed regularly across the hospital, minimizing the severity and duration of radiation-induced, and standard dose chemotherapy-induced oral mucositis and its complications, ensuring that patients’ treatment is not compromised because of oral problems as well as there is no extension of length of hospital stay.
Focused interventions that integrate the basic ideologies of oral care with existing knowledge about the progressive aspects of clinical manifestations, evidence-based standardized approaches to assessment, and utilization of innovative treatment regimens provide an important means by which there will be improvement in patient outcomes. Oral care protocols are essential components of cancer management strategies against treatment related morbidities. Current knowledge of pathophysiology with a targeted, standardized method may help to reduce overall morbidity and improve quality of life in cancer patients.
Study limitations
The results of this study cannot be generalized to the broader population because a purposive non-random sampling technique was used and data was collected from cancer wards of four hospitals, and a self-report technique of data collection was used.
CONCLUSION
In the present study, most of the staff nurses had poor to average knowledge regarding oral care in cancer patients. Many of them even expressed the need to have frequent continuing nursing education specific to cancer patient care, and this requires involvement from a multidisciplinary team involving dentists, radiation oncologists, and medical oncologists on how to perform oral cavity examination and recognize the signs and symptoms of oral changes associated with cancer therapy.
Therefore, it seems suitable to recommend that nurses require more education in oral care and on the effects of chemo therapy and/or radiation therapy on the oral cavity. Nursing curriculum definitely needs to be revised based on the present needs, as different levels of nursing curriculum even at masters’ program do not emphasize the requirement of oral health awareness and assessments to be carried out in cancer units. This study recommends formulation of a more structured curriculum emphasizing on the preventive and post-treatment oral care in cancer nursing.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Haddad RI, Shin DM. Recent advances in head and neck cancer. N Engl J Med. 2008;359:1143–54. doi: 10.1056/NEJMra0707975. [DOI] [PubMed] [Google Scholar]
- 2.Adams R. Qualified nurses lack adequate knowledge related to oral health, resulting in inadequate oral care of patients on medical wards. J Adv Nurs. 1996;24:552–60. doi: 10.1046/j.1365-2648.1996.22416.x. [DOI] [PubMed] [Google Scholar]
- 3.Southern H. Oral care in cancer nursing: Nurses’ knowledge and education. J Adv Nurs. 2006;57:631–8. doi: 10.1111/j.1365-2648.2006.04159.x. [DOI] [PubMed] [Google Scholar]
- 4.Carter LM, Harris AT, Kavi VP, Johnson S, Kanatas A. Oral cancer awareness amongst hospital nursing staff: A pilot study. BMC Oral Health. 2009;9:4. doi: 10.1186/1472-6831-9-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Holmes S. The oral complications of specific anti-cancer therapy. Int J Nurs Stud. 1991;28:343–60. doi: 10.1016/0020-7489(91)90061-7. [DOI] [PubMed] [Google Scholar]
- 6.Ohrn KE, Wahlin YB, Sjödén PO. Oral care in cancer nursing. Eur J Cancer Care. 2000;9:22–9. doi: 10.1046/j.1365-2354.2000.00185.x. [DOI] [PubMed] [Google Scholar]
- 7.Robin MH. Survey of oral hygiene knowledge and practice among mississippi nursing home staff. The University of Mississippi Medical Center, USA. 2010 [Google Scholar]
- 8.Longhurst RH. Cross-sectional study of the oral healthcare instruction given to nurses during their basic training. Br Dent J. 1998;184:453–7. doi: 10.1038/sj.bdj.4809656. [DOI] [PubMed] [Google Scholar]
- 9.Hijji B. Trained nurses’ knowledge and practice of oral care in three wards in acute care hospital in Abu Dhabi. Braz J Nurs. [Last accessed on 2013 Jul 20]. Online. Available from: http://www.nepae.uff.br//siteantigo/objn203hijji.htm .