

Summary
Burn injury remains a serious and devastating issue faced by developing countries. It is also true, however, that the developed world still tackles many of the challenges caused by burns. In order to reduce this problem through preventive programs, the characteristics of this type of injury must be studied and well documented in each setting. Our study aims to show the epidemiology, demographic distribution and clinical outcomes of burns patients referred to Motahari Burn Hospital, the burn care center that receives the most referrals in Iran. This cross-sectional study, from March 2009 to March 2010, included 6,910 patients with burn injuries who were managed as outpatients. The patient demographics along with the characteristics of the burn injuries and their outcomes were recorded for each case and then evaluated. A total of 6,910 burn patients with a mean ± SD age of 30.20 ± 19.11 years presented to our Emergency Department and were treated as outpatients. Of these, 2,900 were female (41.97%) and 4,010 were male (58.03%). Most of the patients were in the 25-35 year age group, with a prevalence of 1,148 (28.6% of total) males and 716 females (24.7% of total), followed by those aged <15-years-old. Most patients had been burned accidentally. An increase in the instance of self-immolation was identified with an increase in the TBSA burned. Mean follow-up was 30+/-5 months. The results revealed that burns were most likely to occur during housekeeping. Other high risk groups identified were males, those aged from 25 to 35 years-old, and those with lower socio-economic status.
Keywords: epidemiology, outpatient, burn, Tehran, Iran
Abstract
Dans les pays en développement les brûlures sont un problème grave. Il est également vrai que le monde développé aborde encore de nombreux défis causés par des brûlures. Afin de réduire ce problème en développant un programme de prévention, les caractéristiques de ce type de blessure devraient être étudiées et bien documentées dans chaque paramètre. Notre étude vise à montrer l’épidémiologie, répartition démographique et les résultats cliniques de patients brûlés traitées à l’hôpital Motahari en Iran. L’étude transversale de Mars 2009 à Mars 2010 comprend 6.910 patients atteints de brûlures qui ont été gérées en ambulatoire. La démographie ainsi que les caractéristiques des brûlures et leurs résultats ont été enregistrés pour chaque cas, puis évalués. Un total de 6.910 patients brûlés avec un moyen âge de 30,20±19,11 années sont présentés à notre service d’urgence et ont été traités en ambulatoire. Parmi ceux-ci, 2.900 étaient de sexe féminin (41,97%) et 4.010 de sexe masculin (58,03%). La plupart des patients étaient dans le groupe âgé de 25-35 ans, dont 1.148 (28,6% du total) étaient des hommes et 716 (24,7% du total) des femmes, suivis par les patients avec moins de 15 ans. La plupart des patients avaient été brûlés accidentellement. Une augmentation de l’occurrence de l’auto-immolation a été identifié avec une augmentation de la surface corporelle totale brûlée. La période moyenne de suivi était de 30+/-5 mois. Les résultats ont révélé que les brûlures étaient les plus susceptibles de se produire lors de l’entretien ménager. D’autres groupes à haut risque identifiés sont: les hommes, les jeunes âgés de 25-34 ans et ceux ayant le statut socio-économique plus faible.
Introduction
Burn injury afflicts people from across the world and is thus not confined to a single country or to a particular population.1-2 In the US, among roughly 2 million burn patients treated at burn centers each year, about one third are hospitalized while the remainder receive outpatient care.3 Even though many cases do not require intensive care and can be discharged early, there is a high probability of post incidental physical and psychological complications.3-7 This indicates that even in cases of minor burn injuries, requiring only outpatient management, there can be a significant impact on health care budgets, resulting in a heavy burden particularly for societies with lower incomes per capita.5-12 Previous reports from Iran have identified women aged 21 to 30 years old and children aged <10 years old to be at greatest risk of burn injury.12 Scalds have also been documented to be the most common cause of burns requiring outpatient treatment.
As a first step to dealing with these issues, it is fundamental to understand the details of the occurrence of burn injuries, particularly in those countries where preventive strategies are to be implemented. These details change from one country to another, as well as from culture to culture, with new characteristics replacing those already described. For this reason, despite many studies having been undertaken worldwide, including several in Iran,4-13 the foundation on which to build preventive action requires periodic, if not daily updates.
The aim of this cross-sectional study was to describe the epidemiologic and etiologic patterns of burn injuries among outpatient clinics in the capital of our country in order to provide a basis for future preventive action.
Methods and materials
Between March 2009 and March 2010, patients who presented to the Emergency Department (ED) of Motahari Burn Hospital were enrolled in our cross- sectional study. Motahari Burn Hospital is well known as a referral center for tertiary burn care, receiving a wide range of burn cases from across the country. All of the patients with burn injuries were eligible for our study. The data were obtained by direct interview allowing the physicians to record demographics and other patient characteristics daily by compiling a questionnaire. If the patients were hospitalized, daily assessments and managements were also recorded by nurses trained in-house. Outpatient cases had a specific recording file which was completed by the doctor in charge during each visit. The data of hospitalized (in-patient) patients were included in another study. Patients were assured that all information provided would be strictly confidential and gave signed consent to participate in the study. The protocol of the study was approved by the Research and Ethics Review Boards of Iran University of Medical Sciences, Tehran, Iran.
The data were analyzed using Statistical Package for the Social Sciences (SPSS) version 16. Values are presented mostly as a percentage (%) or mean ± SD. If applicable, p value was measured to assess the statistical significance of the differences, with a value of p<0.05 being considered statistically significant.
Results
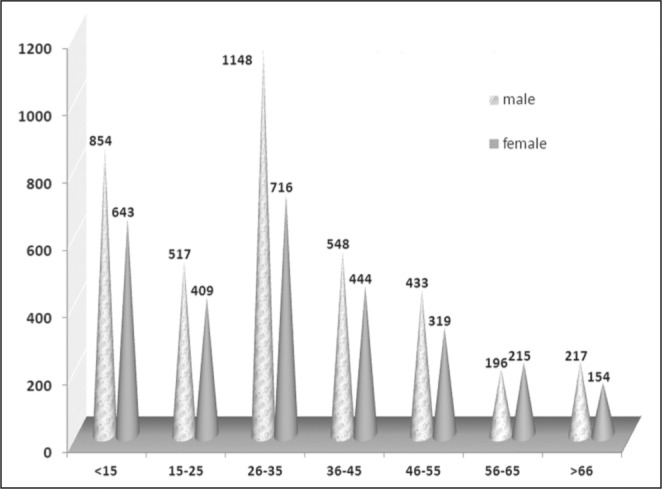
Over the one year study period, a total of 6,910 burn patients with a mean ± SD age of 30.20±19.11 years presented to our ED and were treated as outpatients, of whom 2,900 were female (41.97%) and 4,010 male (58.03%). The most prevalent patients were in the 25-35 year age group: 1,148 (28.6% of total) of whom were male and 716 of whom were female (24.7% of total); followed by those aged <15 years old: 854 of whom were male (21.3% of total ) and 643 of whom were female (22.2% of total) (Fig. 1). Mean follow up was 30+/_5 months.
Fig. 1. Patient age group and gender.
As our study shows, most patients (3,086; 44.65%) had an intermediate level of education followed by 1,860 (26.91%) with a preliminary educational level (Fig. 2). In terms of marital status, 3,884 (56.16%) patients were married, most of whom (97.6%) belonged to the 46-55 yearold age group. Of the 6,910 outpatient burn victims, 4,157 (60.15%) were covered by insurance, 307 of which were in the 56-65 year-old age group (Fig. 3). In addition, a total of 5,212 (75.42%) patients were enrolled in outdoor occupation, among whom the 56-65 year-old age group had the highest frequency (99.7%) (Fig. 4).
Fig. 2. Patient age group and education.
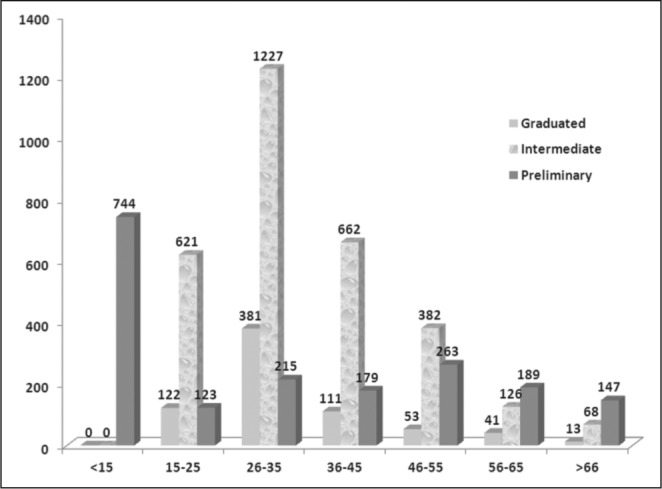
Fig. 3. Patient insurance coverage (percentage).
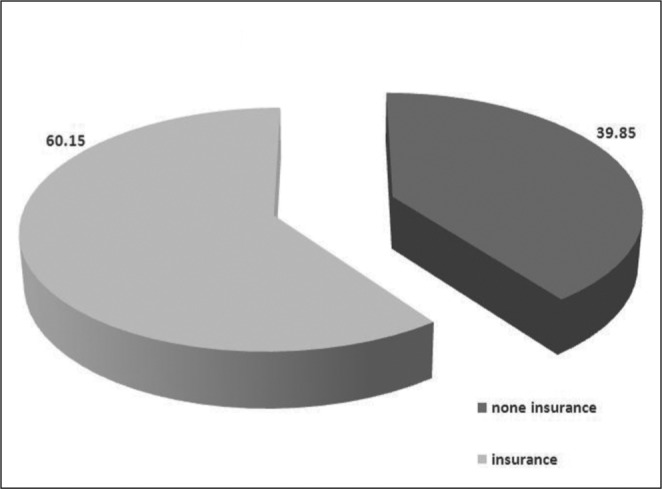
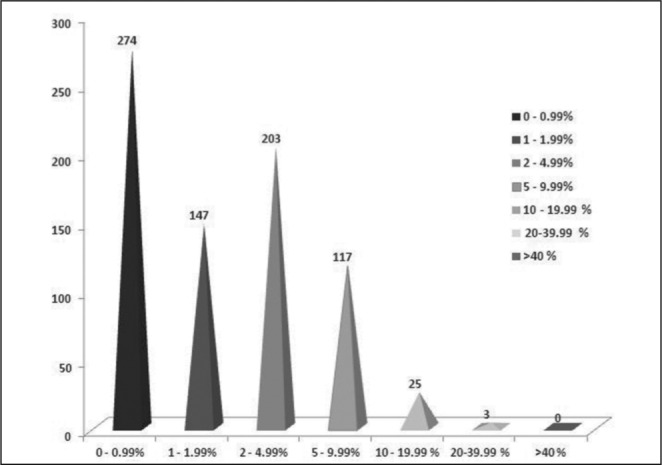
Fig. 4. Frequency of job related causes by percentage of burn injuries (TBSA).
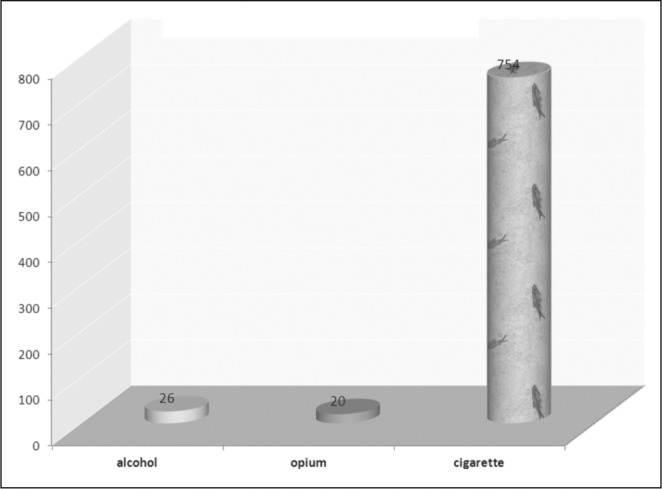
Regarding patient medical background, 219 (3.2%) were identified as having diabetes mellitus (DM) followed by 97 (1.4%) with cardiovascular disease and 165 patients (2.4%) with hypertension (HTN). Of these, the mean ± SD of TBSA involvement was greatest (3.08±3.09) among those with a history of HTN. However, 6 patients with DM had inhalation injury, giving them the highest frequency (2.7%). Of 183 patients (2.6%) with a previous history of burn injury, their 2nd degree burns involved the most TBSA with a mean ± SD of 3.66±4.88. Most patients with a previous history of burns presented with 2nd degree burns in our study. Among patients with addictions, 754 (10.9%) smoked cigarettes, 20 (0.3%) used opium, and 26 (0.4%) were dependent on alcohol (Fig. 5). There was no direct relation between smoking and alcohol consumption with regards to burn injury. Among this group, those addicted to alcohol had the largest TBSA involvement with a mean ± SD of 7±6.59%. However, patients with a history of cigarette smoking suffered more severe burn injuries, with a mean ± SD of 3rd degree burns of 4.42±1.61cm2 and a frequency of 36 (4.8%) cases involving inhalation injury.
Fig. 5. Clinical characteristics of patients.
Although we had 2nd and 3rd degree burns among our outpatients, it was evident that 2nd degree burns constituted the most prevalent type of outpatient burn injuries (Fig. 6).
Fig. 6. Percentage of burn (TBSA) by degree of burn.
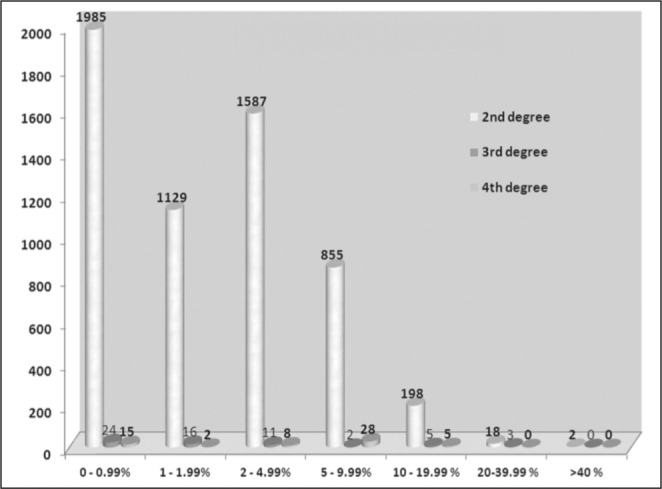
Table I provides a detailed overview of the relationship between outpatient burn features and TBSA. This table shows that as the degree of burn increases, the mean TBSA decreases. For instance, regarding TBSA >40%, all (100%) were second degree burns. The time of injury is shown to be most frequently between 06:00 and 12:00noon among all TBSA categories. Among the burns from flammable substances, oil and tar were the most frequent causes and resulted in the lowest TBSA involvement. Smoke inhalation injury is shown to decrease in frequency as the TBSA increases, occurring more often (0.4%) where TBSA involvement is between 0% and 0.99% and less where TBSA involvement is more than 40%. Among patients with less than 1% TBSA involvement, 852 cases occurred in relation to hot liquids with a prevalence of 4.8%. In 2 cases (9.1%) TBSA involvement of 20-40% was caused by cloth ignition, representing the highest prevalence. Acid was the most frequent chemical substance in each TBSA category, having less involvement as the TBSA increased. Regarding electrical burns, low voltage injuries were more prevalent than high voltage burns and tended to have less TBSA involvement.
Table I. Features of burn injury in relation to TBSA.

Mean ± SD time of transfer to hospital was 19.31±28.90. The greatest delay in transfer time occurred in those with TBSA involvement of less than 1%, decreasing to a mean of 4.20 minutes in patients with TBSA involvement of more than 40%. This indicates that patient transfer time was generally speedy, with patients arriving at the hospital in good time. Most of the burn patients were transferred to hospital by private car.
The majority of burns were accidental, with those inflicted intentionally and by self-immolation following second and third respectively. The cases of self-immolation were seen to rise in line with increasing TBSA involvement, while a decrease in accidental burns was noted as the TBSA involvement increased.
Discussion
Our study aimed to assess the recent epidemiological pattern of burn injuries in the capital of Iran so that the results could be employed to identify groups at risk of such injury. In line with previous studies from Iran4-13 and those from other regions of the world,1-2,14-15 our study revealed that burn injury occurs more frequently in men than women. However, in contrast to those reports, the difference between the percentages of these two sex groups is not remarkable, as shown in Fig. 1, with just a 4% difference. However, there is a factor that should be taken into account here regarding whether the burn injury was intentional or accidental. In this instance, the male to female ratio is subject to change, with many studies reporting a higher prevalence of female burns where self-immolation is involved.4,16
In our study, as in others, those aged 25 to 34 years old are the most frequently impacted age group. Taghavi et al.12 reported a mean age of 31 years for their population while similar studies from Iran5-6,17 measured a lower mean age. The average age-range of our study may be expected, given that this age group is more likely to be active and involved in dangerous activities. However, there is inconsistency across the literature regarding the mean values of age, even from within the same country, which may be explained by differences in sampling or patient selection within each setting.
Although burn injury is not limited to economically developing nations, socio-demographic features of the victims indicate a trend toward a lower economic status, as well as highlighting a considerable correlation between lower socio-economic characteristics and burn severity.18 This was evident in our study, as most patients had an educational level of high school diploma and either ran a private business or were involved in housekeeping. Other studies have also shown housewives to be at greatest risk of burn injuries.12 There are several possible explanations for this, including greater involvement of this group in activities such as cooking at home, especially with traditional and not necessarily standard methods, in which burn injury is more likely to occur. Our study identified a higher incidence of burn injuries with lesser severity among individuals occupied at private businesses compared to the more severe burns in hospitalized patients. This is also due to the sampling of our study which focused solely on those treated as outpatients.
Our results showed that most of the burn incidents occurred between 06:00am and 12:00noon, considering that home-makers are probably alone during this time as other family members are out at work, and likely to be cooking, burns have a greater probability of occuring during this time. Moreover, even when excluding home-makers, 06:00am to 12noon represents a critical period of rush hours to and from work and the time during which most people in Iran are involved in their work duties. This time interval is especially notable in our patients who were injured at work.
Most of the cases of burn injuries admitted to the ED during the study period occurred in closed spaces. This could be due to a lack of smoke detectors in the work place and insufficient residential safety devices, which is generally the case in developing countries such as the region of our study. In our study, burn casualties in closed spaces decreased as the size of the TBSA involvement decreased, similar to the pattern identified in burns involving smoke inhalation injuries.
Scalds from hot liquids were the most frequent cause of burns in our study. The same was also reported from an area similar to Tehran by Taghavi et al.,12 as well as from Shiraz, by Ansari et al.,6 and by others.19 In these studies, scald injuries made up the most common causes of burns in outpatients of all age groups. However, it has also been suggested that flame burns could be the most prevalent cause of burns requiring outpatient treatment.6 It is interesting if we consider the pattern of changes observed in relation to age. Tarim et al.20 reported that children under the age of 6 years old are more likely to be burned by flame contact, while teenagers are more likely to be burned by an electrical current. In another study by Hanand Colleagues,1 scald injuries were the most common causes of burns in the first years of life, after which the common cause changed to flame. In a recent report from Iran by Karimi and Motevalian,21 scalds from hot liquids are the most common cause of burns in children below the age of 10 years old, and flame in those over 10 years old.
Second degree burns have been widely reported to be one of the most commonly seen burn injuries. This has been confirmed both by studies which have included cases in outpatient clinics12 and by others which evaluated the epidemiology of all burn cases.1,99,15,17,21 By implementing the current results, we may be able to develop preventive strategies to lower the probability and fatality of burn cases, even among those who could be successfully managed as outpatients.
Younger women have been identified as one of the most vulnerable populations for burn injuries.8,12-13,22 This may include many women who are burned during pregnancy which, although very rare in our study, can result in problematic consequences. For cultural reasons, pregnant women in Iran tend to settle into safer environments with less exposure to risks.
The timeframe of transfer to hospital has been variably reported by different studies: Ganesamoni et al.22 reported a mean of 3.5 to 4.3 hours delay in hospital transfer in discharged and deceased patients respectively. However, compared to previous reports, there has been a reduction in transfer time in India. In our study, the transfer delay was longest in patients with minimal TBSA involvement, reaching its minimum in those with the greatest TBSA burned. This difference in transfer times could be due to the fact that more severe injuries make patients seek medical care more quickly than milder burn injuries. In comparison to the report from India, our lowest transfer time was consistent with their mean transfer time. This may be due to the fact that Iran has a limited number of tertiary burn care centers, causing many patients from diverse regions to come our center, which receives the most referrals of the entire country. The travel distance required in many instances would thus lead to the larger delay in transfer time to hospital.
As well as the devastating nature of burn injury, its associated cost is another issue which imposes a heavy burden on the health system. This concern is even greater for patients who do not have health insurance and must cover these costs themselves. In our study, 40% of patients had no health insurance coverage, which means not only psychological stress for the patients but also a financial burden for the hospital, health care system and the patients’ families. To date, no study has commented on the impact of health insurance on outcomes of burn patients or its association with the worsening of the burn related burden on societies. Further studies are required to investigate the financial and psychological outcomes of outpatient burn injuries, possibly in comparison with an inpatient setting.
Conclusion
Our study showed that being male, doing housekeeping, being aged between 25-34 years old, and having a lower socio-economic status are the greatest risk factors of encountering burn injury in our population. In addition, most of the injuries occurred at home and between 06:00 and 12noon. Most of the burn patients were transferred to the hospital within less than 30 minutes, and mostly by private car.
Acknowledgments
Conflict of interest. None.
Funding. This study was conducted with the aid of a grant from the vice-president’s office of Iran University of Medical Sciences Research.
Acknowlegments. The Authors wish to thank Mrs. M. Ghadarjani (Head Nurse), Mrs. R. Amiri (nurse), Mrs. A. Kermanshahi, Mrs. Z Karami (nurse), and Mr. G. H. Taban (nurse) for their invaluable efforts in conducting this study.
Statement of authors’ contribution. Each author was actively involved in the planning and carrying out of the study, as well as in the preparation and submission of the present article.
References
- 1.Han TH, Kim JH, Yang MS, et al. A retrospective analysis of 19,157 burns patients: 18-year experience from Hallym Burn Center in Seoul, Korea. Burns. 2005;31:465–70. doi: 10.1016/j.burns.2004.11.014. [DOI] [PubMed] [Google Scholar]
- 2.Ngim RCK. Epidemiology of burns in Singapore children-an 11-year study of 2288 patients. Ann Acad Med Singapore. 1992;21:667–71. [PubMed] [Google Scholar]
- 3.Miller SF, Bessey P, Lentz CW, et al. ABA NBR Committee National burn repository 2007 report: A synopsis of the 2007 call for data. J Burn Care Res. 2008;29:862–70. doi: 10.1097/BCR.0b013e31818cb046. [DOI] [PubMed] [Google Scholar]
- 4.Ahmadi A, Mohammadi R, Stavrinos D, et al. Self-immolation in Iran. J Burn Care Res. 2008;29:451–60. doi: 10.1097/BCR.0b013e31817112f1. [DOI] [PubMed] [Google Scholar]
- 5.Ansari-Lari M, Ansari-Lari M.A. Epidemiology of burns presenting to an emergency department in Shiraz, South Iran. Burns. 2003;29:579–81. doi: 10.1016/s0305-4179(03)00066-4. [DOI] [PubMed] [Google Scholar]
- 6.Groohi B, Alaghehbandan R, Lari AR. Analysis of 1089 burn patients in province of Kurdistan, Iran. Burns. 2002;28:69–74. doi: 10.1016/s0305-4179(02)00099-2. [DOI] [PubMed] [Google Scholar]
- 7.Hosseini R, Askarian M, Assadian O. Epidemiology of hospitalized female burns patients in a burn centre in Shiraz. East Mediterr Health J. 2007:113–8. [PubMed] [Google Scholar]
- 8.Panjeshahin MR, Lari AR, Talei A, Shamsnia J, Alaghehbandan R. Epidemiology and mortality of burns in the South West of Iran. Burns. 2001:219–26. doi: 10.1016/s0305-4179(00)00106-6. [DOI] [PubMed] [Google Scholar]
- 9.Rajabian MH, Aghaei S, Fouladi V. Analysis of survival and hospitalization time for 2057 burn patients in Shiraz, south-western Iran. Med Sci Monit. 2007:353–5. [PubMed] [Google Scholar]
- 10.Saadat M. Epidemiology and mortality of hospitalized burn patients in Kohkiluye va Boyerahmad province (Iran): 2002-2004. Burns. 2005:306–9. doi: 10.1016/j.burns.2004.10.012. [DOI] [PubMed] [Google Scholar]
- 11.Soltani K, Zand R, Mirghasemi A. Epidemiology and mortality of burns in Tehran, Iran. Burns. 1998;24:325–8. doi: 10.1016/s0305-4179(98)00017-5. [DOI] [PubMed] [Google Scholar]
- 12.Taghavi M, Rasouli M.R, Boddouhi N, et al. Epidemiology of outpatient burns in Tehran: An analysis of 4813 cases. Burns. 2010;36:109–13. doi: 10.1016/j.burns.2009.02.011. [DOI] [PubMed] [Google Scholar]
- 13.Lari AR, Alaghehbandan R, Panjeshahin M.R, et al. Suicidal behavior by burns in the province of Fars, Iran. Crisis. 2009;30:98–101. doi: 10.1027/0227-5910.30.2.98. [DOI] [PubMed] [Google Scholar]
- 14.Haik J, Liran A, Tessone A, et al. Burns in Israel: Demographic, etiologic and clinical trends 1997–2003. Isr Med Assoc J. 2007;9:659–62. [PubMed] [Google Scholar]
- 15.Ho WS, Ying SY. An epidemiological study of 1063 hospitalized burn patients in a tertiary burns centre in Hong Kong. Burns. 2001;27:119–23. doi: 10.1016/s0305-4179(00)00095-4. [DOI] [PubMed] [Google Scholar]
- 16.Lari A R, Alaghehbandan R. Epidemiological study of self-inflicted burns in Tehran, Iran. J Burn Care Rehabil. 2003;24:15–20. doi: 10.1097/00004630-200301000-00005. [DOI] [PubMed] [Google Scholar]
- 17.Maghsoudi H, Pourzand A, Azarmir G. Etiology and outcome of burns in Tabriz Iran. An analysis of 2963 cases. Scand J Surg. 2005;94:77–81. doi: 10.1177/145749690509400118. [DOI] [PubMed] [Google Scholar]
- 18.Roberts I. Cause specific social class mortality differentials for child injury and poisoning in England and Wales. J Epidemiol Community Health. 1997;51:334–5. doi: 10.1136/jech.51.3.334. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Houshyarikhah H, Shayestehfard M, Javaherizadeh H, et al. Pediatric burns in Khuzestan Province, Iran. J Egypt Public Health Assoc. 2012;87:34–7. doi: 10.1097/01.EPX.0000408546.10870.8f. [DOI] [PubMed] [Google Scholar]
- 20.Tarim A, Nursal T, Yildirim S, et al. Epidemiology of pediatric burn injuries in southern Turkey. J Burn Care Rehabil. 2005;26:327–30. doi: 10.1097/01.bcr.0000169899.53528.24. [DOI] [PubMed] [Google Scholar]
- 21.Karimi H, Motevalian A, Motabar AR, et al. Epidemiology of paediatric burns in Iran. Ann Burns Fire Disasters. 2012;25:115–20. [PMC free article] [PubMed] [Google Scholar]
- 22.Palumbo L, Budin W. A descriptive summary of New Jersey’s 1985 burn population. J Burn Care Rehabil. 1990;11:565–72. doi: 10.1097/00004630-199011000-00016. [DOI] [PubMed] [Google Scholar]
- 23.Ganesamoni S, Kate V, Sadasivan J. Epidemiology of hospitalized burn patients in a tertiary care hospital in South India. Burns. 2010;36:422–9. doi: 10.1016/j.burns.2009.06.212. [DOI] [PubMed] [Google Scholar]