

Abstract
Background
Infertility is one of the most significant medical, as well as social problems that affect psychological health of families and societies. Determining the prevalence of infertility is important for evaluating the potential of fertility. There are different reports on the prevalence of infertility in Iran, but the current research employs fertility history in order to provide an unbiased estimation of primary infertility.
Methods
Data from a national survey of Iranian women aged 20-40 years was used in this study in year 2011. Totally, 1011 clusters were randomly selected according to post office codes, proportional to the population of the province. We evaluated the history of fertility as the basis for gathering information. Accordingly, we designed a questionnaire. Subsequently, we recruited and trained nurses and obstetricians to call on married women to fill the questionnaires. Primary infertility refers to a condition in which couples have not been able to conceive a child after one year of un-protected intercourse.
Results
In this research, we questioned 17187 women in 1011 clusters. The mean age of the women at the time of their marriage was 20.1, and that of their husbands was 25.4 years. The mean age of women at the time of their first pregnancy was 21.1. This research revealed the prevalence of primary infertility to be 20.2% in Iran.
Conclusion
The prevalence of primary infertility in Iran seems to be higher than the world average. Therefore, it is crucially important to support the large number of couples who face this problem.
Keywords: Prevalence rate, Epidemiology, Primary infertility, Iran
Introduction
Infertility is one of the most important issues related to health that can be estimated via its rate. Calculating the prevalence of infertility is important for evaluating the potential of fertility in any given society (1). Nowadays, Assisted Reproductive Technologies are increasingly being used in different countries. The number of infertility treatment centers and the experts in this field is increasing accordingly; therefore, it is necessary to estimate accurately the prevalence of infertility.
Infertility is the inability to conceive a child. A couple may be considered infertile if, after one year of regular sexual intercourse without contraception, the woman has not become pregnant. Appearance of problems in the process of fertilization or termination of pregnancy due to fetal demise will cause primary infertility. Infertility is caused by various factors. It can occur with either male or female sexual problems or it may have combined reasons affecting both the man and the woman (2).
Prevalence of primary infertility is reported to be 10% to 12% (3). Moreover, fertility and the number of children are decreasing throughout the world (3). The percentage of women who did not conceive a child till the age of 44 was reported as 1.4% to 17.1% with an average of 8.4% (4). The rate of primary infertility in 2004-2005 was 24.9% and the rate of lifetime infertility was reported 3.4% (5). Barooti studied 1992 women between the ages of 20 to 30 years in Tehran and revealed that 78.1% of women conceived during the first year of marriage and the prevalence of the primary infertility was 21.9 % (6). These findings were above the world’s average. One of the latest published studies reported the primary infertility in Iran to be 8 % (7).
Considering the above-mentioned reports and their diversity, we inevitably have to plan and carry out a national study with a robust methodology to better address this problem in the country. None of previous studies on prevalence of primary infertility in Iran was based on a complete reproductive history of women for finding all the existing problems and related issues. The present study is based on fertility history and behavior in order to remove the major causes of bias.
Material and Methods
This research was a cross-sectional study based on reproductive history, which was planned and done by Avicenna Research Institute in 2010-2011. In this research, we investigated the history of women’s fertility through investigating the issues such as pregnancy prevention methods, interruptions in preventive methods, pregnancy, labor, and abortion, reproductive treatments, interruption in reproductive treatments, and divorce and separation from the date of marriage until the time of interview. We developed an appropriate questionnaire and piloted it three times to remove the ambiguities and make sure about its clarity. Finally, the Institute’s Research Committee verified the approved questionnaire.
The study population consisted of all married women aging 20 to 40 years throughout Iran. The inclusion criteria were being Iranian, being married and having permanent residence in the country. The exclusion criteria were not agreeing to take part in the study and not having temporary residence in the country.
Unlike similar studies, which included women up to the age of 45 or even 50, we evaluated women between the ages of 20 to 40 to prevent recall bias and questionnaires were being filled according to the history of women’s fertility, which required the interviewees to recall from memory.
Overall, 1000 clusters were randomly selected according to the post office codes, proportionate to the population of the province. In a few provinces like Ilam, South Khorasan and Kohgiluyeh & Boyerahmad in which the number of clusters was less than 12, we raised this number up to 12, making the total number of 1011 clusters. After preparing the family index, we called on the neighbor houses in a clockwise fashion. In each cluster, the interviewers fulfilled 17 questionnaires. The interviewers were trained nurses or midwifes. The Research Committee verified their capability before starting the research. In compiling the data, 280 interviewers in groups of two were sent to the selected cluster that has been assigned and mapped by the study managerial team. After calling on the families, the interviewers introduced themselves first and after explaining about the study, interviewed the cases who had the inclusion criteria.
The interviewers first inquired about, recorded the general and demographic information of the participants, and then asked about their fertility status and past and present medical problems.
As mentioned previously, reproductive history of fertility was used in this study. The comprehensive methodology for calculation of primary infertility based on reproductive history and its advantages from other alternatives has been reported previously (8). In summary, the following formula was used for the calculation of primary infertility:
Where A5, A6, A7, B10, B11, B12 were defined in the flowchart (Fig. 1).
Fig. 1:

The flowchart used for inquiring about the history of fertility in the country in order to determine the rate of primary infertility
In order to check different assumptions that can be used in calculation of infertility rate, we performed sensitivity analysis regarding two groups: In above formula all seeking treatment women were considered infertile (A6, B11). As a sensitivity analysis, we have considered part of this group who got pregnant in the first year after marriage or contraceptive discontinuation (A10, B15) as fertile women.
Women who had unsafe contraception and got pregnant meanwhile. This group has been eliminated from both numerator and denominator in the above calculation. The main reason for this elimination is that unintended pregnancies are fertile subgroup of ineffective contraceptive users while infertile subgroup of this cohort is not easily distinguished. Generally, they will continue contraception or have not experienced at least one year after contraceptive discontinuation (so will discarded from calculation). Thus, both including and excluding this group will produce bias. In the above formula, we exclude this group because we believe that exclusion of these women will produce less bias. However, as a sensitivity analysis to see the effect of this assumption, we also considered them as fertile women. These two corrections lead to obtain the lower rate of infertility.
We used Stata software program, version 12.0 to calculate primary infertility rate and its confidence interval. In all data analysis, P-value of 0.05 or less was considered significant.
Results
In total, we questioned 17187 women in 1011 clusters. The response rates of people were about 80%. The primary infertility rate and its 95% confidence interval was 20.2 (19.4, 20.9) in the whole country. This rate was lower in urban areas comparing to rural areas (19.9 versus 22.0) which is not statistically significant (P-value=0.058). By considering unintended pregnancies (B3) and seeking treatment with pregnancy during the first year (A10, B15) as fertile women, the infertility rate for the whole country become about 18%.
The mean age of women having their first pregnancy is 21.1. In general, the age of first pregnancy in rural areas was about one year less than urban areas (Table 1). Moreover, the mean age of both women and men at the time of marriage was lower in rural areas than urban areas.
Table 1:
The indicators of fertility and the rate of infertility in Iran
| Region | Primary Infertility Rate (CI* 95%) | The mean age of women in the first pregnancy | The mean age of women at the time of marriage | The mean age of men at the time of marriage |
|---|---|---|---|---|
| Country | 20.2 (19.4, 20.9) | 21.1 | 20.1 | 25.4 |
| Urban areas | 19.9 (19.1, 20.7) | 21.2 | 20.2 | 25.6 |
| Rural areas | 22.0 (20.0, 24.2) | 20.4 | 19.4 | 24.1 |
* Confidence Interval
The primary infertility rate has been compared between different provinces (Table 2). The provinces are divided into three groups.
Table 2:
Comparison of the prevalence of primary infertility in different provinces of Iran
| *Lower than the country's average (Group 1) | The same as the country's average (Group 2) | *Higher than the country's average (Group 3) |
|---|---|---|
| Ilam, Semnan, Kordestan, Gilan, Lorestan | East Azarbayejan, Alborz, Bushehr, Tehran, Cha-harmahal & Bakhtiyari, Khorasan-e- Razavi, North Khorasan, Zanjan, Sistan & Baluchestan, Fars, Qazvin, Kerman, Kermanshah, Kohgiluyeh & Boy-erahmad, Golestan, Markazi, Mazandaran, Hor-mozgan, Hamedan, Esfahan, Yazd | West Azarbayejan, Ardebil, South Khorasan, Khuzestan, Qom |
*Difference is statistically significant with the country average (P value less than 0.05).
Group 1 contains provinces that are significantly lower than country average. Group 3 contains provinces that are significantly higher than country average and finally group 2 contains provinces that are not significantly different from country average. In addition, spatial representation of in fertility rate was shown to provide visual comparison between different provinces (Fig. 2).
Fig. 2:

Spatial Representation of Primary Infertility Rate in Iran in Year 2011
The prevalence of infertility according to the age of women at the time of their marriage has been shown in Fig. 3.
Fig. 3:
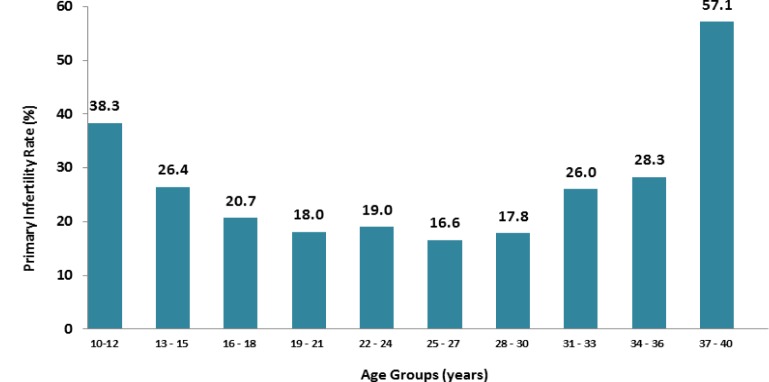
Percentage of Primary Infertility according to the Age Group of Women at the Time of Marriage
Discussion
Infertility is an important issue that has major impact on the health of individuals and the societies. The rate of infertility changes among populations and during different times. Advantages in diagnosis and use of modern treatment techniques have been increasing recently, but finding and calculation of the exact infertility rate is still a problem. In order to assess the trend of fertility, a quantitative and reliable method for assessing infertility is needed.
In the study, the prevalence of primary infertility (using reproductive history) in Iran was 20.2%, which is considerably higher than the world average (9–11). In the sensitivity analysis when we considered unintended pregnancies (B3) and seeking treatment (A10, B15) as fertile, the rate of infertility become 18%, which is still higher than world average. The results of this research are compatible with Vahidi (5) and Barooti (6) but not with Safarinejad (7). Some evidences show that there is a decline in fertility (12, 13); this is an important point that may have happened in Iran but some differences in prevalence of primary infertility are seen due to differences in definitions and epidemiologic study designs and this is the most probable reason for the observed difference in the result of Safarinejad’s study (7) in comparison with other previous studies in Iran. In order to assess the trend of fertility and approaching this challenge, a quantitative and reliable method for assessing infertility is needed. The methodology introduced in this study can estimate the primary infertility rate with the least biases.
The result of the study for the prevalence of primary infertility according to the age group of women showed increasing pattern for the age group younger than 18 and older than 30 years old; According to these results, the ages ranging from 19 to 30 years are the appropriate ages for Iranian women to conceive. This finding is compatible with pattern and relation of the fertility with the age of the women in other epidemiological studies in Iran (5, 6, 14). In the review of infertility epidemiology in Iran, Mohammad and Ardalan found the lowest rate of primary infertility was for women aged 21 to 26 years (17.2 %) which is compatible with the results of the current research (14).
In most provinces, the primary infertility rate was not significantly different from the mean calculated for the whole country. Indeed small sample size cause large variances for the estimated rates and as a result, significant differences are not recognized. This issue led to different results in table 2 and Figure 2. For example, the rate of infertility was higher in Chaharmahal & Bakhtiyari than Khuzestan. However, Chaharmahal and Bakhtiyari Province was not significantly different from country mean while Khuzeatan was significantly higher than the country mean. In the future research, we will use mixed model to analyze and interpret the result of this study. Applying this model will reduce the variance of rate and will increase the accuracy of results.
Considering the infertility rates which was significantly lower or upper than the country average, no significant spatial or geographical pattern was observed. However, Safarinejad (7) reported the higher level of primary infertility in southern provinces of Iran.
Although we can justify some of the differences, such as the effect of different periods, sampling method or physiological changes, but it seems the main reason for the differences lies in collecting methods and analyzing the information. The methodology of this research created a new way to evaluate our objective and estimate the unbiased rate of primary infertility. We, therefore, recommend this methodology for the upcoming research, too.
Conclusion
The prevalence of primary infertility in Iran seems to be higher than the world average. Therefore, it is crucially important to support the large number of couples who face infertility. This problem is more serious in some provinces as shown in the infertility map.
Ethical considerations
Ethical issues (Including plagiarism, Informed Consent, misconduct, data fabrication and/or falsification, double publication and/or submission, redundancy, etc.) have been completely observed by the authors.
Acknowledgment
We thank from Avicenna Research Institute that has supported the project financially. The authors declare that there is no conflict of interest.
References
- Thonneau P, Spira A (1991). Prevalence of infertility: international data and problems of measurement. Eur J Obstet Gynecol Reprod Biol, 38(1): 43–52. [DOI] [PubMed] [Google Scholar]
- Cooper TG, Noonan E, von Eckardstein S, Auger J, Baker HW, Behre HM, et al. (2010). World Health Organization reference values for human semen characteristics. Hum Reprod Update, 16 (3): 231–245. [DOI] [PubMed] [Google Scholar]
- World Health Organization (2004). Demographic and Health Surveys (DHS) Comparative reports No. 9: Infecundity, infertility, and childlessness in developing countries. [Google Scholar]
- Savitz DA, Hertz-Picciotto I, Poole C, Olshan AF (2002). Epidemiologic measures of the course and outcome of pregnancy. Epidemiol Rev, 24(2): 91–101. [DOI] [PubMed] [Google Scholar]
- Vahidi S, Ardalan A, Mohammad K (2009). Prevalence of primary infertility in the Islamic Republic of Iran in 2004–2005. Asia Pac J Public Health, 21(3): 287–293. [DOI] [PubMed] [Google Scholar]
- Barooti A, Ramezani Tehrani F, Heydari Seraj M, Ashrafi M (1999). Primary sterility according to marriage age. Hakim, 10: 88–93. [Google Scholar]
- Safarinejad MR (2008). Infertility among couples in a population based study in Iran: prevalence and associated risk factors. Int J Androl, 31(3): 303–314. [DOI] [PubMed] [Google Scholar]
- Akhondi MM, Kamali K, Ranjbar F, Shafeghati S, Behjati Ardakani Z, Shirzad M, et al. (2012). Introducing a Quantitative Method to Calculate the Rate of Primary Infertility. Iran J Public Health, 41(12): 54–59. [PMC free article] [PubMed] [Google Scholar]
- World Health Organization (2000). Reproductive Health report indicators for Global monitoring, Report of second intraagency meeting. [Google Scholar]
- United Nations (2010). World Fertility Report 2007. [Google Scholar]
- Chandra A, Martinez GM, Mosher WD, Abma JC, Jones J (2005). Fertility, family planning, and reproductive health of U.S. women: Data from the 2002 National Survey of Family Growth. Vital Health Stat, 23(25): 1–160. [PubMed] [Google Scholar]
- Guzick DS, Swan S (2006). The decline of infertility: apparent or real? Fertil Steril, 86(3): 524–526. [DOI] [PubMed] [Google Scholar]
- Stephen EH, Chandra A (2006). Estimating infertility: not the last word. Fertil Steril, 86(3): 534. [DOI] [PubMed] [Google Scholar]
- Mohammad K, Ardalan A (2009). An Overview of the Epidemiology of Primary Infertility in Iran. J Reprod Infertility, 10(3): 213–216. [PMC free article] [PubMed] [Google Scholar]