

Abstract
Background:
A motor vehicle seat belt use law for the driver and front-seat passenger was implemented in Taiwan on June 1, 2001. The purpose of this study was to determine the effect of motor vehicle seat belt use on the severity of traumatic brain injuries because of motor vehicle accidents.
Methods:
Data were collected from 27 major teaching hospitals four years before June 1, 2001 and until May 31, 2013. A total of 822 brain-injured patients with a mean age of 37.4 (± 13.4) years were included; 251 were injured prior to implementation of the law and 571 after. The Glasgow coma scale was adapted to rate the severity of traumatic brain injury on admission. The Glasgow outcome scale was used to categorize the outcome on discharge.
Results:
After the seat belt law was implemented, traumatic brain injuries were less severe (P<0.001) and the rates of loss of consciousness, neurologic deficit, intracranial hematoma, craniotomy, and poor physical condition at discharge were all significantly lower (all P< 0.05). Male gender, longer hospital stays, not wearing a seat belt, and injury before the law was enacted were all associated with poorer physical condition at the time of discharge (all P <0.01).
Conclusion:
Among occupants who survived a motor vehicle accident but had traumatic brain injuries, those who had worn seat belts had a better prognosis. Seat belts remain one of the best methods to reduce both the severity of injuries and the number of fatalities.
Keywords: Glasgow coma scale, Motor vehicle accident, Seat belt, Traumatic brain injury
Introduction
Road traffic injuries are a major global public health issue (1, 2). In Taiwan, data provided by the Ministry of Health and Welfare showed that the mortality rate from traffic injury was 16.8/100,000 in 2008 (3). This was higher than the rates of 14.5/100,000 in the United States, 5.4 in Japan, 5.8 in Singapore, 15.7 in Republic of Korea, 5.0 in England, and 6.2 in Germany in 2008(4), but lower than 39 in Iran (5).
Of the various types of accidental injuries, traumatic brain injury is regarded as most important, because about half of injury-induced deaths are related to traumatic brain injury (6). About 10% of traumatic brain injuries in Taiwan are caused by motor vehicle accidents (7).
Multiple studies in the United States (8, 9), Italy (10), Germany (11), and France (12) have shown that mandatory seat belt use reduced the frequency of traumatic brain injuries. In Taiwan, a seat belt use law was implemented nationwide on June 1, 2001 and motor vehicle drivers caught by the police not using their seat belts could be fined. Drivers and front-seat passengers have been subject to a fine of US$50 for failure to fasten their seatbelts, and drivers are subject to a fine of US$100–200 if they fail to use their seat belt while driving on a freeway or expressway. Starting in 2012, drivers of sedans have been subject to a fine of US$50 when back seat passengers fail to use their seat belts. Despite the law and monetary penalties for failure to use seat belts, there has been widespread resistance to their use. Arguments have included infringement on personal freedom and discomfort.
Because there have been no comprehensive studies in Taiwan indicating that seat belts indeed exert a protective effect in auto accidents, we hope that this study will confirm the benefit of the seat belt legislation, encourage Taiwan to strengthen enforcement of this measure, reduce the severity of external head injuries in auto accidents, and thereby lessen household economic losses and the consumption of medical resources.
The aim of this study was to determine the effect of this new law for car driver and front-seat passenger on the severity of traumatic brain injuries because of motor vehicle accidents. Verification of the benefit of this safety belt legislation would hopefully increase seatbelt compliance in Taiwan.
Methods
Data Collection
In this case-series study, data on motor vehicle-related traumatic brain injuries for car driver and front-seat passenger were collected for the 4 years before (June 1, 1997–May 31, 2001) and 12 years after (June 1, 2001–May 31, 2013) implementation of the seat belt law. The data were collected from the 27 major teaching hospitals in Taiwan, which have been part of the Traumatic Brain Injury Registry of the Ministry of Health and Welfare since 2002 when the number was reduced from the 56 hospitals, which were first included in 1994.
Twenty-three hospitals in Taipei are representative of urban areas and 4 in the Hualien area are representative of rural areas. All of these hospitals have neurosurgery departments. Patients dead on arrival and non-hospitalized patients were excluded from this study, as were those without information about seat belt use (Fig. 1). Most information about seat belt use (74.2%) was taken from police reports. If that source were not available, then patients provided the information. Since it was part of the hospital record and confidential, it was not shared with the police for possible prosecution and there was no incentive for providing false information.
Fig. 1:
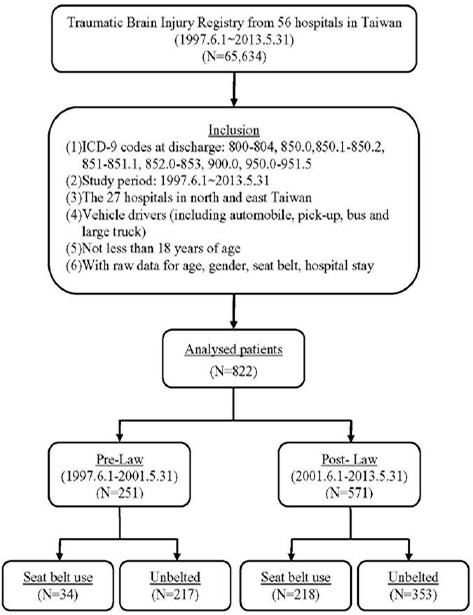
Flow chart of the study
Data about traumatic brain injuries were recorded by experienced neurosurgeons at each hospital and were extracted by the same research assistant from the Injury Prevention Center to maximize reliability and consistency. Cases were identified by International Classification of Diseases, Ninth Revision (ICD-9) classifications (i) fracture of skull or face bones, (ii) concussion, (iii) cerebral/cerebellar/brain stem contusion or laceration, (iv) extracerebral and/or intracerebral hematoma, subarachnoid hemorrhage, subdural hematoma, epidural hemorrhage, intracranial hemorrhage, (v) unspecified intracranial injury, (vi) injury to blood vessels of head and neck, and (vii) injury to cranial nerves. A thorough review of inpatient medical records and related examinations of all traumatic brain injury patients was carried out. Data pertaining to the identification of possible variables implicated in motor vehicle-related traumatic brain injuries were recorded; these were age, gender, and Glasgow Coma Scale (GCS) score. The GCS is scored as follows: 1) severe: score of 8 or below; 2) moderate: score of 9 to 12; 3) mild: score of 13 to 15, or condition not meeting any of the above criteria. The Glasgow Outcome Scale was used to categorize the outcome on discharge: good recovery, moderate disability - disabled but independent, severe disability - conscious but dependent, persistent vegetative state, and death. The study was approved by the Institutional Review Board of Taipei City Hospital.
Statistical analysis
Continuous variables were expressed by median and inter-quartile range (IQR) and compared by the Mann-Whitney U test. Categorical variables were expressed by count and percentage and compared by the Chi-square test or Fisher’s exact test. Univariate and multivariate logistic regression models were utilized to investigate the independent factors associated with physical condition at discharge. Odds ratios (OR) with corresponding 95% confidence intervals (95%CI) were determined for the univariate logistic regression analysis. Variables with a significant association with physical condition at discharge (P<0.2) in the univariate logistic regression model were selected for multivariate analyses. Adjusted ORs (aOR) with 95%CI to identify an association with physical condition at discharge were then calculated. A two-tailed P value < 0.05 was considered statistically significant. Statistical analyses were performed with SAS software version 9.2 (SAS Institute Inc., Cary, NC).
Results
A total of 822 brain-injured patients (561 males and 261 females) with a mean age of 37.4 (SD=13.4) years were retrospectively reviewed and included in this study. Of these 822 patients, 251 had motor vehicle accidents before the law was implemented (1997.6.1–2001.5.31), and the other 571 after that (2001.6.1–2013.5.31) (Supplement Table 1). Among those patients who had accidents, 252 (30.7%) had worn seat belts and 570 (69.3%) had not. Table 1 shows the characteristics of motor vehicle occupants with and without belts. More wore seat belts after the law was implemented. Those with seat belts had a lower median hospital stay than those without seat belts (6[4, 12] vs. 8[4, 15], P=0.026). There was a significant difference between those with and without belts in the distribution of physical conditions at discharge (P < 0.001), as many more of the former made a good recovery (Table 1). In addition, Fig. 2 shows that those subjects without belts had a significantly higher rate of poor physical condition than those with belts after the law was implemented (18.3% vs. 7.4%, P<0.001). Before the law was implemented, physical condition was similar between subjects with and without belts (25% vs. 29.9%, P=0.570) (Fig. 2).
Table 1:
Characteristics of motor vehicle occupants with and without seat belt use
| Variables | Belted (n=252) | Unbelted (n=570) | P value |
|---|---|---|---|
| Age, yr | 35 (28.3, 44) | 35 (26, 46) | 0.807 |
| Gender | 0.015 * | ||
| Female | 95 (36.4%) | 166 (63.6%) | |
| Male | 157 (28.0%) | 404 (72.0%) | |
| Law implementation | <.001 * | ||
| Pre-Law (1997.6.1–2001.5.31) | 34 (13.5%) | 217 (86.5%) | |
| Post-Law (2001.6.1–2013.5.31) | 218 (38.2%) | 353 (61.9%) | |
| Hospital stay, days | 6 (4, 12) | 8 (4, 15) | 0.026 * |
| Glasgow Outcome Scale | <.001 * | ||
| Good recovery | 223 (90.3%) | 413 (77.6%) | |
| Moderate disability | 12 (4.9%) | 47 (8.8%) | |
| Severe disability | 7 (2.8%) | 36 (6.8%) | |
| Vegetative state | 0 (0%) | 3 (0.6%) | |
| Death | 5 (2.0%) | 33 (6.2%) |
Continuous variables were expressed by median and IQR, which were then compared between belted and unbelted groups by the Mann-Whitney U test. Categorical variables were expressed by count and percentage, which were then compared between belted and unbelted groups by the Chi-square test or Fisher’s exact test.
indicates a significant difference between belted and unbelted groups.
Fig. 2:
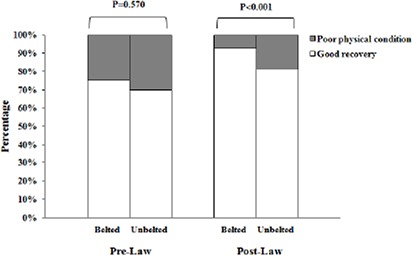
Physical condition at discharge of belted and unbelted subjects before and after the law was implemented. Differences were compared using Pearson’s Chi-square test. P<0.05 indicates a significant difference between belted and unbelted subjects
The rates of loss of consciousness, neurologic deficit, intracranial hematoma and craniotomy were significantly lower for subjects with belts than for those without belts (all P< 0.05). There was also a significant difference in the distribution of severity as rated by the GCS (P < 0.001). Rates of motor vehicle-related traumatic brain injuries were similar in belted and unbelted occupants before the law was implemented (Table 2).
Table 2:
Comparison of motor vehicle-related traumatic brain injuries between belted and unbelted occupants before and after implementation of the Taiwan seat belt use law
| Overall | Belted, n(%) (n=252) | Unbelted, n(%) (n=570) | P value |
|---|---|---|---|
| Loss of consciousness | 78 (31.0) | 208 (38.2) | 0.048 * |
| Amnesia | 37 (14.8) | 104 (19.3) | 0.123 |
| Neurologic deficit | 24 (9.5) | 95 (17.2) | 0.004 * |
| Skull fracture | 23 (9.1) | 74 (13.3) | 0.090 |
| Intracranial hematoma | 73 (29.1) | 218 (39.0) | 0.007 * |
| Craniotomy | 21 (8.4) | 78 (13.9) | 0.027 * |
| Severity (GCS) | <.001 * | ||
| Mild | 205 (81.4) | 393 (69.5) | |
| Moderate | 30 (11.9) | 80 (14.2) | |
| Severe | 17 (6.7) | 92 (16.3) | |
| Pre-Law implementation | (n=34) | (n=213) | |
| Loss of consciousness | 19 (55.9)) | 91 (42.9) | 0.158 |
| Amnesia | 15 (44.1) | 61 (29.5) | 0.088 |
| Neurologic deficit | 8 (23.5) | 56 (26.8) | 0.689 |
| Skull fracture | 4 (11.8) | 33 (15.6) | 0.565 |
| Intracranial hematoma | 16 (47.1) | 95 (44.6) | 0.789 |
| Craniotomy | 7 (20.6) | 38 (17.8) | 0.700 |
| Severity (GCS) | 0.482 | ||
| Mild | 21 (61.8) | 123 (57.7) | |
| Moderate | 8 (23.5) | 40 (18.8) | |
| Severe | 5 (14.7) | 50 (23.5) | |
| Post-Law implementation | (n=217) | (n=350) | |
| Loss of consciousness | 59 (27.1) | 117 (35.1) | 0.047 * |
| Amnesia | 22 (10.2) | 43 (13.0) | 0.322 |
| Neurologic deficit | 16 (7.3) | 39 (11.4) | 0.118 |
| Skull fracture | 19 (8.7) | 41 (11.9) | 0.231 |
| Intracranial hematoma | 57 (26.3) | 123 (35.5) | 0.022 * |
| Craniotomy | 14 (6.5) | 40 (11.4) | 0.050 |
| Severity (GCS) | 0.029 * | ||
| Mild | 184 (84.4) | 270 (76.7) | |
| Moderate | 22 (10.1) | 40 (11.4) | |
| Severe | 12 (5.5) | 42 (11.9) |
Categorical variables were expressed by count and percentage, which were then compared between belted and un-belted groups by the Chi-square test.
indicates a significant difference between belted and unbelted groups.
The rate of total associated injuries was significantly higher in unbelted subjects (P <0.001). Among these patients with injuries, the rates of whole spine fractures and facial fractures were significantly lower for subjects with belts than for those without them (all P <0.05); however, the rate of other injuries was similar for both groups (Table 3). A logistic regression model was utilized to investigate the independent factors associated with poor physical condition including disability, vegetative state and death at discharge. Gender, belt use, implementation of the law, and duration of hospital stay were the independent factors associated with poor physical condition at discharge (all P <0.001). After adjustment for other risk factors, males had a higher rate of poor physical condition at discharge than did females (aOR = 1.94, 95% CI: 1.20–3.11, P = 0.006). For each 1 day increase in hospital stay, the odds ratio (OR) increased by 1.04 (95% CI: 1.03–1.05, P < 0.001).
Table 3:
Injuries to body regions other than the head between belted or unbelted traumatic brain-injured motor vehicle accident victims in Taiwan
| Variables | Belted, n(%) (n=252) | Unbelted, n(%) (n=570) | P value |
|---|---|---|---|
| Total associated injuries | 118 (47.0) | 360 (64.1) | <.001 * |
| Whole spine fracture | 13 (5.2) | 53 (9.4) | 0.040 * |
| Facial fracture | 24 (9.6) | 123 (21.9) | <.001 * |
| Chest injury | 23 (9.2) | 62 (11.0) | 0.421 |
| Abdominal injury | 6 (2.4) | 20 (3.6) | 0.382 |
| Upper extremity fracture | 11 (4.4) | 37 (6.6) | 0.219 |
| Lower extremity fracture | 25 (10.0) | 49 (8.7) | 0.570 |
| Cervical spine | 12 (4.8) | 48 (8.6) | 0.057 |
| Thoracic spine | 4 (1.6) | 13 (2.3) | 0.605 |
| Lumbar spine | 2 (0.8) | 13 (2.3) | 0.137 |
Categorical variables were expressed by count and percentage, which were then compared between belted and unbelted by the Chi-square test or Fisher’s exact test.
indicates a significant difference between belted and unbelted groups.
Implementation of the law was also associated with improved physical condition (aOR = 0.44, 95% CI: 0.29–0.66, P < 0.001) (Table 4).
Table 4:
Relationship between seatbelt use and poor physical condition at discharge (disabled, vegetative state and death): north and east Taiwan, June 1997–May 2013
| Variables | Univariate | Multivariate | ||
|---|---|---|---|---|
| OR(95% CI) | P value | aOR(95% CI) | P value | |
| Age, years | 0.993 (0.979, 1.007) | 0.299 | ||
| Gender | ||||
| Female | 1 | 1 | ||
| Male | 2.272 (1.449, 3.562) | <.001 * | 1.936 (1.204, 3.112) | 0.006 * |
| Belt use | ||||
| Belted | 1 | 1 | ||
| Unbelted | 2.677 (1.677, 4.274) | <.001 * | 1.939 (1.179, 3.189) | 0.009 * |
| Law implementation | ||||
| Pre-law | 1 | 1 | ||
| Post-law | 0.398 (0.273, 0.579) | <.001 * | 0.439 (0.293, 0.659) | <.001 * |
| Hospital stay, days | 1.042 (1.029, 1.054) | <.001 * | 1.041 (1.028, 1.054) | <.001 * |
OR, odds ratio; CI, confidence interval; aOR, adjusted OR.
indicates independent factors associated with the severe traumatic brain injury, poor physical condition at discharge (disabled, vegetative state, and death).
Discussion
After implementation of a seat belt law for the driver and front-seat passenger on June 1, 2001, more Taiwanese motor vehicle accident victims (38.2%) wore them than had those prior to implementation (13.5%). This rate was much lower than that reported in the United States (87%) (13), but higher than that in Nigeria (18.7%) (14).
According to statistics from the National Police Administration, the rate of seat belt use among persons killed in motor vehicle accidents between 2003 and 2012 was 70.7%. The average rate of seat belt use among persons injured in motor vehicle accidents between 2003 and 2012 was 89%. Furthermore, the rate of injury to persons with seat belts decreased annually from 93.2% in 2003) to 85.6% in 2012. (http://talas-pub.iot.gov.tw/TBfiles/101_A.aspx). This study found that after the seat belt law was implemented, the seat belt use rate among drivers suffering traumatic brain injuries in accidents was only 38.2%, indicating that the rate of seat belt use among persons suffering external head injuries was quite low.
There were more traumatic brain injuries among males than among females for all age groups, with a peak in the 35- to 54-year-old group. Being male was also associated with poorer physical status at discharge. This was consistent with a previous study in France (12).
Following accidents, people who used their seat-belts had an average of 2 fewer days of hospitalization than people who failed to use them. According to data compiled by Taiwan’s National Health Insurance Administration in 2013, people who used their seat belts reduced medical expenditures by US$310 compared with people who failed to use them. Unbelted traumatic brain injury patients result in a significant burden on hospitals in terms of increased incidence and severity of injuries to victims, use of more hospital resources, and a greater financial burden. Results of this study were consistent with those of Metzger et al. who found that between 1995 and 2000, unbelted occupants involved in motor vehicle accidents had 1.52 more lost workdays than belted occupants. This was approximately 7.3 million workdays, $566 million in lost wages, and $1.25 billion in workplace costs (15).
Our data showed that seat belt use did not increase the risk of injuries to other body regions, such as the abdomen and chest. This was similar to the findings of Porter et al. (16) while the use of seat belts by obese individuals will increase risk of abdominal injury (17), information about body weight or BMI (body mass index) was not available in this study.
Persons who fail to use their seat belts experience a far greater force of impact in an auto accident than persons who fasten their seat belts (18). When a vehicle is in a collision, the greatest potential hazard of not wearing a seatbelt lies in the possibility of secondary impact. It has been found from collision experiments that motorists who fail to fasten their seat belts will be propelled forward and upward due to inertia, causing their chest to strike inevitably the steering wheel, and their forehead to strike the glass of the windshield, resulting in injury. Similarly, passengers who do not use their seat belts are often killed or severely injured due to impact or being thrown from the vehicle. When drivers do use their seat belts, the tension of the seat belt in the event of a collision will prevent their bodies from striking the steering wheel or glass of the windshield, providing an added layer of protection. This study's finding that the use of seat belts can reduce the severity of external head injuries, including the chance of death, loss of consciousness, neurologic deficit, intracranial hematoma, craniotomy, and facial fracture, indicated that seat belts can protect the head and body by reducing the force of impact and lessen the chance that motorists will suffer external injury when their head strikes the steering wheel or windshield.
After 2001, traumatic brain injuries were less severe and the rates of loss of consciousness, neurological deficit, intracranial hematoma, craniotomy, and poor physical condition at discharge were all lower. These findings might suggest that mandatory seat belt use reduced the number of traumatic brain injuries; however, no data were available about accident victims who died at the scene and were not brought to a hospital.
It is very difficult to judge about factors related to decline of road traffic injury (RTI) and death. This decrease of RTI and fatal RTI might be an indicator of one of the following factors: improved safety of modern vehicles, avoidance of high-risk driving behaviors, wearing helmets, seatbelts, and the increased congestion in the cities. Increased congestion decreases the speed of motor vehicles. Thus, crashes cause minor injuries and fewer deaths (19). Possible factors involved in the decrease in RTI and deaths are due to a variety of interventions, including: seat belt legislation for drivers and front passengers, helmets for motorcycle riders, direct police enforcement, police cameras for monitoring speeding, improved health care facilities, public education campaigns, the police school assistance program, and identification of hazardous locations on the country’s main road network (5, 20). Developing infrastructure to support automated enforcement may be the best solution for speeding/not using seat belts on the roadway (21). On the other hand, although the increase in attitude and behavior was followed by a decrease in road traffic crashes (RTC), the attitude of drivers has a crucial effect on decreasing the number of RTC of drivers (22).
Seat belts remain our best defense in reducing both the severity of injuries and the number of fatalities. Seat belts restrain occupants and minimize the effects of the extreme forces involved in a motor vehicle crash. This is of particular concern in the case of pregnant women. Several studies have documented the concern that seat belts themselves might cause injury or that people did not understand the benefit of the use of restraint (23, 24). Appropriate knowledge about correct seat belt placement could potentially increase the level of comfort while wearing a seat belt (25).
This study had several limitations. We did not collect data about pregnancy or the reason for failure to use seat belts. We used tertiary hospital–based data, which might not reflect the overall traumatic brain injury distribution in the study areas and data were limited to that from hospitals chosen by the Ministry of health and Welfare to continue to be part of the Traumatic Brain Injury Registry. Patients who were dead on arrival or those who were seen in the emergency room but did not require hospitalization were excluded from the study. There was no information about airbags, so that we were unable to determine whether safety measures other than seat belts affected the severity of injuries. While this study did not examine records indicating the directions of vehicle collisions, the direction of a collision may also affect the severity of injuries.
Conclusion
Taiwan implemented legislation requiring motor vehicle drivers and front seat passengers to use seat belts on June 1, 2001, and implemented further legislature requiring backseat passengers to also use seat belts in February 2012. This is the first formal study to verify the protective effect of seat belts in Taiwan. Among occupants who survived a motor vehicle accident but had traumatic brain injuries, those who had worn seat belts had a better prognosis. Seat belts remain one of the best methods to reduce both the severity of injuries and the number of fatalities.
Ethical considerations
Ethical issues (Including plagiarism, informed consent, misconduct, data fabrication and/or falsification, double publication and/or submission, redundancy, etc.) have been completely observed by the authors.
Annual totals of brain-injured patients
| year | 1997.6.1–2001.5.31 (n=251) | 2001.6.1–2013.5.31 (n=571) | Total |
|---|---|---|---|
| 1997 | 62 | 0 | 62 |
| 1998 | 77 | 0 | 77 |
| 1999 | 47 | 0 | 47 |
| 2000 | 46 | 0 | 46 |
| 2001 | 19 | 38 | 57 |
| 2002 | 0 | 34 | 34 |
| 2003 | 0 | 42 | 42 |
| 2004 | 0 | 41 | 41 |
| 2005 | 0 | 50 | 50 |
| 2006 | 0 | 53 | 53 |
| 2007 | 0 | 52 | 52 |
| 2008 | 0 | 54 | 54 |
| 2009 | 0 | 52 | 52 |
| 2010 | 0 | 51 | 51 |
| 2011 | 0 | 44 | 44 |
| 2012 | 0 | 43 | 43 |
| 2013 | 0 | 17 | 17 |
Acknowledgments
This study was supported by a grant (NHRIEX99-9707PI) from the National Health Research Institute, Taiwan. The authors thank the directors and staff of the collaborating hospitals for their full support and for providing complete and invaluable data. The authors declare that there is no conflict of interests.
References
- 1. Peden M, Scurfield R, Sleet D, Mohan D, Hyder AA, Jarawan E, et al. (2004). World report on road traffic injury/prevention . Geneva : : World Health Organization ; . [Google Scholar]
- 2. Bastida JL, Aguilar PS, Gonzalez BD. (2004). The economic costs of traffic accidents in Spain. J Trauma, 56: 883–8. [DOI] [PubMed] [Google Scholar]
- 3. Anonymus (2010). Vital Statistics in Taiwan . Ministry of Health and Welfare ; , Taiwan : . [Google Scholar]
- 4. Anonymus (2011). Health statistics and information systems . Department of Measurement and Health Information, World Health Organization ; . [Google Scholar]
- 5. Rasouli MR, Nouri M, Zarei MR, Saadat S, Rahimi-Movaghar V. (2008). Comparison of road traffic fatalities and injuries in Iran and other countries. Chin J Traumatol, 11: 131–4. [DOI] [PubMed] [Google Scholar]
- 6. Lin JW, Lin CM, Tsai JT, Hung KS, Hung CC, Chiu WT. (2008). Neurotrauma research in Taiwan . Acta Neurochir Supp ,. 101 : 113 – 7 . [DOI] [PubMed] [Google Scholar]
- 7. Lin JW, Tsai SH, Tsai WC, Chiu WT, Chu SF, Lin CM, et al. (2006). Survey of Traumatic intracranial hemorrhage in Taiwan. Surg Neurol, 66 S2: 20 – 5 . [DOI] [PubMed] [Google Scholar]
- 8. Lestina DC, Williams AF, Lund AK, Zador P, Kuhlmann TP. (1991). Motor vehicle crash injury patterns and the Virginia seat belt law. JAMA, 265: 1409–13. [PubMed] [Google Scholar]
- 9. Redelmeier DA, Blair PJ. (1993). Survivors of motor vehicle trauma; an analysis of seat belt use and health care utilization. J Gen Intern Med, 8: 199–203. [DOI] [PubMed] [Google Scholar]
- 10. Campello C, Preite G, Poli A, Zuppichini F, Marigo M. (1996). [Effects of seat belt legislation on injuries of traffic accidents] Epidemiol Prev , 20 : 313 – 7 . [In Italian] [PubMed] [Google Scholar]
- 11. Schrader W, Gramer E, Goldmann F, Marcus U. (2000). [Penetrating and perforating eye injuries in 343 patients due to auto accidents before and after compulsory seat belt legislation resulting in fines (1966–1998)] Klin Monbl Augenheilkd , 217 : 23 – 29 . [In German] [DOI] [PubMed] [Google Scholar]
- 12. Ndiaye A, Chambost M, Chiron M. (2009). The fatal injuries of car drivers. Forensic Sci Int, 184: 21–7. [DOI] [PubMed] [Google Scholar]
- 13. Shults RA, Beck LF. (2012). Self-reported seatbelt use, United States, 2002–2010: does prevalence vary by state and type of seatbelt law? J Safety Res, 43: 417–20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Sangowawa AO, Alagh BT, Ekanem SE, Ebong IP, Faseru B, Adekunle BJ, et al. (2010). An observational study of seatbelt use among vehicle occupants in Nigeria. Inj Prev, 16: 85–9. [DOI] [PubMed] [Google Scholar]
- 15. Metzger J, McGwin G, MacLennan PA, Rue LW. (2004). Is seat belt use associated with fewer days of lost work after motor vehicle crashes? J Trauma, 56: 1009–14. [DOI] [PubMed] [Google Scholar]
- 16. Porter RS, Zhao N. (1998). Patterns of injury in belted and unbelted individuals presenting to a trauma center after motor vehicle crash: seat belt syndrome revisited. Ann Emerg Med, 32: 418–24. [DOI] [PubMed] [Google Scholar]
- 17. Zarzaur BL, Marshall SW. (2008). Motor vehicle crashes obesity and seatbelt use: a deadly combination? J Trauma, 64: 412–9. [DOI] [PubMed] [Google Scholar]
- 18. Mayrose J, Jehle D, Hayes M, Tinnesz D, Piazza G, Wilding GE. (2005). Influence of the un-belted rear-seat passenger on driver mortality: “the backseat bullet”. Acad Emerg Med, 12: 130–4. [DOI] [PubMed] [Google Scholar]
- 19. Rahimi Movaghar V, Zarei MR, Saadat S, Rasouli MR, Nouri M. (2009). Road traffic crashes in Iran from 1997 to 2007. Int J Inj Contr Saf Promot, 16: 179–81. [DOI] [PubMed] [Google Scholar]
- 20. Rahimi Movaghar V. (2010). Factors involved in the past and present history of road traffic injuries and deaths in Iran. Arch Iran Med, 13 : 172 – 3 ; author reply 173–4. [PubMed] [Google Scholar]
- 21. Moradi A, Motevalian SA, Mirkoohi M, McKay MP, Rahimi Movaghar V. (2013). Exceeding the speed limit: prevalence and determinants in Iran. Int J Inj Contr Saf Promot, 20: 307–12. [DOI] [PubMed] [Google Scholar]
- 22. Mirzaei R, Hafezi Nejad N, Sadegh Sabagh M, Ausari Moghaddam A, Eslami V, Rakhshani F, Rahimi Movaghar V. (2014). Dominant role of driver's attitude in prevention of road traffic crashes: a study on knowledge, attitude, and practice of drivers in Iran. Accid Anal Prev, 66: 36–42. [DOI] [PubMed] [Google Scholar]
- 23. Schiff M, Kasnic T, Reiff K, Pathak D. (1992). Seat belt use during pregnancy. Western J Med, 156: 655–7. [PMC free article] [PubMed] [Google Scholar]
- 24. Attico NB, Smith RJ, 3rd, FitzPatrick MB, Keneally M. (1986). Automobile safety restraints for pregnant women and children. J Reprod Med, 31: 187–92. [PubMed] [Google Scholar]
- 25. McGwin G, Russell SR, Rux RL, Leath CA, Valent F, Rue LW. (2004). Knowledge, Beliefs, and Practices Concerning Seat Belt Use During Pregnancy. J Trauma, 56: 670–5. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Annual totals of brain-injured patients
| year | 1997.6.1–2001.5.31 (n=251) | 2001.6.1–2013.5.31 (n=571) | Total |
|---|---|---|---|
| 1997 | 62 | 0 | 62 |
| 1998 | 77 | 0 | 77 |
| 1999 | 47 | 0 | 47 |
| 2000 | 46 | 0 | 46 |
| 2001 | 19 | 38 | 57 |
| 2002 | 0 | 34 | 34 |
| 2003 | 0 | 42 | 42 |
| 2004 | 0 | 41 | 41 |
| 2005 | 0 | 50 | 50 |
| 2006 | 0 | 53 | 53 |
| 2007 | 0 | 52 | 52 |
| 2008 | 0 | 54 | 54 |
| 2009 | 0 | 52 | 52 |
| 2010 | 0 | 51 | 51 |
| 2011 | 0 | 44 | 44 |
| 2012 | 0 | 43 | 43 |
| 2013 | 0 | 17 | 17 |