

Abstract
Objectives
To review the possible causes of the high incidence of urolithiasis in the oil-rich Gulf States.
Methods
Data were extracted from published reports on the incidence of urolithiasis, affluence and diet in the Gulf States, various Western countries and China.
Results
There are strong relationships: (a) between the life-expectancy of stones in men and the Gross National Income (GNI) per capita of these countries; and (b) between the daily consumption of animal protein and GNI per capita. Together these data suggest that the occurrence of stones is proportional to the intake of animal protein, although they also indicate that there are additional factors that further increase the risk of urolithiasis in the populations of the Gulf. The consumption of oxalate in the Gulf is three times higher and that of calcium a half of what it is in Western countries. Thus, the average oxalate/calcium ratio in the intestines of the Gulf populations is five to six times higher than that in Western populations, leading to enteric hyperoxaluria and an increased risk of calcium-oxalate stone formation. The risk is further accentuated by the lower urine volumes, due to the hot, dry climate of the region, and lower excretions of citrate, from the highly acidic urine resulting from the high intake of animal protein. There is a high incidence of uric acid-containing stones from the acidic urine and the hyperuricosuria caused by the high intake of purine.
Conclusions
The high incidence of urolithiasis in the Gulf is due to an adverse combination of dietary and environmental factors.
Abbreviations: CaOx, calcium oxalate; CaP, calcium phosphate; UA, uric acid; GNI, Gross National Income; GDP, Gross Domestic Product; KSA, Kingdom of Saudi Arabia; UAE, United Arab Emirates; PSF, the biochemical probability of stone formation
Keywords: Urolithiasis, Incidence, Affluence, Animal protein consumption, Oxalate, Calcium, Uric acid, pH, Urine volume
Introduction
Urolithiasis is a disorder that is recognised throughout the world, although its incidence varies widely amongst countries [1]. In general, the incidence of kidney stones has been shown to be relatively low in developing countries which have low levels of Gross Domestic Product (GDP) and economies that are dependent mainly on agriculture, but the incidence is higher in the wealthy industrialised countries with high levels of GDP. In the UK there is a strong relationship between the incidence of stones and affluence at three different demographic levels [2]. The highest recorded incidence of upper urinary-tract stones appears to be in the oil-rich states of the Arabian or Persian Gulf, such as the United Arab Emirates (UAE) [3], Kuwait [4] and Saudi Arabia (KSA) [5], where the main types of stones consist of calcium oxalate (CaOx) and/or uric acid (UA) [6,7]. On the other hand, the populations of the countries in this region have fewer calcium phosphate (CaP)-containing stones and fewer infection stones than are reported from most Western countries (Table 1).
Table 1.
The percentage occurrence of different stone types according to the predominant mineral in Kuwait, the KSA, the USA and the UK and between 1975 and 2004.
| Predominant mineral (%) | Kuwait (2004) | KSA (1989) | USA (1975) | UK (1975) |
|---|---|---|---|---|
| UA | 15.5 | 14.6 | 10.1 | 4.5 |
| CaOx | 73.0 | 71.3 | 58.8 | 53.3 |
| CaP | 9.5 | 7.6 | 20.3 | 30.9 |
| Magnesium ammonium phosphate | 1.0 | 3.7 | 9.3 | 9.6 |
| Rare (cystine, etc.) | 1.0 | 2.8 | 1.5 | 1.7 |
In the present article the main risk factors for CaOx and UA stones in the wealthy countries of the Middle East will be reviewed and a hypothesis developed as to why these types of stone formation are so common in that part of the world.
Methods
Data on the life-time expectancy of the forming stones in men were calculated from various publications on urolithiasis in the oil-rich countries of KSA [5,8], Kuwait [4,9] and the UAE [10], and in various countries in the West [1]. Data on international per capita daily food consumption [11–16] and national levels of affluence [17] were taken from previous reports. Data on the 24-h urine composition of men in the Middle East and in the West were taken from published data [3,18]. To be consistent in terms of time, the studies were limited to data collected within the period 1980–90.
Results
The life-time expectancy of stones in men and the effect of affluence
Data on the life-time expectancy of men in various countries forming at least one stone by the age of 70 years in relation to the annual Gross National Income (GNI) per capita in these countries are shown in Fig. 1. (The GNI per capita of a given country is based on the purchasing power parity rate of the GDP per capita in that country calculated in international dollars by the World Bank. This allows for differences in national prices and taxes and is a measure of the relative purchasing power of the per capita income in each country expressed in international dollars, where 1 international dollar = 1 US dollar in 1980). In this review therefore GNI per capita has been used in preference to GDP as a real measure of affluence, as it corrects for variability in purchasing power between countries.
Figure 1.
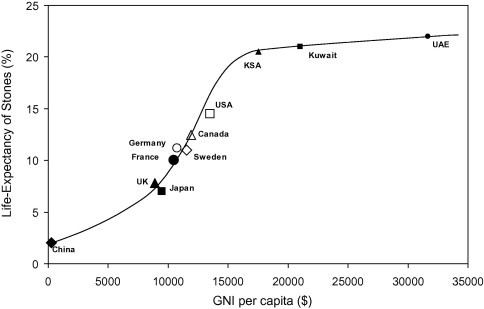
The relationship between the life-expectancy of a man forming at least one stone before the age of 60–70 years and the GNI per capita in US $ in various countries during the period 1980–90.
The data in Fig. 1 were extracted from numerous published sources and relate to the international economic situation between 1980 and 1990 [1,4,5,8–10,17]. The stone incidence data from China were reported before the recent rapid rise in industrialisation and in the GNI per capita of that country, and it is highly likely that urolithiasis is now much more common there than in the 1980s. Figure 1 shows, first, that the incidence of stone disease in a given country is almost linearly related to the level of affluence in the population up to an annual GNI per capita of ≈$16,000 (based on 1980–90 data), and then the relationship begins to flatten. Secondly, Fig. 1 shows that during that period urolithiasis was extremely common in all of the main oil-rich countries of the Gulf region. How does affluence affect the risk of forming stones?
Affluence and diet
Numerous studies have shown that locally, nationally and internationally the main dietary factor that is correlated with the level of affluence in the population is the consumption of animal protein, in particular the ‘meat + fish + poultry’ portion of animal protein [15,16,19–21]. Figure 2 shows an analysis of the major sources of protein in the diet. For stone disease no distinction is drawn between animal protein derived from meat, fish and poultry. In the case of cardiovascular disease there appears to be a difference in the relative influence of these sources of protein on the risk of developing the disorder, but for urolithiasis there appears to be no such difference.
Figure 2.
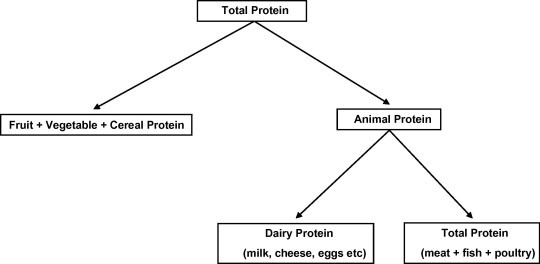
Diagram showing the various components of total protein in the diet.
Figure 3 shows the relationship between the daily per capita consumption of animal protein and the GNI per capita in the countries shown in Fig. 1. Once again, the oil-rich countries of the Middle East are at the top end of the range of countries studied, although the graph shows that the relationship again rises much more slowly as the annual GNI per capita increases above ≈$16,000.
Figure 3.
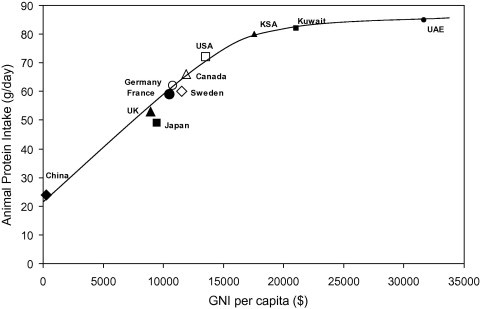
The relationship between the daily intake of animal protein per capita and the GNI per capita in US $ in various countries during the period 1980–90.
Combining the data from Figs. 1 and 3 into Fig. 4, this shows the predicted relationship between the life-time expectancy of men forming at least one stone in various countries and the daily per capita consumption of animal protein in these countries. The relationship appears to be linear up to a daily animal protein intake of ≈75 g/day. However, above this value the slope of the relationship increases sharply, suggesting that in the three Gulf States there might be other factors that are causing a further increase in the risk of forming CaOx- and/or UA-containing stones. What are these factors?
Figure 4.
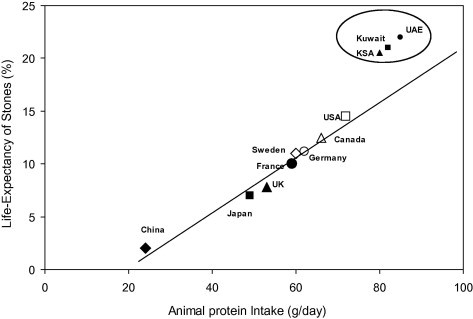
The predicted relationship between the life-expectancy of a man forming at least one stone before the age of 60–70 years and the daily intake of animal protein per capita in various countries, taken from the data in Figs 1 and 3.
Diet and urinary composition
Previous studies have shown that a high animal-protein diet per se adversely affects up to five of the seven main urinary risk factors for CaOx- and UA-stone formation [19–22]. Most of these studies have shown that this type of diet causes an increase in the urinary excretions of calcium and UA, and a decrease in urinary pH and in the urinary excretion of citrate. Some [19,20], but not all [21,22] reports have shown that it also increases the urinary excretion of oxalate. The possible causes of these changes in urinary composition are outlined in Table 2. Taken together, these changes would be anticipated to increase greatly the biochemical risk of forming both CaOx- and UA-containing stones [19–21]. Although Fig. 4 confirms this hypothesis, it also suggests that in the oil-rich Gulf States there must be other factors that account for the further sharp increase in the curve of stone incidence vs. animal protein consumption at high intake of animal protein.
Table 2.
Adverse effects of a high animal protein diet on the composition of urine.
| Causal factor | Metabolic effect | Effect on urine |
|---|---|---|
| ↑ Dietary acid (from sulphur-containing amino acids) | ↑ Urinary acid excretion | ↓ pH |
| ↑ Urinary acid excretion | ↑ Tubular reabsorption of citrate | ↓ Citrate |
| ↑ Urinary acid excretion | ↓ Tubular reabsorption of calcium | ↑ Calcium |
| ↑ Tyrosine, tryptophan, phenyl-alanine and hydroxyproline | ↑ Partial metabolism to oxalate | ↑ Oxalate |
| ↑ Dietary purine | ↑ Metabolism to uric acid | ↑ Uric acid |
In this connection, it has been shown that in KSA (and predictably also in Kuwait and the UAE) there are indeed other dietary factors that also increase the risk of forming stones [5,23]. First, the daily dietary intake of oxalate is about three times higher than in most Western countries, arising from the consumption of several high oxalate-containing foods particular to that part of the Middle East, as shown in Table 3. However, conversely the daily intake of calcium is only about half of that in the West. This means that the oxalate/calcium ratio in the intestine is about six times higher in the populations of the Gulf States than it is in populations in the West. Thus, more oxalate becomes available for absorption as calcium is absorbed from the gut contents in the small intestine. This in turn would be predicted to lead to a higher absorption of oxalate in the large bowel (where oxalate is known to be absorbed passively) and a much higher average urinary excretion of oxalate (i.e. a form of enteric hyperoxaluria). In confirmation of this hypothesis, the urinary oxalate data in Western and Middle Eastern men in the UAE and in KSA are compared in Fig. 5. Clearly, the urinary excretion of oxalate is considerably higher in the Middle Eastern men than in Western men. As an increase in urinary oxalate has been shown to be the second most important factor after a decrease in urine volume in increasing the risk of stone formation [24], these very high urinary excretions of oxalate would be predicted to produce a massive increase in the incidence of stones and might explain the divergence of the data in Fig. 4 in the oil-rich Gulf States.
Table 3.
Oxalate content of some foods popular in the Middle East.
| Foodstuff | Oxalate content (mmol/100 g) |
|---|---|
| Kusa (zucchini) | 0.05 |
| Kasbara (coriander leaves) | 0.10 |
| Jarjeer (watercress) | 0.10 |
| Kurath (leek-like) | 0.14 |
| Green peppers | 0.18 |
| Summer squash | 0.24 |
| Eggplant (aubergine) | 0.27 |
| Bagdunas (curly parsley) | 0.51 |
| Okra | 1.62 |
| Malooqia | 1.76 |
| Sabanaq (spinach-like) | 1.99 |
| Salaq | 3.43 |
| Spinach | 8.33 |
| Tea (without milk) | 0.14 |
| Chocolate (plain) | 1.30 |
| Peanuts | 2.08 |
| Pecans | 2.24 |
| Cashews | 3.53 |
Figure 5.
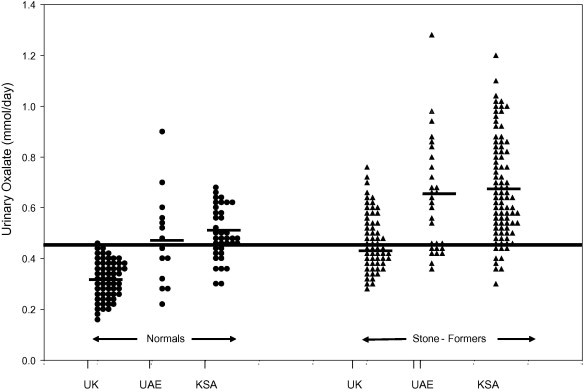
The 24-h urinary excretion of oxalate (in mmol/day) in normal men and in male stone-formers in the UK, KSA and the UAE. The black line is the upper limit of 24-h urinary excretion of oxalate in normal men in the UK.
However, there is a slight compensating factor that might help to partially modulate the marked effect on stone incidence that would be expected from these very high urinary excretions of oxalate by men in the Gulf States, as the low intake of calcium and the (perhaps surprisingly) low vitamin D status of Saudis [25,26] combine to cause them to have a relatively low intestinal absorption and urinary excretion of calcium. Fig. 6 shows the comparable data for urinary calcium excretion in the groups described in Fig. 5. From this it is clear that hypercalciuria is a relatively rare occurrence in the Middle East and certainly cannot be considered to be the main risk factor for stones in that part of the world. In passing, these data also cast considerable doubt on the now outdated hypothesis that hypercalciuria is the main risk factor for stones [27] but rather support the contention that it is only an ancillary factor for the disorder [24]. However, despite the relatively low urinary excretions of calcium found in the Middle East, the net effect of these changes in urinary composition is to increase the biochemical risk of forming CaOx-containing stones in the populations of the Gulf States (Fig. 7).
Figure 6.
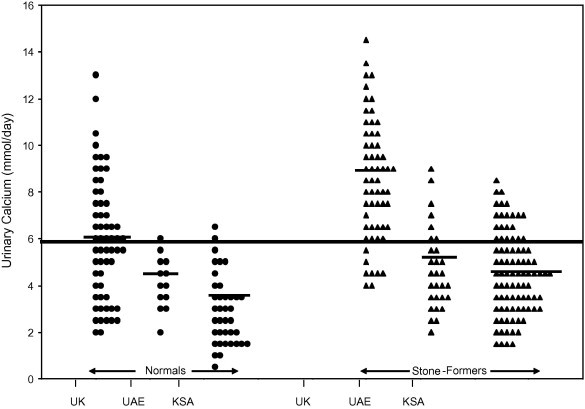
The 24-h urinary excretion of calcium (in mmol/day) in normal men and in male stone-formers in the UK, KSA and the UAE. The black line is the mean value of 24-h urinary excretion of calcium in normal men in the UK.
Figure 7.
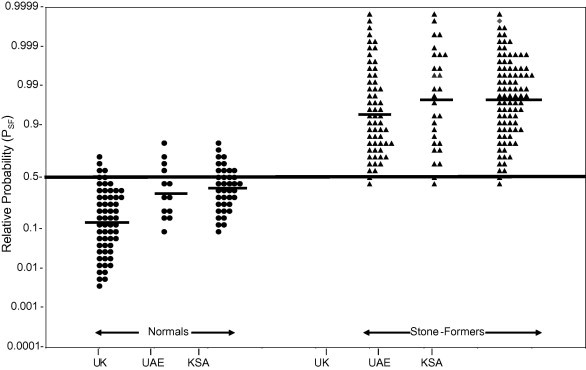
The PSF of forming CaOx- and/or UA-containing stones in normal men and in male stone-formers in the UK, KSA and the UAE, calculated from the data in Figs. 5 and 6. The black line is the 95% upper confidence limit of PSF in normal men in the UK.
There is one further urinary factor that would be predicted to increase the risk of forming all types of stone in the countries of the Gulf, and that is a low urine volume. Studies have shown that in the urban populations of the Gulf States average urine volume is slightly lower than in the West but it is not as low as might be expected from the hot, dry climate of the region [18]. This is probably because most urban communities in these countries live and work in air-conditioned environments and so the loss of fluid through sweating is not as high as might be anticipated from the high ambient outside temperature and low humidity. If it had been possible to carry out studies amongst the Bedouin tribes, who largely live in tents in the desert, the incidence of low urine volumes (<1 L/day) might have been much higher. Nevertheless, the tendency to a low urine volume observed in the urban populations of the oil-rich Gulf States will certainly increase the risk of forming both UA- and CaOx-containing stones and might also contribute to the divergence of the data from these countries, as shown in Fig. 4.
Urinary composition and biochemical risk of stone-formation
The net result of the socio-economic, environmental and dietary factors mentioned above will have a pronounced effect on the biochemical risk of forming both UA- and CaOx-containing stones in the populations of the Gulf States. The above studies have shown that Middle Eastern men from these countries have higher urinary excretions of oxalate and uric acid, lower urinary volumes and a lower urinary excretion of citrate, and pass more acidic urine than Western men [3,18]. Although they also have lower urinary excretions of calcium, the net effect of these changes is to produce a marked increase in the biochemical risk of forming both UA- and CaOx-containing stones (Fig. 7). The biochemical probabilities of forming stones (PSF) are calculated from data originally published in 1981 [3] and 1989 [18] using the urinary risk factors detailed above (i.e. a high or low urinary pH, a low urine volume, hypercalciuria, hyperoxaluria, hyperuricosuria, hypocitraturia and hypomagnesuria). The PSF values are calculated on a probability scale from 0 to 1 and show the highest value of PSF for the various stone types found in each individual. In most cases these were the PSF values for CaOx, UA or a mixture of these two stone constituents. PSF values of >0.5 are indicative of a significantly high risk of forming stones; values of >0.9 are generally found in urine from actively recurrent stone-formers who are not on any form of prophylactic treatment [24].
A summary of the dietary, environmental and urinary factors that lead to the high incidence of UA- and CaOx-containing stones in the affluent, oil-rich Gulf States is shown in Fig. 8.
Figure 8.
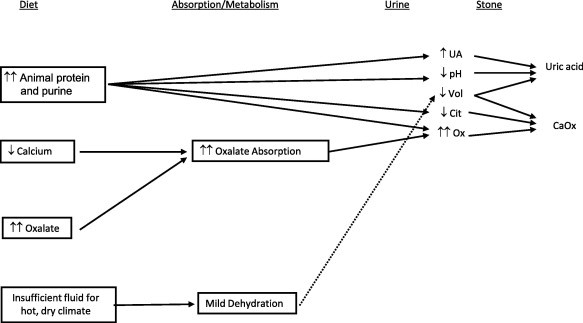
Summary of the dietary and urinary risk factors leading to a high incidence of UA- and CaOx-containing stones in the affluent, oil-rich countries of the Gulf.
Discussion and conclusions
The high incidence of UA- and CaOx-containing stones in the oil-rich countries of the Gulf observed in the 1980s is due to a combination of several socio-economic, environmental and nutritional factors, and the interrelationships between these factors. These include: (i) the level of affluence in the population and the effect that this has on the consumption of animal protein; (ii) other local dietary habits such as the high intake of oxalate-containing foods and the low intake of calcium-containing foods; and (iii) the hot, dry climate of the region and its effect on urine volume. It might be that some of these factors will have changed in the past 20–30 years, as the GNI per capita of some of these countries (particularly that of Kuwait) has increased markedly during that time [17]. Dietary and lifestyle practices might also have changed. However, personal experience over the past 15 years of screening Middle Eastern men from the Gulf States who come to London for their stone management suggests that the dietary and urinary abnormalities discovered in the 1980s still persist in the present.
Conflict of interest
No conflict of interest to declare.
Footnotes
Peer review under responsibility of Arab Association of Urology.

References
- 1.Robertson W.G. The scientific basis of urinary stone-formation. In: Mundy A.R., Fitzpatrick J.M., Neal D.E., George N.J.R., editors. Scientific Basis of Urology. 3rd ed. Informa UK Ltd.; Colchester: 2010. pp. 162–181. [Google Scholar]
- 2.Robertson W.G., Peacock M., Hodgkinson A. The effect of dietary changes on the incidence of urinary calculi in the UK between 1958 and 1976. J Chronic Dis. 1979;32:469–476. doi: 10.1016/0021-9681(79)90107-3. [DOI] [PubMed] [Google Scholar]
- 3.Al-Ali I.H., Husain I., Robertson W.G., Ouimet E., Waheed S.A. Metabolic aspects of calcium oxalate urolithiasis and the effect of allopurinol. Emirates Med J. 1981;3:292–299. [Google Scholar]
- 4.El-Reshaid K., Mughal H., Kapoor M. Epidemiological profile, mineral metabolic pattern and crystallographic analysis of urolithiasis in Kuwait. Eur J Epidemiol. 1997;13:229–234. doi: 10.1023/a:1007346727944. [DOI] [PubMed] [Google Scholar]
- 5.Robertson W.G., Hughes H. Epidemiology of urinary stone disease in Saudi Arabia. In: Ryall R., Bais R., Marshall V.R., Rofe A.M., Smith L.H., Walker V.R., editors. Urolithiasis 2. Plenum Press; New York and London: 1994. pp. 453–455. [Google Scholar]
- 6.Barkworth S.A., Louis S., Walker V.R., Hughes H., Robertson W.G. Stone type and urine composition in the Middle East with particular reference to Saudi Arabia. In: Walker V.R., Sutton R.A.L., Cameron E.C.B., Pak C.Y.C., Robertson W.G., editors. Urolithiasis. Plenum Press; New York and London: 1989. p. 715. [Google Scholar]
- 7.Abomelha M.S., Al-Khader A.A., Arnold J. Urolithiasis in Saudi Arabia. Urology. 1990;35:31–34. doi: 10.1016/0090-4295(90)80008-b. [DOI] [PubMed] [Google Scholar]
- 8.Abdul-Halim R.E. Urolithiasis in adults. Saudi Med J. 2005;26:705–713. [PubMed] [Google Scholar]
- 9.Al-Hunayan A., Abdul-Halim H., Kehinde E.O., Al-Awadi K., El Barky E., Al-Ateequi A. Mode of presentation and first line of management of non-recurrent urolithiasis in Kuwait. Int J Urol. 2004;11:963–968. doi: 10.1111/j.1442-2042.2004.00934.x. [DOI] [PubMed] [Google Scholar]
- 10.Husain I., Badsha S.A., Al-Ali I.H., Walton M., Sahab A., Jafree S. A survey of urinary stone disease in Abu Dhabi. Emirates Med J. 1979;1(Suppl.):17–33. [Google Scholar]
- 11.Organization for Economic Cooperation and Development. Food consumption statistics, Paris: OECD; 1975, 1–301.
- 12.Food and Agriculture Organization. Analysis of food consumption survey data for developing countries. FAO and Agricultural Organization of the United Nations, Rome: OECD 1980, 1–139. [PubMed]
- 13.Food and Agriculture Organization. Bibliography of food consumption surveys. FAO and Agricultural Organization of the United Nations, Rome: OECD 1981, 1–85.
- 14.Abelow B.J., Holford T.R., Insogna K.L. Cross–cultural association between dietary animal protein and hip fracture: a hypothesis. Calcif Tissue Int. 1992;50:14–18. doi: 10.1007/BF00297291. [DOI] [PubMed] [Google Scholar]
- 15.Robertson W.G., Peacock M., Heyburn P.J., Hanes F.A., Swaminathan R. The risk of calcium stone-formation in relation to affluence and dietary animal protein. In: Brockis J.G., Finlayson B., editors. Urinary calculus. PSG Publishing; Littleton, Mass: 1981. pp. 3–12. [Google Scholar]
- 16.Speedy A.W. Global production and consumption of animal source foods. J Nutr. 2003;133:4048S–4053S. doi: 10.1093/jn/133.11.4048S. [DOI] [PubMed] [Google Scholar]
- 17.World Bank Development Indicators. Washington: World Bank; 2012: 20.
- 18.Robertson W.G., Qunibi W., Husain I., Hughes, Walker V.R., Taher S. The calculation of stone risk in the urine of Middle Eastern men and Western expatriates living in Saudi Arabia. In: Walker V.R., Sutton R.A.L., Cameron E.C.B., Pak C.Y.C., Robertson W.G., editors. Urolithiasis. Plenum Press; New York and London: 1989. pp. 669–671. [Google Scholar]
- 19.Robertson W.G., Heyburn P.J., Peacock M., Hanes F., Swaminathan R. The effect of a high animal protein intake on the risk of calcium stone-formation in the urinary tract. Clin Sci. 1979;57:285–288. doi: 10.1042/cs0570285. [DOI] [PubMed] [Google Scholar]
- 20.Robertson W.G., Peacock M., Heyburn P.J., Hanes F., Rutherford A., Clementson E. Should recurrent, calcium-containing stone-formers become vegetarians? Br J Urol. 1979;51:427–431. doi: 10.1111/j.1464-410x.1979.tb03570.x. [DOI] [PubMed] [Google Scholar]
- 21.Breslau N.A., Brinkley L., Hill K.D., Pak C.Y. Relationship of animal protein-rich diet to kidney stone formation and calcium metabolism. J Clin Endocrinol Metab. 1988;66:140–146. doi: 10.1210/jcem-66-1-140. [DOI] [PubMed] [Google Scholar]
- 22.Marangella M., Bianco O., Martin I.C., Petrarulo M., Vitale C., Linari F. Effect of animal and vegetable protein intake on oxalate excretion in idiopathic calcium stone disease. Br J Urol. 1989;63:348–351. doi: 10.1111/j.1464-410x.1989.tb05214.x. [DOI] [PubMed] [Google Scholar]
- 23.Robertson W.G., Nisa M., Husain I., Al-Faqih S., Chakrabarty A., Quinibi W. The importance of diet in the aetiology of primary calcium and uric acid stone-formation: The Arabian experience. In: Sutton R.A.L., Cameron E.C.B., Pak C.Y.C., Robertson W.G., Walker V.R., editors. Urolithiasis. Plenum Press; New York and. London: 1989. pp. 735–739. [Google Scholar]
- 24.Robertson W.G. A risk factor model of stone-formation. Front Biosci. 2003;8:1330–1338. doi: 10.2741/1181. [DOI] [PubMed] [Google Scholar]
- 25.Sedrani S.H. Low 25-hydroxyvitamin D and normal serum calcium concentrations in Saudi Arabia: Riyadh region. Ann Nutr Metab. 1984;28:181–185. doi: 10.1159/000176801. [DOI] [PubMed] [Google Scholar]
- 26.Sadat-Ali M., Al-Elq A., Al-Turki H., Al-Mulhim F., Al-Ali A. Vitamin D levels in healthy men in eastern Saudi Arabia. Ann Saudi Med. 2009;29:378–382. doi: 10.4103/0256-4947.55168. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Coe F.L., Kavalach A.G. Hypercalciuria and hyperuricosuria in patients with calcium nephrolithiasis. N Engl J Med. 1974;291:1344–1350. doi: 10.1056/NEJM197412192912510. [DOI] [PubMed] [Google Scholar]