

Abstract
A 27-year-old female patient presented with a slight scaly, crusting, erythematous patch close to the right nipple 10 years ago. When her symptoms failed to respond to topical therapy 3 months later, nipple biopsy was performed and revealed Paget’s disease of the breast. The patient underwent unilateral mastectomies with sentinel lymph node biopsy. She has stayed healthy and has had no evidence of breast cancer recurrence since surgery.
Keywords: Paget’s disease, nipple, breast cancer
Introduction
Paget’s disease of the breast is a rare presentation of breast cancer and most commonly is identified in the setting of a scaly erythematous nipple or an erythematous patch near the nipple, often referred to as an eczematous rash. Nipple pruritus may also be a manifestation of Paget’s disease [1]. Often when women present for evaluation of nipple itching in the setting of a normal appearing nipple, the possibility of Paget’s disease is overlooked. Women presenting with such changes are frequently diagnosed as dermatitis or eczema and treated with topical regimens with the true diagnosis remaining elusive for long periods of time [2,3].
To avoid missing a diagnosis of Paget’s disease of the breast, the clinicians must maintain a high level of clinical suspicion. The case we present is unusual in that the patient was 27 years of age without any significant breast cancer risk factors and the presenting symptoms were nipple pruritus and eczematous rash. Failure to respond to topical treatment and the clinician’s investigation with a nipple biopsy intended to exclude the diagnosis of breast cancer revealed the unsuspected diagnosis of Paget’s disease of the breast.
Case presentation
A 27-year-old female presented with a scaly, erythematous patch near the right nipple, accompanied by crusting and pruritus. When the pruritus persisted for 3 months, she visited her primary physician who prescribed a topical medication and suggested that she might be developing eczema. The pruritus failed to resolve and she returned for further evaluation. She was referred to a local surgeon. The doctor felt that the likelihood of Paget’s disease was very low given her age and lack of suggestive skin findings, but recommended a biopsy of the nipple to exclude the possibility. However, nipple biopsy confirmed the unlikely diagnosis of Paget’s disease of the breast. No individual or familiar risk factors were known.
Clinical examination revealed a healthy-appearing young woman. Inspection of the breasts identified a 2-cm round, slight scaly, crusting, erythematous patch close to the right nipple (Figure 1) without other skin findings. Specifically, no papular or ulcerations lesions were present. There was not any palpable mass in the underlying breast parenchyma or any axillary lymph node enlargement. There were also no sonographic findings of concern in the subareolar or upper outer breast. Bilateral breast MRI was then performed and no focal abnormalities concerning for malignancy were identified.
Figure 1.

Scaly, crusting, erythematous patch of the affected nipple.
The histopathological examination showed epidermal cells with hyperchromatic and polymorphic nuclei, intraepithelial gland cells (Figure 2A). Immunohistochemical tests showed that the tumor cells were positive for cytokeratin 7 (CK7), epithelial membrane antigen (EMA), and C-erbB2. The cytoplasm of the tumor cells was positive for D-PAS staining (Figure 2B). The tumor cells were negative for S-100, HMB-45, and Melan-A staining (not shown).
Figure 2.
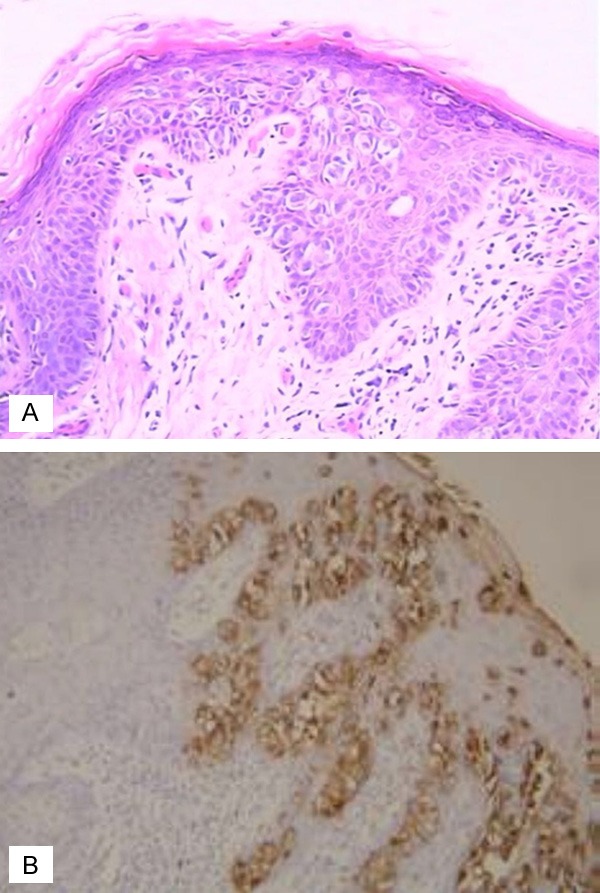
Histologic and immunohistochemical appearance of a surgical tissue specimen from the affected nipple. A: The epidermal cells with hyperchromatic and polymorphic nuclei, intraepithelial gland cells (HE×200); B: The tumor cells were positive for immunohistochemical staining (SP×200).
After further discussion and consideration of treatment options, the patient elected to proceed with right skin-sparing mastectomies with implant reconstruction.
Final surgical pathology of the right mastectomy specimen demonstrated the Paget’s disease of the breast, which was consistent with the original pathologic diagnosis. No angiolymphatic invasion was identified. Sentinel lymph node biopsy was negative for axillary nodal involvement. In addition, a single right intramammary lymph node was negative for tumor involvement. The patient recovered well after surgery. The patient was then seen for regular oncologic follow-up and continues to have no evidence of recurrent breast cancer.
Discussion
Paget’s disease of the breast is a rare malignant condition with a reported incidence among all primary breast cancers of 1-3% [2-4]. Underlying carcinoma is identified in the majority of cases but may be absent in up to 33% of cases [5]. It is extremely uncommon in young women. The presenting age ranges from 24 to 84 years with a mean age at diagnosis being 55 years [6]. This is one of the few reports in the literature of a woman presenting at a young age with Paget’s disease of the breast, and this patient represents the third youngest such woman. To our knowledge, there are only two other reports of very young women diagnosed with Paget’s disease of the breast [7,8].
Despite description well over 100 years ago and a generally widely recognized typical clinical presentation, it remains relatively common for women presenting with classic clinical findings of Paget’s disease of the breast to be misdiagnosed with either eczema or dermatitis. Often such patients are treated with topical steroids with no improvement and may elude accurate diagnosis for months or longer. Thus, women presenting with non-classical clinical indicators of Paget’s disease may remain undiagnosed for extended periods of time resulting in more locally or loco-regionally advanced disease at diagnosis.
The prognosis of Paget’s depends on the presence of an invasive cancer and axillary lymph node spread. In Paget’s disease, there is no underlying breast malignancy or lymph node spread and the five-year survival is 92-94% [6,9]. Hence, Early and accurate diagnosis of Paget’s disease by means of cytology enables organ conserving surgery, especially when the lesion is confined to the epidermis of nipple [1,2]. While our patient presented with an erythematous patch near the nipple, she did not have any of the classic dermatologic changes associated with Paget’s disease of the breast. This case underlines how important histological examinations even in unusual clinical pictures are.
Disclosure of conflict of interest
None.
References
- 1.Sakorafas GH, Blanchard K, Sarr MG, Farley DR. Paget’s disease of the breast. Cancer Treat Rev. 2001;27:9–18. doi: 10.1053/ctrv.2000.0203. [DOI] [PubMed] [Google Scholar]
- 2.Chaudary MA, Millis RR, Lane EB, Miller NA. Paget’s disease of the nipple: a ten year review including clinical, pathological, and immunohistochemical findings. Breast Cancer Res Treat. 1986;8:139–146. doi: 10.1007/BF01807702. [DOI] [PubMed] [Google Scholar]
- 3.Dixon AR, Galea MH, Ellis IO, Elston CW, Blamey RW. Paget’s disease of the nipple. Br J Surg. 1991;78:722–723. doi: 10.1002/bjs.1800780627. [DOI] [PubMed] [Google Scholar]
- 4.Caliskan M, Gatti G, Sosnovskikh I, Rotmensz N, Botteri E, Musmeci S, Rosali-Dos SG, Viale G, Luini A. Paget’s disease of the breast: the experience of the European institute of oncology and review of the literature. Breast Cancer Res Treat. 2008;112:513–521. doi: 10.1007/s10549-007-9880-5. [DOI] [PubMed] [Google Scholar]
- 5.Kothari AS, Beechey-Newman N, Hamed H, Fentiman IS, D’Arrigo C, Hanby AM, Ryder K. Paget’s disease of the nipple: a multifocal manifestation of higher-risk disease. Cancer. 2002;95:1–7. doi: 10.1002/cncr.10638. [DOI] [PubMed] [Google Scholar]
- 6.Siponen E, Hukkinen K, Heikkil P, Joensuu H, Leidenius M. Surgical treatment in Paget’s disease of the breast. Am J Surg. 2010;200:241–246. doi: 10.1016/j.amjsurg.2009.07.044. [DOI] [PubMed] [Google Scholar]
- 7.Nicole PS, Harry JL, Kiley JJ, Amy CD. An unusual presentation of breast cancer in a very young woman. BMJ Case Rep. 2011;102:137–142. doi: 10.1136/bcr.12.2010.3590. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Singla V, Virmani V, Nahar U, Singh G, Khandelwal NK. Paget’s disease of breast masquerading as chronic benign eczema. Indian J Cancer. 2009;46:344–7. doi: 10.4103/0019-509X.55560. [DOI] [PubMed] [Google Scholar]
- 9.Alexandre MM, Eduardo M, José RF, Rolf G. Immediate nipple-areola-sparing mastectomy reconstruction: An update on oncological and reconstruction techniques. World J Clin Oncol. 2014;5:478–494. doi: 10.5306/wjco.v5.i3.478. [DOI] [PMC free article] [PubMed] [Google Scholar]