

Abstract
Background:
Movement disorders after the clipping for an unruptured giant aneurysm are rare. The information on the pathogenesis and treatment options for this condition is largely unknown.
Case Description:
An 82-year-old female with no neurological deficits underwent a clipping for a giant middle cerebral artery (MCA) aneurysm. Immediately after surgery, she presented with hemichorea–hemiballismus (HC–HB) on the left side. Postoperative angiograms and single-photon emission computed tomography demonstrated the hyperperfusion in the right frontal cortex and the decreased perfusion in the basal ganglia, indicating that the abrupt hemodynamic changes due to the obliteration of the giant aneurysm caused the dysfunction of the frontal cortical and subcortical pathway and the basal ganglia. Administration of tiapride hydrochloride was dramatically effective in controlling the HC–HB until the hyperperfusion resolved. Single-photon emission computed tomography obtained 8 weeks after surgery revealed that the cerebral blood flow had been normalized in the right frontal cortex. The relative hypoperfusion of the right basal ganglia was also resolved. Then tiapride hydrochloride was discontinued without a relapse of HC–HB.
Conclusion:
This case appears consistent with the theory that the connecting fibers responsible for the development of HC–HB are also located in the frontal lobe. The treatment of giant aneurysms involving the M1 portion can cause abrupt hemodynamic changes in both frontal cortex and the basal ganglia, which can potentially induce postoperative movement disorders.
Keywords: Aneurysm, chorea, clipping, giant aneurysm, hyperperfusion, single-photon emission computed tomography
INTRODUCTION
Movement disorders can occur as secondary to a variety of neurological, metabolic, infectious, traumatic, and other systemic diseases.[20,24] Cerebrovascular events account for approximately 22% of these secondary movement disorders.[24] A large series study reported that chorea was the most common movement disorder (35.7%).[2] Hemichorea–hemiballismus (HC–HB) has been observed in patients with hemodynamic insufficiency caused by moyamoya disease,[10,13,14,16,21,25,29,30,32,33,38,40,41] intracranial arterial stenosis,[15,17] and extracranial carotid artery stenosis.[8,22,27] The basal ganglia, particularly the lentiform nucleus and the thalamus, has traditionally been deemed responsible for HC–HB.[2,3,5,9,20] However, recent studies investigating the distribution of hemodynamic insufficiency using single-photon computed tomography (SPECT) demonstrated that the frontal cortical subcortical motor pathway also plays a significant role in the development of HC–HB.[14,22]
Here we report a case of HC–HB on the left side of the body that started immediately after clipping of a right unruptured giant middle cerebral artery (MCA) aneurysm at the M1 portion. This patient had no hemorrhage or infarct appreciable on postoperative magnetic resonance (MR) images. However, SPECT showed some degree of postoperative hyperperfusion in the right frontal lobe as well as the hypoperfusion of the right basal ganglia. These hemodynamic changes resolved 8 weeks after surgery with remission of HC–HB. Our findings indicated that hyperperfusion as well as hypoperfusion can induce contralateral HC–HB and substantiated the previous theory that dysfunction of the frontal cortical subcortical motor pathway is one of the possible mechanisms of HC–HB. The treatment of giant aneurysms involving the M1 portion might be at an increased risk of postoperative movement disorder because it can potentially cause abrupt hemodynamic changes in both frontal cortex and the basal ganglia.
CASE REPORT
An 82-year-old female was referred to our hospital with a 1-month history of pulsatile headache. A head computed tomography (CT) scan taken at the previous hospital showed a 2.5-cm sized mass in the right temporal region. MR imaging demonstrated a round and partially thrombosed aneurysm of the MCA [Figure 1a]. After thoroughly discussing treatment options and risks with the patient and her family, they decided to continue to watch the aneurysm. We scheduled a follow-up visit in 6 months, but this was not accomplished because the patient felt she was stable. When she revisited our hospital for worsening headache 2 years after her last visit, the aneurysm had grown in size from 2.5 to 4.0 cm, with the development of a significant perifocal edema [Figure 1b]. She had no neurological deficits. We recommended that she undergo clipping of the aneurysm, and she agreed to our proposal. We performed a right frontotemporal craniotomy through the orbitozygomatic approach, with intraoperative monitoring of the motor-evoked potential. The aneurysm was buried in the temporal lobe [Figure 1c]. Dissecting the sylvian fissure, we found the aneurysm had arisen from the nonbranching portion of the M1, not M1–M2 bifurcation. First, we anastomosed the right superficial temporal artery (STA) to the temporal cortical branch of the MCA to secure distal blood flow during the temporary occlusion of M1. After confirming patency of the anastomosis and the distribution of bypass flow, we trapped the M1 using temporary clips. Next, we sectioned the aneurysm and completely removed the clots. Two clips were then applied in an angioplastic fashion [Figure 1d]. A good patency was confirmed using Doppler flowmetry and indocyanine green fluorescence angiography. The patient showed a good arousal from anesthesia, but presented a few hours after surgery with an irregular, purposeless, and hyperkinetic movement in the left arm and leg, which she was still able to move voluntarily (see Supplementary Video). Postoperative CT scan obtained immediately after surgery revealed no abnormal findings. MR images obtained 1 day after surgery did not reveal any new hemorrhage or infarction [Figure 2a–c]. We diagnosed her abnormal movement as HC–HB. Angiography delineated a complete obliteration of the aneurysm with no other occluded arteries. However, the arterial flow in the peripheral MCA territory obviously increased, compared with preoperative findings [Figure 2d and e]. Although STA–MCA bypass flow was also confirmed, the flow via the bypass was only toward the distal portion of the cortical temporal artery [Figure 2f]. The 99mTc-ECD SPECT obtained 3 days after surgery demonstrated hyperperfusion of the MCA territory [Figure 3a]. There was slight hypoperfusion in the right basal ganglia including the subthalamic regions. Cerebral blood flow (CBF) was decreased in the lateral insular cortex, but the area of hypoperfusion corresponded to that of the perifocal edema existing before surgery. We suspected that the patient's HC–HB may be related to the hyperperfusion in the right frontal cortex in addition to the decreased perfusion in the right thalamic region. Although her neurological findings were otherwise normal, HC–HB persisted without any improvement for the following week, irrespective of our attempt to maintain her systolic blood pressure under 130 mmHg. We next tried tiapride hydrochloride, 75 mg twice a day, which dramatically relieved her symptoms. The patient was discharged with no neurological deficit. SPECT obtained 8 weeks after surgery revealed that CBF had been normalized in the right frontal cortex with the resolved laterality of the perfusion in the thalamic regions [Figure 3b]. The semiquantitative data calculated by the Patlak plot method demonstrated the normalization of regional CBF in the right frontal lobe and the resolution of the disparity in the bilateral subthalamic nuclei [Table 1]. At that point, the tiapride hydrochloride was discontinued without a relapse of HC–HB.
Figure 1.
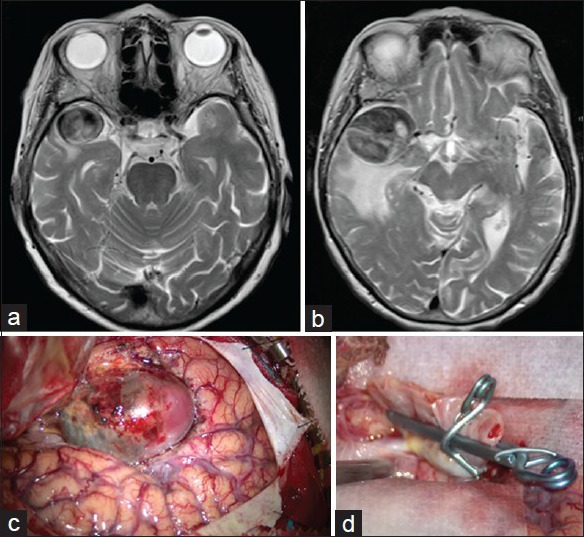
(a and b) Axial T2-weighted MR images showing an increase of the right middle cerebral artery aneurysm diameter from 2.5 to 4 cm in 2 years. (c) Intraoperative photograph of the aneurysm. (d) The aneurysm was clipped using two clips
Figure 2.
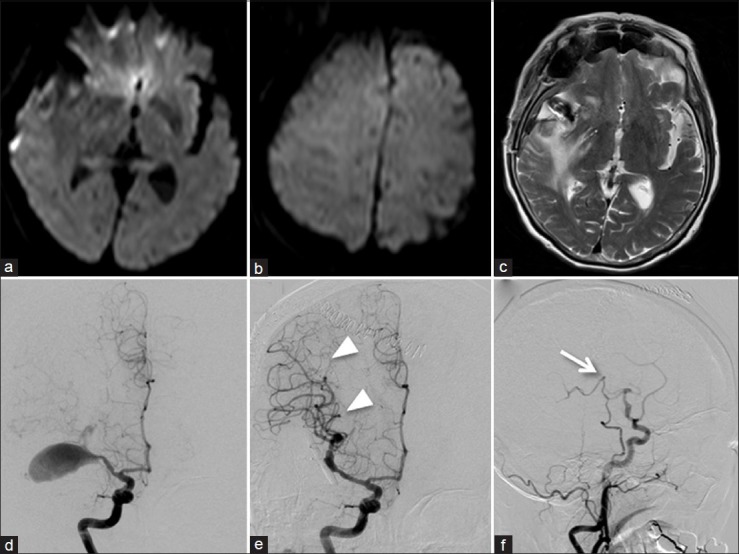
(a and b) Axial diffusion-weighted MR images obtained 1 day after surgery revealing no acute ischemia. (c) Axial T2-weighted MR image performed 1 day after surgery showing no new changes other than the preexisting edema around the aneurysm. (d) Preoperative angiogram demonstrating a giant MCA aneurysm. (e) Postoperative angiogram showing the complete obliteration of the aneurysm with preservation of the parent artery. Note the remarkable increase of the arterial flow in the MCA territory (arrowheads). (f) Right lateral carotid angiogram demonstrating that the bypass flow covered only a small area of the frontal lobe distal to the site of anastomosis (arrow)
Figure 3.
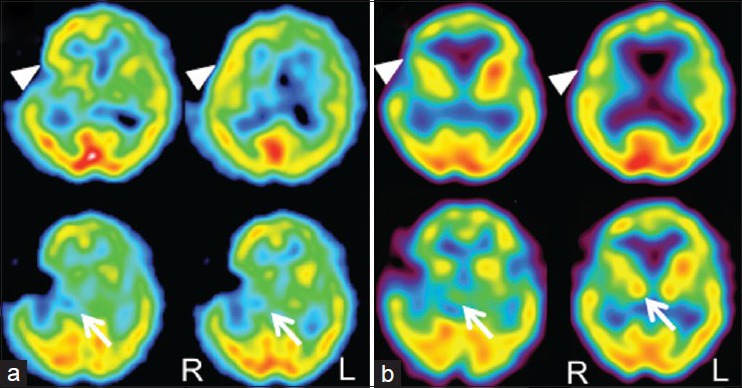
(a) 99mTc-ECD SPECT performed 3 days after surgery revealing hyperperfusion in the frontal cortex (arrowheads). There was also slight hypoperfusion in the right basal ganglia including the subthalamic nucleus (arrows). (b) 99mTc-ECD SPECT obtained 8 weeks after surgery showed the resolution of hyperperfusion in the right frontal cortex (arrowheads) with the resolved laterality of the perfusion in the subthalamic regions (arrows)
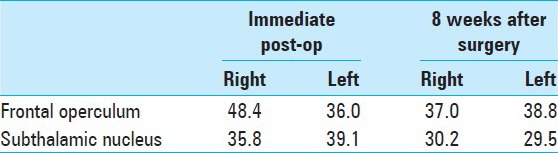
Table 1.
Cerebral blood flow calculated by the Patlak plot method (ml/100 g/min)
DISCUSSION
HC–HB can occur as a sequela to a variety of strokes.[4,20,24] Stroke types associated with HC–HB include cerebral infarction,[11,26,28,36] moyamoya disease,[10,13,14,16,21,25,29,30,32,33,38,40,41] intracranial arterial stenosis due to atherosclerotic change,[14,15] delayed vasospasm after subarachnoid hemorrhage,[31] extracranial carotid artery stenosis,[8,22,27] and cerebral hemorrhage.[2,18] Traditionally, the mechanism underlying poststroke HC–HB is believed to be ischemia of the basal ganglia, particularly the lentiform nucleus and the thalamus.[2,3,5,9,20] However, previous literature also shows that HC–HB can be caused by subcortical ischemia, without involvement of the basal ganglia.[1,7] In addition, recent studies examining CBF show that the frontal cortical and subcortical motor pathway may also play a significant role in the development of HC–HB.[14] Morigaki et al. also reported two cases of HC–HB that subsided after revascularization.[22] Their study proposes that the disrupted hemodynamics in the watershed areas of the frontal lobe account for the onset of hemichorea associated with carotid artery occlusive disease. In our case, the findings from postoperative angiography and SPECT demonstrated hyperperfusion, not hypoperfusion, in the frontal lobe immediately following surgery. It is well known that hyperperfusion can cause a variety of neurological deficits following STA–MCA anastomosis,[6,12,39] carotid endarterectomy (CEA),[37] obliteration of arteriovenous malformation,[34] and clipping of giant aneurysms.[19,23,35] We presume that abrupt elimination of the giant aneurysm from the M1 segment, which had long served as a buffering reservoir, may have led to a massively increased blood flow in the cortical MCA territory, resulting in dysfunction of the frontal cortical and subcortical motor pathways. It is unlikely that the STA–MCA bypass caused the hyperperfusion in our case because bypass flow covered only a small area of the frontal lobe distal to the site of anastomosis. We also speculate that the slight decreased perfusion in the right basal ganglia, although it was less prominent than the change in the frontal cortex, might have exacerbated the dysfunction of the frontal cortical and subcortical motor pathways. This hypoperfusion in the basal ganglia might be due to the flow reduction of the perforators caused by clipping of the giant M1 aneurysm with a wide neck. The development of HC-HB in this case could have a bearing on the morphological and anatomical characteristics of a giant M1 aneurysm mentioned above.
In summary, we encountered a case of HC–HB that developed immediately after clipping of a giant unruptured MCA aneurysm. Postoperative angiography and SPECT indicated that hyperperfusion in the frontal cortex and hypoperfusion in the basal ganglia appeared to provoke this hyperkinetic movement disorder. Administration of tiapride hydrochloride was effective in controlling the HC–HB until the hyperperfusion resolved. This study also supports the recent theory that the connecting fibers in the frontal cortical and subcortical motor pathway play a significant role in the development of HC–HB.
Video available on: www.surgicalneurologyint.com
Footnotes
Available FREE in open access from: http://www.surgicalneurologyint.com/text.asp?2015/6/1/84/157444
Contributor Information
Soichi Oya, Email: sooya-tky@umin.ac.jp.
Naoaki Fujisawa, Email: naoaki@saitama-med.ac.jp.
Toru Matsui, Email: matsui@saitama-med.ac.jp.
REFERENCES
- 1.Alakandy LM, Iyer RV, Golash A. Hemichorea, an unusual complication of ventriculoperitoneal shunt. J Clin Neurosci. 2008;15:599–601. doi: 10.1016/j.jocn.2006.12.016. [DOI] [PubMed] [Google Scholar]
- 2.Alarcón F, Zijlmans JC, Dueñas G, Cevallos N. Post-stroke movement disorders: Report of 56 patients. J Neurol Neurosurg Psychiatr. 2004;75:1568–74. doi: 10.1136/jnnp.2003.011874. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Béot Y, Giroud M, Moreau T, Benatru I. Clinical spectrum of movement disorders after stroke in childhood and adulthood. Eur Neurol. 2011;68:59–64. doi: 10.1159/000336740. [DOI] [PubMed] [Google Scholar]
- 4.Cardoso F, Seppi K, Mair KJ, Wenning GK, Poewe WW. Seminar on choreas. Lancet Neurol. 2006;5:14–14. doi: 10.1016/S1474-4422(06)70494-X. [DOI] [PubMed] [Google Scholar]
- 5.Chung SJ, Im JH, Lee MC, Kim JS. Hemichorea after stroke: Clinical-radiological correlation. J Neurol. 2004;251:725–9. doi: 10.1007/s00415-004-0412-5. [DOI] [PubMed] [Google Scholar]
- 6.Fujimura M, Mugikura S, Kaneta T, Shimizu H, Tominaga T. Incidence and risk factors for symptomatic cerebral hyperperfusion after superficial temporal artery-middle cerebral artery anastomosis in patients with moyamoya disease. Surg Neurol. 2009;71:442–7. doi: 10.1016/j.surneu.2008.02.031. [DOI] [PubMed] [Google Scholar]
- 7.Fukui T, Hasegawa Y, Seriyama S, Takeuchi T, Sugita K, Tsukagoshi H. Hemiballism-hemichorea induced by subcortical ischemia. Can J Neurol Sci. 1993;20:324–8. [PubMed] [Google Scholar]
- 8.Galea I, Norwood F, Phillips MJ, Shearman C, McMonagle P, Gibb WR. Pearls and Oysters: Resolution of hemichorea following endarterectomy for severe carotid stenosis. Neurology. 2008;71:e80–2. doi: 10.1212/01.wnl.0000336975.80810.74. [DOI] [PubMed] [Google Scholar]
- 9.Ghika-Schmid F, Ghika J, Regli F, Bogousslavsky J. Hyperkinetic movement disorders during and after acute stroke: The Lausanne Stroke Registry. J Neurol Sci. 1997;146:109–16. doi: 10.1016/s0022-510x(96)00290-0. [DOI] [PubMed] [Google Scholar]
- 10.Han SH, Kim YG, Cha SH, Chung SY. Moyamoya disease presenting with singing induced chorea. J Neurol Neurosurg Psychiatr. 2000;69:833–4. doi: 10.1136/jnnp.69.6.833. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Hara Y, Hashimoto Y, Terasaki T, Yamashita S, Uchino M. Cerebral embolism with hemiballism due to putaminal lesion. Rinsho Shinkeigaku. 1998;38:138–41. [PubMed] [Google Scholar]
- 12.Hayashi K, Horie N, Suyama K, Nagata I. Incidence and clinical features of symptomatic cerebral hyperperfusion syndrome after vascular reconstruction. World Neurosurg. 2012;78:447–54. doi: 10.1016/j.wneu.2011.10.041. [DOI] [PubMed] [Google Scholar]
- 13.Hong YH, Ahn TB, Oh CW, Jeon BS. Hemichorea as an initial manifestation of moyamoya disease: Reversible striatal hypoperfusion demonstrated on single photon emission computed tomography. Mov Disord. 2002;17:1380–3. doi: 10.1002/mds.10245. [DOI] [PubMed] [Google Scholar]
- 14.Im SH, Oh CW, Kwon OK, Cho BK, Chung YS, Han DH. Involuntary movement induced by cerebral ischemia: Pathogenesis and surgical outcome. J Neurosurg. 2004;100:877–82. doi: 10.3171/jns.2004.100.5.0877. [DOI] [PubMed] [Google Scholar]
- 15.Irioka T, Ayabe J, Mizusawa H. Hemichorea improved by extracranial-intracranial bypass surgery for middle cerebral artery occlusion. J Neurol. 2010;257:1756–8. doi: 10.1007/s00415-010-5596-2. [DOI] [PubMed] [Google Scholar]
- 16.Kamijo K, Matsui T. Dramatic disappearance of moyamoya disease-induced chorea after indirect bypass surgery. Neurol Med Chir (Tokyo) 2008;48:390–3. doi: 10.2176/nmc.48.390. [DOI] [PubMed] [Google Scholar]
- 17.Kim JM, Kim JS, Cho AH, Jeon SB, Lee DK, Suh DC, et al. Angioplasty of middle cerebral artery stenosis improves recurrent hemichorea caused by basal ganglia hypoperfusion. J Stroke Cerebrovasc Dis. 2006;15:69–71. doi: 10.1016/j.jstrokecerebrovasdis.2005.12.002. [DOI] [PubMed] [Google Scholar]
- 18.Larrosa D, Ramón C, Santamarta E, Zeidan N, Pascual J. Hemichorea secondary to contralateral pontine haemorrhage. Parkinsonism Relat Disord. 2013;19:271–2. doi: 10.1016/j.parkreldis.2012.06.016. [DOI] [PubMed] [Google Scholar]
- 19.Maruya J, Nishimaki K, Minakawa T. Hyperperfusion syndrome after neck clipping of a ruptured aneurysm on a dolichoectatic middle cerebral artery. J Stroke Cerebrovasc Dis. 2011;20:260–3. doi: 10.1016/j.jstrokecerebrovasdis.2009.11.014. [DOI] [PubMed] [Google Scholar]
- 20.Mehanna R, Jankovic J. Movement disorders in cerebrovascular disease. Lancet Neurol. 2013;12:597–608. doi: 10.1016/S1474-4422(13)70057-7. [DOI] [PubMed] [Google Scholar]
- 21.Miura T, Kobayashi M, Sonoo M, Isii K, Shimizu T. An adult case of Moyamoya disease presenting with transient hemichorea. Rinsho Shinkeigaku. 2002;42:45–7. [PubMed] [Google Scholar]
- 22.Morigaki R, Uno M, Suzue A, Nagahiro S. Hemichorea due to hemodynamic ischemia associated with extracranial carotid artery stenosis. Report of two cases. J Neurosurg. 2006;105:142–7. doi: 10.3171/jns.2006.105.1.142. [DOI] [PubMed] [Google Scholar]
- 23.Murakami H, Inaba M, Nakamura A, Ushioda T. Ipsilateral hyperperfusion after neck clipping of a giant internal carotid artery aneurysm. Case report. J Neurosurg. 2002;97:1233–6. doi: 10.3171/jns.2002.97.5.1233. [DOI] [PubMed] [Google Scholar]
- 24.Netravathi M, Pal PK, Indira DB. A clinical profile of 103 patients with secondary movement disorders: Correlation of etiology with phenomenology. Eur J Neurol. 2012;19:226–33. doi: 10.1111/j.1468-1331.2011.03469.x. [DOI] [PubMed] [Google Scholar]
- 25.Pandey P, Bell-Stephens T, Steinberg GK. Patients with moyamoya disease presenting with movement disorder. J Neurosurg Pediatr. 2010;6:559–66. doi: 10.3171/2010.9.PEDS10192. [DOI] [PubMed] [Google Scholar]
- 26.Pareés I, Hernández-Vara J, Alvarez-Sabín J. Post-stroke hemichorea: Observation-based study of 15 cases. Rev Neurol. 2010;51:460–4. [PubMed] [Google Scholar]
- 27.Pareés I, Pujadas F, Hernández-Vara J, Lorenzo-Bosquet C, Cuberas G, Munuera J, et al. Reversible hemichorea associated with extracranial carotid artery stenosis. J Neurol Sci. 2011;300:185–6. doi: 10.1016/j.jns.2010.08.068. [DOI] [PubMed] [Google Scholar]
- 28.Park SY, Kim HJ, Cho YJ, Cho JY, Hong KS. Recurrent hemichorea following a single infarction in the contralateral subthalamic nucleus. Mov Disord. 2009;24:617–8. doi: 10.1002/mds.22423. [DOI] [PubMed] [Google Scholar]
- 29.Parmar RC, Bavdekar SB, Muranjan MN, Limaye U. Chorea: An unusual presenting feature in pediatric Moyamoya disease. Indian Pediatr. 2000;37:1005–9. [PubMed] [Google Scholar]
- 30.Pavlakis SG, Schneider S, Black K, Gould RJ. Steroid-responsive chorea in moyamoya disease. Mov Disord. 1990;6:347–9. doi: 10.1002/mds.870060414. [DOI] [PubMed] [Google Scholar]
- 31.Sakai K, Kyoshima K, Ohigashi Y, Unoki T, Kobayashi S, Meguro M. Generalized choreic movement associated with subarachnoid hemorrhage. No To Shinkei. 1991;43:875–80. [PubMed] [Google Scholar]
- 32.Shanahan P, Hutchinson M, Bohan A, O’Donoghue D, Sheahan K, Owens A. Hemichorea, moya-moya, and ulcerative colitis. Mov Disord. 2001;16:570–2. doi: 10.1002/mds.1095. [DOI] [PubMed] [Google Scholar]
- 33.Spengos K, Tsivgoulis G, Toulas P, Vemmos K, Vassilopoulos D, Spengos M. Hyperventilation-enhanced chorea as a transient ischaemic phenomenon in a patient with moyamoya disease. Eur Neurol. 2003;51:172–5. doi: 10.1159/000077665. [DOI] [PubMed] [Google Scholar]
- 34.Spetzler RF, Wilson CB, Weinstein P, Mehdorn M, Townsend J, Telles D. Normal perfusion pressure breakthrough theory. Clin Neurosurg. 1977;25:651–72. doi: 10.1093/neurosurgery/25.cn_suppl_1.651. [DOI] [PubMed] [Google Scholar]
- 35.Sugino T, Ohtaki M, Wanibuchi M, Kin S, Houkin K. Hyperperfusion Syndrome After Clipping an Unruptured Cerebral Aneurysm. Neurol Med Chir. 2010;50:306–9. doi: 10.2176/nmc.50.306. [DOI] [PubMed] [Google Scholar]
- 36.Sugiura A, Fujimoto M. Facial chorea and hemichorea due to cardiogenic cerebral embolism in the cortex and subcortical white matter. Rinsho Shinkeigaku. 2006;46:415–7. [PubMed] [Google Scholar]
- 37.Sundt TM, Sharbrough FW, Piepgras DG, Kearns TP, Messick JM, O’Fallon WM. Correlation of cerebral blood flow and electroencephalographic changes during carotid endarterectomy: With results of surgery and hemodynamics of cerebral ischemia. Mayo Clin Proc. 1981;56:533–43. [PubMed] [Google Scholar]
- 38.Takanashi J, Sugita K, Honda A, Niimi H. Moyamoya syndrome in a patient with Down syndrome presenting with chorea. Pediatr Neurol. 1993;9:396–8. doi: 10.1016/0887-8994(93)90111-o. [DOI] [PubMed] [Google Scholar]
- 39.Teo K, Choy DK, Lwin S, Ning C, Yeo TT, Shen L, et al. Cerebral hyperperfusion syndrome after superficial temporal artery-middle cerebral artery bypass for severe intracranial steno-occlusive disease: A case control study. Neurosurgery. 2013;72:936–42. doi: 10.1227/NEU.0b013e31828bb8b3. [DOI] [PubMed] [Google Scholar]
- 40.Watanabe K, Negoro T, Maehara M, Takahashi I, Nomura K, Miura K. Moyamoya disease presenting with chorea. Pediatr Neurol. 1989;6:40–2. doi: 10.1016/0887-8994(90)90077-e. [DOI] [PubMed] [Google Scholar]
- 41.Zheng W, Wanibuchi M, Onda T, Liu H, Koyanagi I, Fujimori K, et al. A case of moyamoya disease presenting with chorea. Childs Nerv Syst. 2006;22:274–8. doi: 10.1007/s00381-004-1104-2. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.