

Abstract
BACKGROUND
Children with peri-natal stroke may show evidence of contralateral spatial neglect. The goal of this study was to determine whether a clock drawing task commonly used in adults to identify neglect would be effective in detecting neglect in children with peri-natal stroke.
METHODS
Thirty-eight individuals (age range 6–21 years) with left hemisphere (LH) or right hemisphere (RH) peri-natal onset unilateral lesions and one hundred seventy-nine age-matched controls were given the free-drawn Clock Drawing Task (CDT) in a cross-sectional design. An adapted scoring system that evaluated right- and left-sided errors separately was developed as part of the investigation.
RESULTS
Children with LH lesions made a greater number of errors on both the right and left sides of the clock drawings in all age subgroups (6–8 years, 9–14 years, and 15–21 years) compared to controls. Children with RH lesions showed greater left and right errors in the younger groups compared to controls, with significantly poorer performance on the left at 6–8 years, suggestive of contralateral neglect. However, by ages 15–21 years, the RH lesion subjects no longer differed from controls.
CONCLUSIONS
Clock drawing can identify spatial neglect in children with early hemispheric damage. However, brain development is a dynamic process, and as children age, spatial neglect may no longer be evident. These findings demonstrate the limitations of predicting long-term outcome after peri-natal stroke from early neuro-cognitive data. Children with peri-natal stroke may require different neural pathways to accomplish specific skills or to overcome deficits, but ultimately they may have “typical” outcomes.
Keywords: clock drawing, peri-natal stroke, spatial neglect
Introduction
Drawing is a task that involves complex neurological, psychological, and motor actions and can therefore be used to investigate both motor and cognitive functions of patients in clinical settings. The Clock Drawing Test (CDT) was originally used to evaluate visuo-constructive abilities, and is now broadly used to assess cognitive impairments in adults. 1–3 The CDT has been used as a clinical indicator of spatial dysfunction and unilateral neglect in adults. Spatial neglect is a neuropsychological syndrome occurring after damage to one hemisphere of the brain that involves a deficit in attention to stimuli, generally in contralesional space. 4, 5 Adults with right hemisphere stroke have generally shown more severe and persistent contralateral neglect than those with left hemisphere damage, leading to the hypothesis that the right hemisphere may be dominant for spatial attention. 6–10 Clock drawings in adults may demonstrate neglect of the contralateral half of extra- personal space after stroke by omission of numbers, transposition of the numbers and hands from the neglected side to the other, or improper spatial layout of numbers. In the most severe cases of neglect, clock drawings may show all numbers drawn on the side of the clock ipsilateral to the lesion. 4, 11
Clock drawing has rarely been studied or used clinically in children. However, children do learn to draw a clock in school at an early age; thus, the task should have applicability for school-age children, both to assess constructional ability and to look for evidence of hemi-spatial neglect in children with focal brain injury. Neglect of contralateral hemispace has been demonstrated in children with peri-natal stroke, primarily using cancellation and search tasks.6 However, such tasks are relatively straightforward and may underestimate the extent of neglect. Since clock drawing is more complex and requires several steps, it is possible that clock drawing might detect more subtle impairments. Questions also remain regarding whether evidence of neglect declines as the children get older, and whether the presence of neglect might interfere with real-life activities. The current prospective study was designed to compare clock drawings of children with peri-natal stroke to those of typically developing controls in order to determine whether the CDT revealed evidence of hemi-spatial neglect in children with focal lesions, and to delineate the effect of age on clock drawing skill and spatial neglect.
Methods
Study Population
Two hundred seventeen subjects between the ages of 6 years and 21 years participated in this study. Twenty-one subjects had LH lesions (12 males, 9 females; age range 6–19 years; age M = 12 years, SD ± 4 years), seventeen subjects had RH lesions (11 males, 6 females; age range 6–21 years; age M = 10 years, SD = 4 years), and one hundred seventy-nine subjects were typically developing controls with no neurological conditions (75 males, 104 females; age range 6–20 years; age M = 12 years, SD = 4 years).
All of the children in the focal lesion groups sustained a single, unilateral, peri-natal arterial ischemic or hemorrhagic infarct, which was documented by medical history and neuro-imaging (CT or MRI). Each lesion was coded for site (hemisphere and lobes involved) by a clinical neuro-radiologist blinded to subject status. A severity score was assigned for each scan based on a scoring system utilized in our previous studies12. Children were either recruited in infancy from local neonatal intensive care units or through referrals from pediatric neurology practices locally, and participated in longitudinal studies of cognitive development over time. All children received a complete neurological examination that documented, among other details, presence or absence of hemiparesis, visual fields to confrontation, and sensory and motor functions.
Control children were recruited primarily through fliers placed in pediatricians’ offices and local community centers, advertisements in parent magazines, and by word of mouth. Control participants had no significant neurological or psychiatric history, and had normal medical and developmental histories.
All children examined for the study were able to understand the procedure and perform the task.
Informed consent was obtained for all participants prior to testing, in accordance with the procedures of the University of California-San Diego Institutional Review Board.
Clock Drawing Task
Subjects were provided with a pen and a plain white 8-½ × 11 inch sheet of paper. They were asked to draw a clock and to put in the time at 10 minutes after 11, without any time limit on performance. The center of the sheet was aligned with the subject’s midline and the subject was instructed not to tilt or turn the paper.
Scoring System
An adapted scoring system was developed to identify errors including omissions, repetitions, errors in spatial arrangement of numbers, reversals, incorrect placement of hands, and perseveration (numbering beyond 12). For this purpose, different available scoring protocols for rating the clock drawings were reviewed 13–16 and an adapted system for the CDT that considered lateralized errors was designed (Table 1). This scoring system is comprised of a 25-point scale for an overall score of correct features. In addition to the total score, the system quantified left-sided and right-sided errors, and combined them to calculate total errors for each clock drawing. Two independent raters scored the CDTs separately and compared the results. Disagreements in scoring were resolved following additional review and discussion.
Table 1.
Scoring System for clock-drawing task
| Partial Score | L-Error | R-Error | |
|---|---|---|---|
| Omission | 2: all numbers present 1: one number omitted 0: more than one number omitted |
1: for each omitted number on the left side | 1: for each omitted number on the right side |
| Repetition | 2: no number repeated 1: one number repeated 0: more than one number repeated |
1: for each repeated number on the left side | 1: for each repeated number on the right side |
| Rotation | 1: no number rotated more than 90 degrees 0: at least one number rotated more than 90 degrees |
1: for each rotated number (greater than 90 degrees) on the left side | 1: for each rotated number (greater than 90 degrees) on the right side |
| Perseveration | 1: no number beyond 12 0: numbers beyond 12 |
1: for each number beyond 12 on the left side | 1: for each number beyond 12 on the right side |
| Misplacement | 2: for each filled quadrant 1: for half quadrant 0: missing quadrant |
2: for any quadrant missed completely on the left side 1: for any quadrant missed partially on the left side or having less than 4 numbers (including borders) |
2: for any quadrant missed completely on the right side 1: for any quadrant missed partially on the right side or having less than 4 numbers (including borders) |
| 12-6 Alignment | 1: 12-6 directly opposite each other 0: 12-6 not directly opposite each other |
1: if either 12 or 6 moved to the right side | 1: if either 12 or 6 moved to the left side |
| 3–9 Alignment | 1: 3–9 directly opposite each other 0: 3–9 not directly opposite each other |
1: if 3 is misplaced | 1: if 9 is misplaced |
| Right Time | 1: right time (11:10) 0: not the right time |
--- | --- |
| Hand Switch | 2: hands not switched 1: hands switched 0: wrong time |
--- | --- |
| Hand Absence | 2: both hands present 1: only one hand present 0: no hand present |
--- | --- |
| Hour Hand Shift | --- | 1: hour hand shifted to the right or absent | 1: hour hand shifted to the left or absent |
| Minute Hand Shift | --- | 1: minute hand shifted to the right or absent | 1: minute hand shifted to the left or absent |
| Distorted Circle | 1: no major circle distortion 0: major circle distortion |
1: major distortion or omission of the circle on the left side | 1: major distortion or omission of the circle on the right side |
| Displacement | 2: no displacement 1: 1 to 2 quadrants displaced 0: 3 to 4 quadrants displaced |
1: for each displaced quadrant on the left side 1: one or both quadrants omitted on the left side |
1: for each displaced quadrant on the right side 1: one or both quadrants omitted on the right side |
| Number Mirrored | 1: no number mirrored 0: at least one number mirrored |
1: for any mirrored number on the left side | 1: for any mirrored number on the right side |
Statistical Analysis
Between group differences were analyzed using an ANOVA framework with Bonferroni-corrected follow-up tests. The independent variables were group membership (LH lesion, RH lesion, control). The dependent variables were total score, total errors, left errors, and right errors. Paired t-tests were used to examine within-group differences for left vs. right errors for all three groups (LH, RH, and controls). Once the initial data were analyzed, children in the focal lesion group were coded as either with neglect or without neglect based on a calculation of lateralized errors (defined by us a priori as contralateral error – ipsilateral error ≥ 2). Existence of hemiparesis in the children with neglect compared to children without neglect was analyzed using χ2 tests. Alpha was set at .05 in all statistical analyses.
Location of the lesion within the hemisphere in children with and without neglect was examined qualitatively because the numbers of subjects in some groups were too small for meaningful statistical analyses.
Results
The characteristics of the focal lesion group, including age, gender, lesion side and site, and presence or absence of neglect and hemiparesis are displayed in Table 2.
Table 2.
Subject information for lesion groups. (Lobe F: Frontal, T: Temporal, P: Parietal, O: Occipital). Neglect was defined as contralateral error – ipsilateral error score ≥ 2.
| Age | Gender | Lesion Side | Lobe | Severity | Neglect | Hemiparesis |
|---|---|---|---|---|---|---|
| 6 | Male | Left | F/T/P/O | 5 | No | Yes |
| 7 | Male | Left | F/T/P/O | 5 | No | No |
| 7 | Male | Left | F/P | 5 | No | Yes |
| 7 | Male | Left | P | 4 | Yes | Yes |
| 8 | Female | Left | T | 4 | No | No |
| 8 | Male | Left | F | 4 | No | Yes |
| 8 | Male | Left | F/P | 5 | Yes | No |
| 9 | Female | Left | F/T/P/O | 5 | No | Yes |
| 9 | Male | Left | T | 4 | No | No |
| 10 | Male | Left | F | 4 | Yes | Yes |
| 11 | Male | Left | F | 4 | Yes | Yes |
| 11 | Female | Left | T/P | 5 | No | Yes |
| 13 | Female | Left | F/T | 5 | No | No |
| 13 | Male | Left | F/P/O | 5 | No | No |
| 13 | Female | Left | F/T/P | 5 | Yes | Yes |
| 17 | Female | Left | F | 4 | No | No |
| 17 | Female | Left | F/T/P/O | 5 | No | Yes |
| 17 | Female | Left | P/O | 5 | No | No |
| 17 | Female | Left | F/T/P | 5 | Yes | Yes |
| 19 | Male | Left | F/T/P | 5 | Yes | No |
| 16 | Male | Left | T | 4 | No | Yes |
| 6 | Female | Right | F | 4 | No | Yes |
| 7 | Female | Right | F | 4 | Yes | No |
| 7 | Male | Right | F/T/P | 5 | Yes | Yes |
| 7 | Female | Right | F/T/P/O | 5 | Yes | Yes |
| 8 | Male | Right | F/T/P | 5 | Yes | Yes |
| 9 | Female | Right | F/P/O | 5 | No | Yes |
| 9 | Male | Right | F/T/P | 5 | No | Yes |
| 9 | Male | Right | F(SUBCORT) | 3 | No | No |
| 9 | Male | Right | P/O | 5 | Yes | Yes |
| 9 | Female | Right | F(SUBCORT) | 3 | No | Yes |
| 9 | Female | Right | F/T/P/O | 5 | No | Yes |
| 11 | Male | Right | P | 4 | No | No |
| 11 | Male | Right | F/T/P/O | 5 | No | Yes |
| 11 | Male | Right | F | 4 | No | No |
| 13 | Male | Right | F/T | 5 | No | Yes |
| 15 | Male | Right | F/T/P/O | 5 | No | Yes |
| 21 | Male | Right | P/O | 5 | No | No |
Because of the wide age range of children in this study, we divided them into three subgroups based on age (6 to 8 years, 9 to 14 years, and 15 years and older). The rationale for this division is based on our observation that the total errors of our control group dropped dramatically from ages 8 to 9, and then from 14 to 15. A previous study of typically developing children also showed major changes in clock drawing ability after age 8.17
Figure 1 demonstrates representative clock drawings for LH, RH, and control children in each age group. The means for total score, total errors, left errors and right errors for each age subgroup of the Control, LH, and RH groups are displayed in Table 3 and Figure 2. Children with either LH or RH lesions had lower total scores and made more errors than those in the control group within each age subgroup, except for the oldest RH lesion group.
Figure 1.

Samples of clock drawings of children in age subgroup 1 (6–8 year old) on the top row (a–d), age subgroup 2 (9–14 year old) on the middle row (e–h), and age subgroup 3 (15 year old and older) on the bottom row (i–l).
Table 3.
Total scores, total errors, right errors and left errors for the control, LH (left hemisphere) and RH (right hemisphere) lesion groups, within each age subgroup; *p < 0.05, **p < 0.01 for LH/RH vs. control group comparisons.
| Age Subgroup | |||||||
|---|---|---|---|---|---|---|---|
| 6–8 years | 9–14 years | ≥15 years | |||||
| M | SD | M | SD | M | SD | ||
| Total Score | Control | 19.1 | 2.9 | 22.5 | 2.0 | 24.0 | 1.2 |
| LH | 15.9** | 5.0 | 19.4* | 4.5 | 19.7* | 2.9 | |
| RH | 12.6* | 4.0 | 20.0* | 4.5 | 23.0 | 2.8 | |
| Total Errors | Control | 5.4 | 3.7 | 1.7 | 1.5 | 0.7 | 0.8 |
| LH | 11.7* | 9.3 | 5.1* | 4.1 | 4.5* | 2.5 | |
| RH | 15.2* | 8.2 | 4.7* | 3.8 | 2.5 | 3.5 | |
| Left Errors | Control | 2.8 | 2.5 | 0.7 | 1.1 | 0.2 | 0.5 |
| LH | 5.4** | 4.3 | 2.6* | 3.2 | 2.3* | 2.5 | |
| RH | 9.0* | 4.3 | 2.0* | 2.3 | 1.0 | 1.4 | |
| Right Errors | Control | 2.6 | 2.1 | 1.1 | 1.0 | 0.5 | 0.7 |
| LH | 6.3* | 5.6 | 2.5* | 2.3 | 2.2* | 1.3 | |
| RH | 6.2* | 4.0 | 2.7* | 2.5 | 1.5 | 2.1 | |
Figure 2.
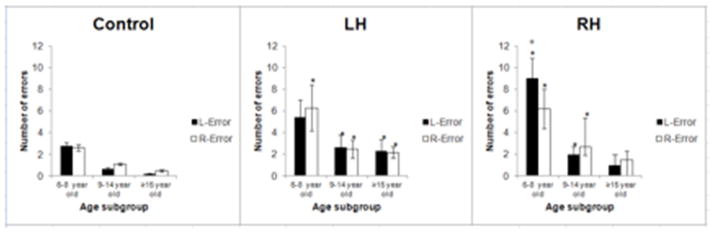
Mean number of left errors versus right errors made by control (n = 179), left hemisphere (LH) lesion (n = 21), and right hemisphere (RH) lesion (n = 17) participants within each age subgroup. Error bars represent standard error of the mean.
* designates statistical significance (p < .05) for lesion vs. control group comparison.
+ designates statistical significance (p < .05) for left error vs. right error comparison within the lesion group.
Between-group follow-up tests indicated that the LH lesion subjects made significantly more errors on both the right and left sides compared with controls (all p values ≤ 0.013) except at the youngest age, where left-sided errors only approached significance (p=0.083). RH lesion subjects made significantly more errors than the control group on both the left and right sides in the two younger age groups, but were no different from controls in the oldest group.
Within group analyses revealed that significantly more left-sided than right-sided errors were made by the youngest RH lesion children (p = 0.013; Figure 2). In the youngest LH lesion subgroup, although more errors were made on the right side than on the left side, the difference was not statistically significant.
No specific pattern of error type (e.g. only omission, only misplacement, etc.) was found in any control or lesion group or age subgroup. The children within the focal lesion group (left and right combined) were divided into neglect and non-neglect subgroups as described above. Presence of hemiparesis in the children with neglect compared to children without neglect was not qualitatively different. Location of the lesion within each hemisphere was not found to be related to the presence or absence of neglect. For example, 57% of children with left parietal involvement and 60% with left frontal involvement did not demonstrate neglect; 64% of children with right parietal involvement and 71% of children with right frontal involvement did not demonstrate neglect.
Discussion
This study demonstrated several important findings. First, children with either right or left brain damage acquired in the peri-natal period may show evidence of contralateral spatial neglect, as had been demonstrated previously using cancellation and search tasks6. Second, the clock drawing task can be used to identify spatial neglect even in young school-age children with early focal brain damage. Third, neither hemiparesis nor location of the lesion within the hemisphere appear to explain the neglect phenomenon, although only qualitative analyses could be used for the latter data because of small numbers of children in each group. The study further demonstrated that even 7- and 8-year-old typically developing children can draw an accurate representation of a clock from memory, making this a useful tool with which to assess possible hemi-neglect as well as constructional abilities in young school-age children.
The results of this study show a pattern of spatial neglect in children with early focal brain damage that is distinct from that which has been described in adults. The pattern of bilateral errors seen in children with LH lesions is different from the pattern of mild and transient contralateral neglect observed in adults with LH lesions. 8–10 On the other hand, the pattern of contralateral inattention seen in children with RH lesions is consistent with what is seen in adults, 6–10 but appears to be more pronounced in the younger age range and to largely disappear by adolescence.
In a recent study from our laboratory, Thareja et al.6 investigated the presence of spatial neglect in school-age children with peri-natal stroke, using both a visual cancellation task and manual exploration task. Although the clock drawing task integrates different components including memory, constructional abilities, and the knowledge of time, that require additional complexity compared with the tasks used by Thareja et al.6, our findings are remarkably similar to their results. They found that children with LH lesions had bilateral difficulties in performing both tasks. Using a very different task, we also found that children with early LH damage performed more poorly on both left and right sides of their clock drawings compared to controls throughout all age groups. This pattern of bilateral inattention seen in children with LH damage is more often observed in adults with RH lesions.18 Further, Thareja et al.6 showed that children with RH lesions demonstrated contralateral neglect. Our study found similar results for the RH lesion group, but these differences were significant only at the younger ages (6–8 years). The older RH lesion group (15–21 years) performed at a similar level to controls.
One potential explanation could be the lack of sensitivity of the clock drawing test to identify neglect at older ages. Another possibility is that the plasticity of the developing brain allows for the development of compensatory pathways to diminish the consequences of earlier focal brain injury.19 Using a spatial construction task, Stiles et al. 19 also found that children with RH lesions performed more poorly than controls only at younger ages, but were comparable to controls as they got older. The children in the Stiles study demonstrated considerable improvement in spatial construction ability over time. They concluded that these children gained proficiency by developing task-specific compensatory strategies, rather than general recovery of spatial skills. It is possible that in the clock drawing task, we see similar compensatory changes over time in the RH lesion group. Children with LH lesions do not, however, achieve age-appropriate clock drawing skills even into adolescence, suggesting that their compensatory skills may be more limited than those of RH lesion children. It is unclear why this difference exists. One possible explanation is the crowding hypothesis 20, which suggests that when the left hemisphere is damaged, language moves to other areas of the brain, “crowding out” other cognitive functions. Other potential limitations to plasticity, including size and location of the lesion, may also play a role. We did not, however, find any obvious effect of size or of lesion location within the hemisphere as an indicator of neglect in the current study.
It is important to recognize that the type of scoring system utilized for clock drawing must be considered in relation to the questions being asked. If constructional ability in general is the goal of the test, there are a number of scoring systems already described for adults that work well. If, however, spatial neglect is being studied, then a scoring system that evaluates lateralized errors must be applied. To reduce evaluator bias, various clock drawing scoring protocols have been developed for adults with spatial neglect 2, 13, 14, 22 and other cognitive impairments. 23–25 The first scoring system used for children with spatial neglect was devised by Edmonds et al. (cited in Cohen et al.)17 but it has not been universally applied. In the present study, a comprehensive scoring system was designed based on the published adult literature as well as errors in clock drawings unique to children. Moreover, existent scoring systems code predominantly for constructional ability and not neglect, so for this study we designed a system that would be sensitive to neglect as well as overall constructional ability. Following the characteristics of a scoring system that previous studies have recommended,3, 14, 25 the scoring system devised in this study is easy to administer and quick to score and it can be applied easily by clinicians. On the other hand, we found that scoring a clock drawing of a child can be subjective and requires some standard training to be useful for this purpose.
In summary, the free-draw clock drawing task is able to detect differences between children with peri-natal stroke and typically developing children. This test is able to identify neglect in a subset of younger children with RH damage. It can identify constructional deficiencies in both groups and it can track improvement over time. However, it may be most useful in conjunction with other tests of spatial attention, such as a cancellation test.
Clock drawing can identify spatial neglect in children with early hemispheric damage. However, brain development is a dynamic process, and as children age, spatial neglect may no longer be evident. These findings demonstrate the limitations of predicting long-term outcome after peri-natal stroke from early neuro-cognitive data. Children with peri-natal stroke may require different neural pathways to accomplish specific skills or to overcome deficits, but ultimately they may have “typical” outcomes.
Acknowledgments
Our sincerest appreciation is extended to all of the children and young adults, and their parents, whose participation was vital to this research. This research was supported by the National Institutes of Health (NS22343, Center for the Study of the Neurological Basis of Language, D. Trauner P.I.), and by NIH Clinical Research Training Grant T32 RR023254.
Appendix 1: Scoring System
| Partial Score | L-Error | R-Error | |
|---|---|---|---|
| Omission | 2: all numbers present 1: one number omitted 0: more than one number omitted |
1: for each omitted number on the left side | 1: for each omitted number on the right side |
| Repetition | 2: no number repeated 1: one number repeated 0: more than one number repeated |
1: for each repeated number on the left side | 1: for each repeated number on the right side |
| Rotation | 1: no number rotated more than 90 degrees 0: at least one number rotated more than 90 degrees |
1: for each rotated number (greater than 90 degrees) on the left side | 1: for each rotated number (greater than 90 degrees) on the right side |
| Perseveration | 1: no number beyond 12 0: numbers beyond 12 |
1: for each number beyond 12 on the left side | 1: for each number beyond 12 on the right side |
| Misplacement | 2: for each filled quadrant 1: for half quadrant 0: missing quadrant |
2: for any quadrant missed completely on the left side 1: for any quadrant missed partially on the left side or having less than 4 numbers (including borders) |
2: for any quadrant missed completely on the right side 1: for any quadrant missed partially on the right side or having less than 4 numbers (including borders) |
| 12-6 Alignment | 1: 12-6 directly opposite each other 0: 12-6 not directly opposite each other |
1: if either 12 or 6 moved to the right side | 1: if either 12 or 6 moved to the left side |
| 3–9 Alignment | 1: 3–9 directly opposite each other 0: 3–9 not directly opposite each other |
1: if 3 is misplaced | 1: if 9 is misplaced |
| Right Time | 1: right time (11:10) 0: not the right time |
--- | --- |
| Hand Switch | 2: hands not switched 1: hands switched 0: wrong time |
--- | --- |
| Hand Absence | 2: both hands present 1: only one hand present 0: no hand present |
--- | --- |
| Hour Hand Shift | --- | 1: hour hand shifted to the right or absent | 1: hour hand shifted to the left or absent |
| Minute Hand Shift | --- | 1: minute hand shifted to the right or absent | 1: minute hand shifted to the left or absent |
| Distorted Circle | 1: no major circle distortion 0: major circle distortion |
1: major distortion or omission of the circle on the left side | 1: major distortion or omission of the circle on the right side |
| Displacement | 2: no displacement 1: 1 to 2 quadrants displaced 0: 3 to 4 quadrants displaced |
1: for each displaced quadrant on the left side 1: one or both quadrants omitted on the left side |
1: for each displaced quadrant on the right side 1: one or both quadrants omitted on the right side |
| Number Mirrored | 1: no number mirrored 0: at least one number mirrored |
1: for any mirrored number on the left side | 1: for any mirrored number on the right side |
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- 1.Plummer P, Morris ME, Dunai J. Assessment of unilateral neglect. Phys Ther. 2003;83(8):732–740. [PubMed] [Google Scholar]
- 2.Smith AD, Gilchrist ID, Butler SH, Harvey M. Around the clock surveillance: simple graphic disturbance in patients with hemispatial neglect carries implications for the clock drawing task. J Neurol Neurosurg Psychiatry. 2006;77(3):407–409. doi: 10.1136/jnnp.2005.071472. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Agrell B, Dehlin O. The clock-drawing test. Age Ageing. 1998;27:399–403. doi: 10.1093/ageing/afs149. [DOI] [PubMed] [Google Scholar]
- 4.Ishiai S, Sugishita M, Ichikawa T, Gono S, Watabiki S. Clock-drawing test and unilateral spatial neglect. Neurology. 1993;43(1):106–110. doi: 10.1212/wnl.43.1_part_1.106. [DOI] [PubMed] [Google Scholar]
- 5.Halligan PW, Marshall JC. Graphic neglect-more than the sum of the parts. Neuroimage. 2001;14:S91–97. doi: 10.1006/nimg.2001.0821. [DOI] [PubMed] [Google Scholar]
- 6.Thareja T, Ballantyne AO, Trauner DA. Spatial analysis after peri-natal stroke: patterns of neglect and exploration in extra-personal space. Brain Cogn. 2012;79(2):107–116. doi: 10.1016/j.bandc.2012.02.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Heilman KM, Watson RT, Valenstein E. Spatial neglect. In: Karnath HO, Milner AD, Vallar G, editors. The cognitive and neural bases of spatial neglect. Oxford: Oxford University Press; 2002. pp. 3–30. [Google Scholar]
- 8.Bowen A, McKenna K, Tallis RC. Reasons for variability in the reported rate of occurrence of unilateral spatial neglect after stroke. Stroke. 1999;30(6):1196–1202. doi: 10.1161/01.str.30.6.1196. [DOI] [PubMed] [Google Scholar]
- 9.Gainotti G, Messerli P, Tissot R. Qualitative analysis of unilateral spatial neglect in relation to laterality of cerebral lesions. J Neurol Neurosurg Psychiatry. 1972;35(4):545–550. doi: 10.1136/jnnp.35.4.545. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Heilman KM, Van Den Abell T. Right hemisphere dominance for attention: the mechanism underlying hemispheric asymmetries of inattention (neglect) Neurology. 1980;30(3):327–330. doi: 10.1212/wnl.30.3.327. [DOI] [PubMed] [Google Scholar]
- 11.Friedman PJ. Clock drawing in acute stroke. Age Ageing. 1991;20:140–145. doi: 10.1093/ageing/20.2.140. [DOI] [PubMed] [Google Scholar]
- 12.Ballantyne AO, Spilkin AM, Hesselink J, Trauner DA. Plasticity in the developing brain: intellectual, language and academic functions in children with ischaemic perinatal stroke. Brain. 2008;131:2975–2985. doi: 10.1093/brain/awn176. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Richardson HE, Glass JN. A comparison of scoring protocols on the Clock Drawing Test in relation to ease of use, diagnostic group, and correlations with Mini- Mental State Examination. J Am Geriatr Soc. 2002;50(1):169–173. doi: 10.1046/j.1532-5415.2002.50024.x. [DOI] [PubMed] [Google Scholar]
- 14.Jouk A, Tuokko H. A reduced scoring system for the Clock Drawing Test using a population-based sample. Int Psychogeriatr. doi: 10.1017/S1041610212000804. Epub 2012 Jun 1. [DOI] [PubMed] [Google Scholar]
- 15.Lessig MC, Scanlan JM, Nazemi H, Borson S. Time that tells: critical clock drawing errors for dementia screening. Int Psychogeriatr. 2008;20:459–470. doi: 10.1017/S1041610207006035. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Tuokko H, Hadjistavropoulos T, Miller JA, et al. The Clock Test: administration and scoring manual. Toronto: Multi-Health Systems; 1995. [Google Scholar]
- 17.Cohen MJ, Ricci CA, Kibby MY, Edmonds JE. Developmental progression of clock face drawing in children. Child Neuropsychol. 2000;6(1):64–76. doi: 10.1076/0929-7049(200003)6:1;1-B;FT064. [DOI] [PubMed] [Google Scholar]
- 18.Weintraub S, Mesulam MM. Right cerebral dominance in spatial attention. Further evidence based on ipsilateral neglect. Arch Neurol. 1987;44(6):621–625. doi: 10.1001/archneur.1987.00520180043014. [DOI] [PubMed] [Google Scholar]
- 19.Stiles J, Trauner D, Engel M, Nass R. The development of drawing in children with congenital focal brain injury: evidence for limited functional recovery. Neuropsychologia. 1997;35(3):299–312. doi: 10.1016/s0028-3932(96)00088-7. [DOI] [PubMed] [Google Scholar]
- 20.Thomas M. Limits on plasticity. Journal of Cognition and Development. 2003;4(1):95– 121. [Google Scholar]
- 21.Lidzba K, Staudt M, Wilke M, Krägeloh-Mann I. Visuospatial deficits in patients with early left-hemispheric lesions and functional reorganization of language: consequence of lesion or reorganization? Neuropsychologia. 2006;44(7):1088–94. doi: 10.1016/j.neuropsychologia.2005.10.022. [DOI] [PubMed] [Google Scholar]
- 22.Tuokko H, Hadjistavropoulos T, Rae S, O’Rourke N. A comparison of alternative approaches to the scoring of clock drawing. Arch Clin Neuropsychol. 2000;15(2):137–148. [PubMed] [Google Scholar]
- 23.Mendez MF, Ala T, Underwood KL. Development of scoring criteria for the clock drawing test in Alzheimer’s disease. J Am Geriatr Soc. 1992;40:1095–1099. doi: 10.1111/j.1532-5415.1992.tb01796.x. [DOI] [PubMed] [Google Scholar]
- 24.Rouleau I, Salmon DP, Butters N, et al. Quantitative and qualitative analyses of clock drawings in Alzheimer’s and Huntington’s disease. Brain Cogn. 1992;18(1):70–87. doi: 10.1016/0278-2626(92)90112-y. [DOI] [PubMed] [Google Scholar]
- 25.Shulman KI, Shedletsky R, Silver I. The challenge of time: clock drawing and cognitive function in the elderly. Int J geriatr Psychiatr. 1986;1:135–140. [Google Scholar]