

SUMMARY
The present study aims to evaluate and validate the Italian version of Khalfa's questionnaire on hyperacusis (HQ). We recruited 117 patients (64 men, 53 women, mean age 53 years, range 14-88) with tinnitus for at least 3 months as a primary disorder. All patients completed the THI and the Italian version of the HQ and underwent audiometry, pitch and loudness tinnitus matching, otoacoustic emissions with distortion products (DPOAE) and uncomfortable loudness level (ULL). The overall performance of the tests was evaluated and compared using the area under the RO C curve (AUC) relative to the tests. The cut-off of the HQ was calculated. We also assessed the Cronbach's alpha (αC) for the HQ and its three major dimensions (attentional - αC1, emotional - αC2 and social - αC3). Statistical analysis showed no correlation between DPOAE, audiometry, ULL and gender. We observed a high correlation (p < 0.05) between hyperacusis and ULL described by the Spearman's ρ index (rs = 0.72). We found a cut-off of 16 indicative of hyperacusis comparing the area under the RO C curve (AUC) of HQ and audiometry, taken as a diagnostic reference, (sensitivity = 67.9% and specificity = 72.2%). The reliability of HQ was confirmed by a high αC = 0.89. The αC for the single dimensional scales were, respectively, αC1 = 0.73, αC2 = 0.72 and αC3 = 0.81. The Italian version of the HQ is recommended for proper and complete classification of patients with tinnitus and hyperacusis. From our study, we found a cut-off of 16 instead of the cut-off of 28 described as very high by other authors. Moreover, ULL was an important variable and can be discriminating in the evaluation of hyperacusis.
KEY WORDS: Khalfa, Hyperacusis questionnaire, Tinnitus, Uncomfortable loudness level (ULL)
RIASSUNTO
Il presente studio ha come scopo quello di valutare e dimostrare la validità della versione italiana del questionario sull'iperacusia di Khalfa (HQ). Sono stati reclutati 117 pazienti (64 uomini, 53 donne; età: 14-88 anni, media 53 anni) con acufene da almeno 3 mesi come disturbo primario. Tutti i pazienti hanno compilato il THI e la versione italiana del HQ e sono stati sottoposti ad esame audiometrico, acufenometria, otoemissioni acustiche con prodotti di distorsione (DPOAE) e soglia del fastidio (ULL). La performance complessiva dei test è stata valutata e confrontata usando l'area sotto le curve ROC (AUC) relative ai test. Il cut-off del HQ è stato calcolato. Inoltre abbiamo valutato l'alfa di Cronbach's (αC) per il HQ e per le sue tre scale dimensionali: attenzionale (αC1), emotiva (αC2) e sociale (αC3). La nostra analisi statistica non ha evidenziato alcuna correlazione tra DPOAE, esame audiometrico, ULL e sesso. Inoltre è stata osservata una elevata correlazione tra l'iperacusia e l'ULL, descritto dall'indice ρ di Spearman (rs = 0,72). È stato calcolato un cut-off di 16 indicativo di iperacusia, comparando l'area sotto la curva ROC (AUC) del HQ e l'audiometria, presa come riferimento diagnostico, (sensibilità = 67.89% e specificità = 72.22%). L'affidabilità del HQ è stata confermata da un alto αC = 0,89. L'αC per le singole scale dimensionali sono risultate rispettivamente αC1 = 0.73, αC2 = 0.72 e αC3 = 0.81. La versione italiana del HQ è consigliata per una classificazione appropriata e completa dei pazienti con iperacusia. Dal nostro studio abbiamo trovato un cut-off di 16 invece del cut-off di 28, descritto come molto alto da differenti autori. Inoltre, l'ULL risulta una importante variabile e può essere discriminante nella valutazione dell'iperacusia.
Introduction
Noise exposure is considered one of the most common causes of hearing loss that may lead to various disorders, such as loudness recruitment, tinnitus and hyperacusis 1. Hyperacusis can be part of the clinical spectrum of auditory and vestibular disorders, such as acoustic shock injury, Meniere's disease, otosclerosis, perilymphatic fistula, Bell's palsy and superior semicircular canal dehiscence (SSCD) 2 3. However, hyperacusis can also be due to several pathological conditions, some of which affect the neurological pathway (head injury, migraine, Lyme disease, Williams syndrome) or the psychological/psychiatric apparatus (acoustic spectrum disorders, chronic fatigue syndrome, fibromyalgia) 4 5. Tinnitus is defined as an exaggerated perception of sound in absence of an external source. Hyperacusis is a disorder of loudness perception, in which sound intensities that are considered comfortable by most people are perceived unbearably loud 5. Hyperacusis is described as a reduced tolerance to ordinary environmental sounds and is characterised by consistently exaggerated or inappropriate responses to sounds 6 7. Reported prevalence for sound intolerance in tinnitus patients ranges widely, from 30 8 up to 79% 9 10. This variability is probably due to the various techniques used in the literature to objectify hyperacusis complaints and results from the absence of a uniform standardised diagnostic procedure. Hyperacusis can occur without a loss of hearing thresholds 11. For both tinnitus and hyperacusis, however, hearing loss is a major risk factor. As the incidence of hearing loss will increase with the aging of the population, the incidence of tinnitus and hyperacusis may also increase 12.
Hyperacusis does not imply a higher than normal threshold sensitivity to sound, nor loudness recruitment (the rapid growth in perceived loudness with increasing sound intensity that occurs with sensorineural hearing loss) 13. Instead, in hyperacusis, sounds are not simply a bit loud, but truly unbearable 12.
Hyperacusis is due to an alteration in the central processing of sound in the auditory pathways where there is an abnormally strong reaction from exposure to moderate sound levels. The cochlea is often completely normal, although patients frequently wrongly believe it is irreversibly damaged. Hyperacusis is often associated with tinnitus, but the mechanisms are largely unknown 14.
Many authors consider that hyperacusis seems to increase in extent at times of anxiety, tiredness or stress 15 16. The pathophysiological mechanism that may explain this abnormal response during stress involves the release of endogenous dynorphins into the synaptic region beneath the inner hair cells. Subsequently, this mechanism leads to an enhanced glutamate neurotransmitter activity, causing the excessive loudness of the sound perceived 17. Nowadays, based on the limited evidence related to hyperacusis, it has been pointed out as a concomitant occurrence with tinnitus 18. Patients with hearing loss are exposed to a high risk to develop tinnitus and hyperacusis. Several studies showed a correlation but not causal relationships among hyperacusis, tinnitus and hearing loss 19.
Khalfa validated a questionnaire in order to screen several aspects of auditory symptoms and to quantify and evaluate the characteristics of hyperacusis 20. The questionnaire is divided into 2 parts. The first includes 3 binary questions giving general information on auditory disorders and noise exposure. The second part comprises 14 selfrating items that will be scored over three major dimensions: attentional (questions 1-4), social (questions 5-10) and emotional (questions 11-14). Answers to each question/ item are given on a 4-point scale, ranging from 'no' (scoring 0 points), 'yes a little' (scoring 1 point), 'yes, a lot' (scoring 2 points) to 'yes, quite a lot' (scoring 3 points). The hyperacusis questionnaire is highly sensitive to discriminate subjects with hyperacusis in the general population. A mean score greater than 28.4 is considered as indicative of hyperacusis. The questionnaire is useful in the quantification and characterisation of the clinical aspects of hyperacusis and is a valid instrument for follow- up. Meeus suggested that the cut-off value of 28 is too high and can underestimate some patients with hyperacusis 21. Overall, no correlations were found between scores on questionnaires and audiometric values. Other questionnaires to assess subjective distress, related to hypersensitivity to sound, are available such as the Multiple- Activity Scale for hyperacusis (MASH) 22 and the self-rating questionnaire on hypersensitivity to sound (GUF) 23. The MASH is designed for interview-based questioning and classifies hyperacusis into 4 grades from mild to very severe. The GUF is based on 15 questions and evaluates hyperacusis according to cognitive reactions, behavioural changes and emotional responses. The original GUF is in German, and a Spanish version is available 24. The Khalfa questionnaire (HQ) is also translated in other languages, most recently in Japanese 25.
The present study aims to evaluate and validate the Italian version of the HQ in view of its use as an essential tool in the evaluation of hyperacusis. Our assessment considers all the possible factors that can lead to higher degrees of failure secondary to this symptom.
Materials and methods
The Italian validation of the HQ consisted of three different phases.
In the first, three native speakers of Italian, bilingual in English, independently translated the original questionnaire into Italian with the permission of the author. Subsequently, we formed the pooled version that was then reviewed for the linguistic quality. This version was back translated into English and compared with the original questionnaire. The initial Italian version of the questionnaire was formulated and administered to patients (Appendix 1).
Participants
From November 2011 to December 2012, the final version of HQ was administered to 117 consecutive outpatients [64 male (54.7%) and 53 female (45.3%), age range 14-88 years, (mean 53)], with a primary complaint of tinnitus to improve population homogeneity. All patients had tinnitus for at least 3 months. All questionnaires were filled in by patients in a self-administered way. Exclusion criteria were the presence of recruitment and Ménière's disease evaluated with anamnesis and audiological data. Patients with a previous diagnosis of psychiatric disease were also excluded. Informed consent was obtained from each participant before examination.
Patients were also asked to complete the Italian version of Tinnitus Handicap Inventory (THI).
All patients underwent ENT clinical examination with anamnesis, otoscopy and audiometric evaluation. Pure-tone audiometry was performed at 0.125, 0.25, 0.5, 1, 2, 3, 4, 6 and 8 kHz. Pitch and loudness tinnitus matching was carried out for each patient using the method of adjustment by Newman et al. 26. Hyperacusis measurement includes uncomfortable loudness levels (ULL) which were measured at 0.25, 0.5, 1, 2, 4 and 8 kHz. Mild hyperacusis was considered in presence of ULL at 80-90 dB in 2 or more frequencies, moderate hyperacusis in presence of ULL at 65-75 dB in 2 or more frequencies and severe hyperacusis in presence of ULL at 60 dB or lower in 2 or more frequencies 27.
Otoacoustic emissions with distortion product (DPOAE) determined the hypothetical influence of hyperacusis on DPOAE parameters in tinnitus patients. DPOAE were recorded with f1/f2 = 1.22 and intensities of 65 dB (f1) and 55 dB (f2) SPL.
Statistical analysis
Cronbach's coefficient alpha (αC) assessed the scale reliability for the total score of HQ and for the three dimensions of the HQ (αC1, αC2 and αC3). Under the assumption that subjects were selected among those with some degree of acoustic impairment, a RO C analysis was carried out to estimate the performance of the HQ in discriminating medium and high levels of impairment. The diagnostic index variable used was the audiometric examination.
The αC was used to assess the validity of the Italian version of the HQ on the basis of internal consistency. Coefficients greater or equal to 0.70 were defined as acceptable, and those greater than or equal to 0.80 were defined as good. We compared the results to those obtained by Khalfa et al. (2002) on the original version of the HQ.
The statistical analysis preliminary studied the association among DPOAE, gender, ULL and audiometric examination, calculating pairwise Spearman correlations.
A proportional odds ratio (OR) model was worked out to account for the ordinal variable ULL with more than two categories. This model treated the variables gender (ORgender) and HQ (ORHQ) as regressors. The Brant test of parallel regression assumption was statistically significant (p < 0.05).
The analysis was carried out using STATA software version 12.
Results
We found that a cut-off of 16 was indicative of hyperacusis by comparing the RO C curves of HQ and audiometric examination (Fig. 1). The area under the RO C curve (AUC) of hyperacusis, evaluated by HQ, using audiometric examination as diagnostic reference variable (AUC = 0.67 ± 0.05), was statistically significant (p < 0.05). However, the AUC suggests a poorer performance of the HQ with respect to low and high ULL levels (optimal cut-off = 16, sensibility = 67.89%, specificity = 72.22%). Based on the cut off of 16 on HQ, 40.4% of patients with tinnitus also presented hyperacusis.
Fig. 1.
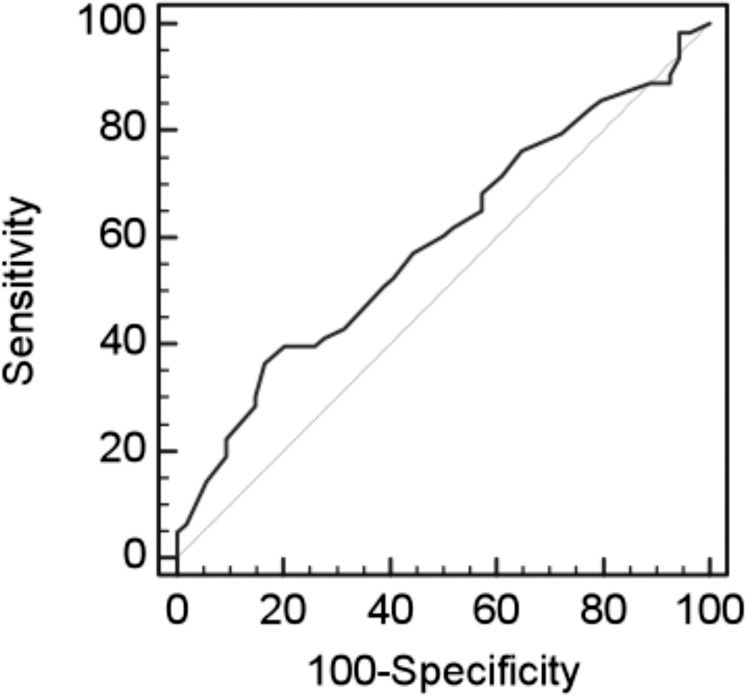
AUC of hyperacusis calculated using HQ score and audiometric exam.
The scale reliability of the Khalfa questionnaire was statistically significant (αC = 0.89). We evaluated the three dimensions in which the questionnaire is divided and found that the αC indexes were, respectively, αC1 = 0.73, αC2 = 0.72 and αC3 = 0.81.
From statistical analysis, there was no association between DPOAE and audiometric examination.
We also observed statistically significant (p < 0.05) Spearman's ρ index (rs = 0.72) between HQ and ULL.
We carried out an ordered logistic regression modelling having ULL (low, middle and high) as response variable with gender and HQ as regressors. The interpretation is that for a one unit increase in gender, i.e. going from 0 (male) to 1 (female), the odds of high ULL versus the combined middle and low categories are OR = 0.39 lower, given that all of the other variables in the model are held constant. The odds of the combined middle and high categories versus low ULL is OR = 0.39 times lower, given that all of the other variables are held constant. For each one unit increase in HQ, the odds of the high category of ULL versus the low and middle categories of ULL are OR = 1.07 times greater, given that the other variables in the model are held constant. Because of the proportional odds assumption, the same increase of OR = 1.07 times was found between low ULL and the combined categories of middle and high ULL (Table I). The likelihood ratio χ2 of 14.16 with a p < 0.05 confirms that our model as a whole is statistically significant, compared to the null model with no predictors. Therefore, we can affirm that gender and HQ are significant and determinant of ULL scores.
Table I.
Ordered logistic regression with ULL, gender and HQ. (OR: odds ratio. SE: standard error. P significant level, Cut 1: cut-off mild ULL. Cut2: cutoff moderate ULL. Cut3: cut-off severe ULL).
| ULL | OR | SE | P |
|---|---|---|---|
| gender | 0.39 | 0.18 | 0.039 |
| HQ | 1.07 | 0.028 | 0.007 |
| Cut1 | -3.86 | 0.84 | |
| Cut2 | 1.83 | 0.55 | |
| Cut3 | 3.57 | 0.66 |
Table I reports the cut-off points of the latent structure model that can be used in a clinical context.
Discussion
As demonstrated for both the original version and the Dutch version 21 of the HQ, the Italian adaptation does not seem to be affected by age and gender and this result contributes to its general, cross-cultural validity as a selfreport measure of perceived severity of hyperacusis.
In our study, we found a cut-off of 16 instead of the previous cut-off of 28 identified by Khalfa to represent strong auditory hypersensitivity, described as very high by different authors. This difference in cut-off could be due to the selection criteria of the subject sample. Khalfa selected the sample among the general population without a specific criterion since the main objective was solely to evaluate the sensitivity of the questionnaire among the general population 20. Otherwise, Meeus et al. studied hyperacusis with the HQ and the MASH in 46 patients with a primary complaint of tinnitus. This study provided a Dutch validated version of the HQ and suggested that the cut-off value of 28 is too high and can underestimate some patients with hyperacusis 21.
The Italian version of HQ has an high and good internal consistency reliability for the total scale (αC = 0.89, sensibility = 67.89%, specificity = 72.22%) and for the three dimensions: attentional dimension (αC 1 = 0.73), social dimension (αC2 = 0.72) and emotional dimension (αC3 = 0.81). It is worth noting that the high specificity of the HQ is important in detecting the absence of the affection.
The original version demonstrated three dimensions with satisfactory internal consistency reliability according to αC values: respectively, 0.66 for attentional dimension, 0.68 for social dimension and 0.67 for emotional dimension 20. The Dutch version of the HQ had a good internal consistency (αC = 0.85). In contrast with other authors 21, we report good correlation between HQ and ULL scores.
Compared with hearing loss and tinnitus, little attention is given to hyperacusis.
In our study, we found hyperacusis in 40.4% of patients with tinnitus, as reported in the literature (40%) 8. Schecklmann et al. indicated a rate of hyperacusis of 55% calculated among 1713 patients with tinnitus. In the study by Schecklmann et al., hyperacusis was investigated with the question "Do sounds cause you pain or physical discomfort?" of the Tinnitus Sample Case History Questionnaire (TSCHQ). This higher rate of hyperacusis could be explained by the use of a less specific screening tool for hyperacusis 28.
Hyperacusis may be very invalidating with consequent social isolation, anxiety and depression. Appropriate treatment involves a multidisciplinary approach with the general practitioner, neurologist, ENT and psychologist.
Gu et al. 11 studied the sound-evoked fMRI activation in the subcortical centres such as the inferior colliculus (IC) and medial geniculate body (MGB) and in the primary auditory cortex (PAC) in people with and without tinnitus. In this study, the signal change in the fMRI in the subcortical centres was significantly correlated with ULL and a sound level tolerance questionnaire (SLTQ) score. There was little or no effect of tinnitus on the sound-evoked activation levels of these subcortical structures. In contrast to the subcortical centres, some of the cortical areas also showed an effect of tinnitus. Even in the cortical areas the correlation between the percentage signal change and STL measures was significant.
These results directly show a physiological correlate of abnormal SLT that is indicative of hyperacusis, ranging from mild to severe. This means that hyperacusis could be more directly related to tinnitus than generally appreciated.
There was no statistically significant association between DPOAE and ULL (p > 0.05), DPOAE and audiometric examination (p > 0.05), or DPOAE and gender (p > 0.05). The Spearman correlation between ULL and HQ was statistically significant (p < 0.05), (rs = 0.72). The AUC of HQ using audiometric examination as a diagnostic reference variable (AUC = 0.67 ± 0.05) was statistically significant (p < 0.05), suggesting a poor performance of the test compared to low and high ULL levels (optimal cutoff = 16, sensibility = 67.89%, specificity = 72.22%).
The OR model showed an adequate fitting (χ2 = 14.16, p < 0.05). ORgender = 0.39 ± 0.18 (p < 0.05). The odds interpretation can be that the high ULL level vs. the combined middle and low categories is less than 1, i.e. women have a lower odds of a high ULL level if hyperacusis is held constant.
ORHQ = 1.07 ± 0.03 (p < 0.05). Odds of the high category of ULL versus the low and middle categories of ULL are 1.07 times greater within each gender. Because of the proportional odds assumption the same increase, 1.07 times is found between low ULL and the combined categories of middle and high ULL.
Other factors, such as long-term stress, need to be taken in consideration when assessing hyperacusis with a questionnaire. As reported by Hasson et al., women with high levels of emotional exhaustion become more sensitive to sound after an acute stress task and have reduced thresholds to loudness. Patients with normal ULL but seeking help for hyperacusis should be assessed for emotional exhaustion with control of plasma cortisol concentration and estradiol 29 30. We also confirm, as Hasson et al. 29, that the strongest correlation was found for the social dimension of HQ. This result may suggest that social aspects revealed by the questionnaire HQ correspond best to ULL. Moreover, it was pointed out a sex-related biological difference between male and female subjects. In fact, in women with high emotional stress levels the prevalence increase of the ULL levels was more pronounced than in men 29.
In addition, many patients are unaware that their problem has a name or do not know the significance of "hyperacusis". The use of HQ represents a screening tool to evaluate the subjective distress related to hypersensitivity to sound and to guide the results of the therapy. However, the present study presents a limit in that we administered the HQ only to patients with tinnitus, while a control group of normal subjects is not present.
A future prospective will be to establish which index between audiometry, DPOAE and ULL is most predictive of hyperacusis in relation to the degree obtained with score on the HQ.
Conclusions
In our study, we found a cut-off of 16 instead of the previous cut-off of 28, described as very high by different authors. The αC in our study is also very significant and, consequently, the Italian version of the HQ should be introduced among questionnaires necessary for the classification of patients with tinnitus and intolerance to sounds, possibly using adjusted scores. Moreover, from our study, ULL was an important variable that can be discriminating in the evaluation of the hyperacusis. The HQ is a valid and easy instrument to evaluate hyperacusis, which is often undervalued in patients with hearing disorders.
Appendix 1. The Italian translation of the hyperacusis questionnaire by Khalfa S. et al., 2002.
Questionario sull'iperacusia
Cognome, Nome: _________________________________________________________ Data: _______________
Sesso: [M] [F] Età: ____________________________________________________________________________
Professione:__________________________________________________________________________________
Città di residenza:_____________________________________________________________________________
Telefono fisso / mobile:________________________________________________________________________
È stato o è esposto al rumore?___________________________________________________________________
Tollera il rumore meno bene di qualche anno fa?_____________________________________________________
Ha mai avuto problemi di udito? Se sì di che tipo? ___________________________________________________
| No | Raramente | Spesso | Sempre | |
|---|---|---|---|---|
| 1. Ha l'abitudine ad usare tappi o cuffie per ridurre la percezione del rumore (non consideri l'utilizzo di protezioni auricolari durante situazioni di anormali od elevati rumori)? | ||||
| 2. Le riesce difficile ignorare i suoni circostanti in situazioni quotidiane? | ||||
| 3. Ha difficoltà a leggere in ambienti rumorosi? | ||||
| 4. Ha difficoltà a concentrarsi in situazioni rumorose? | ||||
| 5. Ha difficoltà a seguire la conversazione in ambienti rumorosi? | ||||
| 6. Qualcuno le ha detto che tollera poco il rumore o alcuni suoni? | ||||
| 7. È particolarmente sensibile o disturbato dai rumori della strada? | ||||
| 8. Trova il rumore sgradevole in alcune situazioni sociali (night club, pub, bar, concerti, rinfreschi, spettacoli pirotecnici)? | ||||
| 9. Quando le propongono qualcosa (uscire, andare al cinema, andare ad un concerto) pensa immediatamente al rumore al quale potrà essere esposto? | ||||
| 10. Rinuncia mai ad inviti o ad uscire a causa del rumore a cui potrebbe essere esposto? | ||||
| 11. Il rumore o particolari suoni la disturbano maggiormente in un luogo silenzioso piuttosto che in presenza di un leggero rumore di fondo? | ||||
| 12. Lo stress e la stanchezza riducono la sua capacità di concentrazione in presenza di rumore? | ||||
| 13. La sua capacità di concentrazione in presenza di rumore diminuisce verso la fine della giornata? | ||||
| 14. Il rumore o alcuni suoni le causano stress od irritabilità? |
References
- 1.Moller Chen G, Lee C, et al. Behavioral evidence for possible simultaneous induction of hyperacusis and tinnitus following intense sound exposure. J Assoc Res Otolaryngol. 2013;14:413–424. doi: 10.1007/s10162-013-0375-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Minor LB, Solomon D, Zinreich JS, et al. Sound- and/or pressure-induced vertigo due to bone dehiscence of the superior semicircular canal. Arch Otolaryngol Head Neck Surg. 1998;124:249–258. doi: 10.1001/archotol.124.3.249. [DOI] [PubMed] [Google Scholar]
- 3.Modugno GC, Brandolini C. Can lateral semicircular canal dysplasia play a role in the genesis of hyperacusis. Acta Otorhinolaryngol Ital. 2014;34:71–74. [PMC free article] [PubMed] [Google Scholar]
- 4.Katzenell U, Segal S. Hyperacusis: review and clinical guidelines. Otol Neurotol. 2001;22:321–326. doi: 10.1097/00129492-200105000-00009. [DOI] [PubMed] [Google Scholar]
- 5.Baguley DM. Hyperacusis. J R Soc Med. 2003;96:582–585. doi: 10.1258/jrsm.96.12.582. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Vernon JA. Pathophysiology of tinnitus: a special casehyperacusis and a proposed treatment. Am J Otol. 1987;8:201–202. [PubMed] [Google Scholar]
- 7.Klein AJ, Armstrong BL, Greer MK, et al. Hyperacusis and otitis media in individuals with Williams syndrome. J Speech Hear Disord. 1990;55:339–344. doi: 10.1044/jshd.5502.339. [DOI] [PubMed] [Google Scholar]
- 8.Jastreboff MM, Jastreboff PJ. Decreased sound tolerance and tinnitus retraining therapy (TRT) Aust N Z J Audiol. 2002;21:74–81. [Google Scholar]
- 9.Baguley DM, McFerran DJ. Current perspective on tinnitus. Arch Dis Child. 2002;86:141–143. doi: 10.1136/adc.86.3.141. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Dauman R, Bouscau-Faure F. Assessment and amelioration of hyperacusis in tinnitus patients. Acta Otolaryngol. 2005;125:503–509. doi: 10.1080/00016480510027565. [DOI] [PubMed] [Google Scholar]
- 11.Gu JW, Halpin CF, Nam EC, et al. Tinnitus, diminished sound-level tolerance, and elevated auditory activity in humans with clinically normal hearing sensitivity. J Neurophysiol. 2010;104:3361–3370. doi: 10.1152/jn.00226.2010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Knipper M, Dijk VP, Nunes I, et al. Advances in the neurobiology of hearing disorders: Recent developments regarding the basis of tinnitus and hyperacusis. Prog Neurobiol. 2013;111:17–33. doi: 10.1016/j.pneurobio.2013.08.002. [DOI] [PubMed] [Google Scholar]
- 13.Tyler RS, Conrad-Armes D. The determination of tinnitus loudness considering the effects of recruitment. J Speech Hear Res. 1983;26:59–72. doi: 10.1044/jshr.2601.59. [DOI] [PubMed] [Google Scholar]
- 14.Hébert S, Fournier P, Noreña A. The auditory sensitivity is increased in tinnitus ears. J Neurosci. 2013;33:2356–2364. doi: 10.1523/JNEUROSCI.3461-12.2013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Jüris L, Andersson G, Larsen HC, et al. Psychiatric comorbidity and personality traits in patients with hyperacusis. Int J Audiol. 2013;52:230–235. doi: 10.3109/14992027.2012.743043. [DOI] [PubMed] [Google Scholar]
- 16.Blaesing L, Kroener-Herwig B. Self-reported and behavioral sound avoidance in tinnitus and hyperacusis subjects, and association with anxiety ratings. Int J Audiol. 2012;51:611–617. doi: 10.3109/14992027.2012.664290. [DOI] [PubMed] [Google Scholar]
- 17.Darrow KN, Maison SF, Liberman MC. Cochlear efferent feedback balances interaural sensitivity. Nat Neurosci. 2006;9:1474–1476. doi: 10.1038/nn1807. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Andersson G, Strömgren T, Ström L, et al. Randomized controlled trial of internet-based cognitive behavior therapy for distress associated with tinnitus. Psychosom Med. 2002;64:810–816. doi: 10.1097/01.psy.0000031577.42041.f8. [DOI] [PubMed] [Google Scholar]
- 19.Nelson JJ, Chen K. The relationship of tinnitus, hyperacusis, and hearing loss. Ear Nose Throat J. 2004;83:472–476. [PubMed] [Google Scholar]
- 20.Khalfa S, Dubal S, Veuillet E, et al. Psychometric normalization of a hyperacusis questionnaire. ORL J Otorhinolaryngol Relat Spec. 2002;64:436–442. doi: 10.1159/000067570. [DOI] [PubMed] [Google Scholar]
- 21.Meeus OM, Spaepen M, Ridder DD, et al. Correlation between hyperacusis measurements in daily ENT practice. Int J Audiol. 2010;49:7–13. doi: 10.3109/14992020903160868. [DOI] [PubMed] [Google Scholar]
- 22.Dauman R, Bouscau-Faure F. Assessment and amelioration of hyperacusis in tinnitus patients. Acta Otolaryngol. 2005;125:503–509. doi: 10.1080/00016480510027565. [DOI] [PubMed] [Google Scholar]
- 23.Nelting M, Rienhoff NK, Hesse G, et al. The assessment of subjective distress related to hyperacusis with a self-rating questionnaire on hypersensitivity to sound. Laryngorhinootologie. 2002;81:327–334. doi: 10.1055/s-2002-28342. [DOI] [PubMed] [Google Scholar]
- 24.Herráiz C, Santos G, Diges I, et al. Assessment of hyperacusis: the self-rating questionnaire on hypersensitivity to sound. Acta Otorrinolaringol Esp. 2006;57:303–306. doi: 10.1016/s0001-6519(06)78716-7. [DOI] [PubMed] [Google Scholar]
- 25.Kumagaya S, Ayaya S, Takenaga T, et al. Prevalence and risk factors for hyperacusis in general college students. Audiology Japan. 2013;56:234–242. [Google Scholar]
- 26.Newman CW, Wharton JA, Shivapuja BG, et al. Relationships among psychoacoustic judgments, speech understanding ability and self-perceived handicap in tinnitus subjects. Audiology. 1994;33:47–60. doi: 10.3109/00206099409072954. [DOI] [PubMed] [Google Scholar]
- 27.Goldstein B, Shulman A. Tinnitus-hyperacusis and the loudness discomfort level test. A preliminary report. Int Tin J. 1996;2:83–89. [PubMed] [Google Scholar]
- 28.Schecklmann M, Landgrebe M, Langguth B TRI Database Study Group, author. Phenotypic characteristics of hyperacusis in tinnitus. eCollection 2014.PLoS One. 2014;9:e86944–e86944. doi: 10.1371/journal.pone.0086944. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Hasson D, Theorell T, Bergquist J, et al. Acute stress induces hyperacusis in women with high levels of emotional exhaustion. PLoS One. 2013;8:e52945–e52945. doi: 10.1371/journal.pone.0052945. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Wallén MB, Hasson D, Theorell T, et al. The correlation between the hyperacusis questionnaire and uncomfortable loudness levels is dependent on emotional exhaustion. Int J Audiol. 2012;51:722–729. doi: 10.3109/14992027.2012.695874. [DOI] [PubMed] [Google Scholar]