

Abstract
Dietary patterns high in refined starches, sugar, and saturated and trans-fatty acids, poor in natural antioxidants and fiber from fruits, vegetables, and whole grains, and poor in omega-3 fatty acids may cause an activation of the innate immune system, most likely by excessive production of proinflammatory cytokines associated with a reduced production of anti-inflammatory cytokines. The Mediterranean Diet (MedDiet) is a nutritional model inspired by the traditional dietary pattern of some of the countries of the Mediterranean basin. This dietary pattern is characterized by the abundant consumption of olive oil, high consumption of plant foods (fruits, vegetables, pulses, cereals, nuts and seeds); frequent and moderate intake of wine (mainly with meals); moderate consumption of fish, seafood, yogurt, cheese, poultry and eggs; and low consumption of red meat, processed meat products and seeds. Several epidemiological studies have evaluated the effects of a Mediterranean pattern as protective against several diseases associated with chronic low-grade inflammation such as cancer, diabetes, obesity, atherosclerosis, metabolic syndrome and cognition disorders. The adoption of this dietary pattern could counter the effects of several inflammatory markers, decreasing, for example, the secretion of circulating and cellular biomarkers involved in the atherosclerotic process. Thus, the aim of this review was to consider the current evidence about the effectiveness of the MedDiet in these chronic inflammatory diseases due to its antioxidant and anti-inflammatory properties, which may not only act on classical risk factors but also on inflammatory biomarkers such as adhesion molecules, cytokines or molecules related to the stability of atheromatic plaque.
Keywords: Adhesion molecules, atheromatic plaque, atherosclerosis, cytokines, inflammation, mediterranean diet, mediterranean dietary pattern, plaque vulnerability
Introduction
The World Health Organization (WHO) recognizes that diet plays an important role in preventing non-communicable diseases. Unhealthy nutrition, as well as other adverse lifestyle health behaviors are recognized as being part of the prime factors responsible for cardiovascular disease (CVD), diabetes, malignant cancer and chronic disease of the respiratory system [1].
Epidemiological studies such as the Seven Countries Study in the 60s [2] demonstrated a great interest in the Mediterranean diet (MedDiet) as a healthy eating pattern. These epidemiological studies have shown that high adherence to traditional MedDiet was associated with a lower mortality and cardiovascular disease incidence, reducing the risk of developing the metabolic syndrome, type 2 diabetes, and some neurodegenerative diseases and cancers [3].
The MedDiet is a nutritional model inspired by the traditional dietary pattern of some of the countries of the Mediterranean basin. At least 16 countries border the Mediterranean Sea. Diets vary between these countries and also between regions within the same country. Many differences in culture, ethnic background, religion, economy and agricultural productions result in different diets, but the common Mediterranean dietary pattern (MDP) gather the following characteristics: abundant consumption of olive oil and high consumption of fruits, vegetables, cereals (preferably as whole grain), legumes, nuts and seeds. The MDP also includes moderate consumption of fish and shellfish, white meat, eggs, and fermented dairy products (cheese and yogurt), as well as relatively small amounts of red meat, processed meats, and foods rich in sugars. Frequent but moderate intake of wine, especially red wine with meals is also recommended [4, 5]. The MedDiet is characterized by a relatively high fat intake (40%–50% of total daily calories), of which saturated fatty acids (SFA) comprises ≤ 8% and monounsaturated fatty acids (MUFA), mainly from olive oil, between 15%–25% of calories. It is characterized by a high omega-3 fatty acid intake from fish and plant sources and a low Omega-6:Omega-3 ratio of 2:1–1:1 compared to 14:1 in Europe [4, 6]. High consumption of dietary fiber [7], low glycemic index and glycemic load [8], anti-inflammatory effects [9], and antioxidant compounds [10, 11] may act together to produce favorable effects on health status.
Effects of the Mediterranean Diet on Inflammation
Dietary patterns high in refined starches, sugar, and saturated and trans-fatty acids, poor in natural antioxidants and fiber from fruits, vegetables, and whole grains, and poor in omega-3 fatty acids may cause an activation of the innate immune system, most likely by excessive production of proinflammatory cytokines associated with a reduced production of anti-inflammatory cytokines.
Chronic disease risk links behavioral factors and obesity through an underlying pathophysiological mechanism, that is, chronic low-grade inflammation. Elevated levels of inflammatory biomarkers such as C-reactive protein (CRP), interleukin (IL) 6 and 18, fibrinogen, and adhesion molecules (e.g., E-selectin, intercellular adhesion molecule 1 (ICAM-1), and vascular cell adhesion protein 1 (VCAM-1) sustain evidence of a central role of inflammation in CVD, type 2 diabetes or cancer. In contrast, concentrations of anti-inflammatory adipokine adiponectin were inversely associated with CVD, type 2 diabetes, and obesity-related cancer [12, 13]. Thus, the MedDiet could be used as dietary therapy for chronic low-grade inflammation-related diseases (Fig. 1).
Fig. (1).
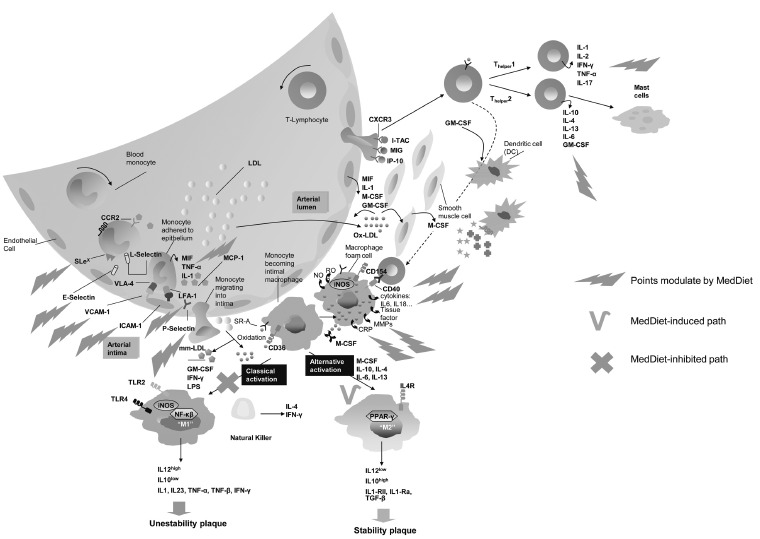
Modulation of the Mediterranean diet on the immune factors providing protective effect against cardiovascular disease or cancer. Accumulation of oxidised low-density lipoprotein (oxLDL), starting in the fatty streaks, promotes the inflammatory response. Oxidized lipids and oxLDL trigger the expression of adhesion molecules (VCAM-1, mainly) and other mediators such as selectins and integrins, promoting the recruitment of monocytes into the subendothelial space in response to chemo-attractant cytokines. Successive accumulation of apoptotic cells, debris and cholesterol crystals form a necrotic core. Macrophages can be either classically activated (M1) or alternatively activated (M2). M1 monocytes display pro-inflammatory activity and could promote plaque vulnerability while, M2 monocytes are associated with homeostatic activity but could be pro-atherogenic in the early stages while promoting plaque stability in the later stages. Finally, in late stages atheromatic plaque may become unstable, leading to cap rupture, ensuing thrombosis and finally, cardiovascular events. The MedDiet exerts an anti-inflammatory and a modulating effect on CRP, interleukins such as IL-1, IL-6 as well as on TNF-α and its receptors, or chemoattractant molecules as MCP-1 or soluble adhesion molecules (sVCAM-1, sICAM-1, sE- and sP-Selectin). MedDiet triggers the alternative activation and exerts an immunomodulatory effect on biomarkers related to plaque stability such as IL-18, MMP-9 or TGF-β. It also can regulate the expression of leukocyte adhesion molecules including SLex, VLA-4 and LFA. IL-: interleukins; MMP-9: Metalloprotease-9; TNF-α: Tumor necrosis factor; TGF-β1: Transforming Growth Factor-β1; sVCAM-1: soluble vascular cell adhesion molecule; sICAM-1: Soluble intercellular adhesion molecule-1; sP-Selectin: Soluble platelet selectin; sE-Selectin: soluble endothelial selectin. Figure adapted [27, 28, 75, 76].
Mediterranean diet and Cardiovascular disease
Since the turn of the 21st century, coronary heart disease (CHD) has been a major cause of death and disability in Western countries, although the incidence varies according to geographical origin, with Mediterranean countries and Japan showing the lowest rates worldwide [14]. Geographical differences in CHD rates are attributable, in part, to dietary and other lifestyle habits. Several epidemiological studies have reported that high adherence to the MedDiet is associated with a lower incidence of CHD and mortality rates [15-17].
Up to now, the beneficial effect of the MedDiet against CVD has been attributed to its effects in controlling classical risk factors. Thus, several clinical studies have shown that Mediterranean-style diets are protective against the development of prevalent diseases that promote CHD, such as the metabolic syndrome [18], diabetes [19], hypertension [20] or dyslipidemia [21]. Recently, some authors have suggested that an anti-inflammatory effect in the vascular wall may be another important mechanism to explain the link between the MedDiet and low cardiovascular mortality [22]. Indeed, additional evidence from clinical trials have suggested that the MedDiet reduces vascular inflammation [22], oxidative stress [23], and endothelial dysfunction [24, 25], which are factors involved in the development of atherosclerosis. Interestingly, it has also been reported that the MedDiet can favorably modulate the expression of pro-atherogenic genes [26].
The effects of Inflammation on Atherosclerotic Disease
Atherosclerosis is a chronic inflammatory disorder of the vessel wall and involves accumulation of lipids in the arterial intima which leads to formation of vascular lesions, or atheromatic plaque [27]. Monocytes and T-cells are implicated in this atherogenic process, migrating from the circulation into the intima of the arterial wall where they are differentiated into macrophages and later into foam cells after joining oxidized low-density lipoprotein (oxLDL) [28, 29]. This process triggers an activation of endothelial cells, because of the accumulation of modified LDL. Activated endothelial cells upregulate adhesion molecule expression (VCAM-1, mainly) and other mediators such as selectins, integrins, promoting the recruitment of monocytes into the subendothelial space in response to chemo-attractant cyotkines [29]. The recruitment of immune cells is a crucial early step in atherogenesis. Macrophages and T-lymphocytes together release a wide array of chemokines and cytokines that can exert both pro- and antiinflammatory effects [28]. C-reactive protein (CRP), tumor necrosis factor (TNF)-α, or pro-inflammatory cytokines such as interleukin-6 (IL-6) are associated with the development of atherosclerosis. Finally, in late stages atheromatic plaque may become unstable, leading to cap rupture, ensuing thrombosis and finally, cardiovascular events [30]. In this context, some circulating molecules, such as matrix metalloprotease-9 (MMP-9) or interleukin-18 (IL-18), are considered to be early biomarkers of plaque vulnerability [31].
Several anti-inflammatory mechanisms have been proposed correlating the MedDiet and/or its components with the different steps of atherosclerotic process. Therefore, circulating markers of inflammation, such as CRP, TNF-α, and some interleukins (IL-6, IL-18) may be correlated with the development of vascular events and, in some cases, also contribute to their pathogenesis. On the other hand, adiponectin (protein that originates from adipose tissue) also exhibits potent anti-inflammatory and antiatherosclerotic effects. Therefore, low plasma adiponectin levels are an independent risk factor for the future development of type 2 diabetes, whereas high plasma adiponectin concentrations are associated with a lower risk of myocardial infarction in men. Finally, it has become increasingly clear that inflammation strictly correlates with endothelial dysfunction and insulin resistance [13].
Immunomodulatory effects of the Mediterranean Diet
Experimental and clinical studies have shown that olive oil down-regulates the expression of VCAM-1, ICAM-1, and E-selectin in circulating lymphocytes and monocytes [32] and decreases plasma concentrations of sICAM-1, sVCAM-1, sE-selectin, IL-6, and CRP in high-risk patients [33, 34]. The observational ATTICA study evaluated 1,514 Greek men and 1,528 women. This study showed that greater adherence to a Mediterranean-style diet was associated with 20% lower CRP and 17% lower IL-6 compared with those in the lowest tertile of adherence [35]. In the Nurses’ Health Study, a Mediterranean diet index score was associated with lower concentrations of biomarkers of inflammation and endothelial dysfunction (CRP, IL6, ICAM-1 and VCAM-1) [36]. A pattern similar to a MDP was inversely associated with plasma CRP and E-selectin concentrations, whereas a Western pattern, with a higher intake of red meat, sweets, fries and refined grains, was positively associated with CRP, IL-6, E-selectin, ICAM-1 and VCAM-1 concentrations [37]. A recent meta-analysis including a total 17 of trials reported that greater adherence to the MedDiet was associated with a significantly greater reduction in IL-6 and CRP compared to control intervention protocols, improving endothelial function [38]. In addition, a group of patients with metabolic syndrome following a MedDiet pattern showed reduced serum concentrations of CRP, IL-6, IL-7 and IL-18, decreased insulin resistance and improved endothelial function [22].
Other studies such as that by Llorente-Cortés et al. showed an increase of cyclooxygenase 2 (COX-2) and LDL-C receptor related protein, representing a decrease in the expression of monocyte chemoattractant protein 1 (MCP-1) in 49 asymptomatic individuals with high CVD risk after a 3-month intervention with the MedDiet [26]. Furthermore, the MedDiet can also exert a modulation effect on the expression of genes related to plaque stability, such as MMP-9, even in an elderly high-risk population and after a short period [39]. In addition, the MedDiet acts by improving endothelial dysfunction in healthy elderly individuals after 4-weeks of consumption, increasing the production of endothelial progenitor cells and decreasing the release of endothelial microparticles [40]. The inflammatory markers upon which the MedDiet acts are shown in Table 1.
Table 1. Protective effects of the MedDiet on immune factors.
| Mediterranean Diet | ||||||
|---|---|---|---|---|---|---|
| Immune Factors | ||||||
| Interleukins & CRP | Tumor Necrosis Factor & Receptors | Tumor Necrosis Factor & Receptors | Chemokines | Stability / Unstability of Atheromatic Plaque | Circulating Adhesion Molecules | Leukocyte Adhesion Molecules |
| IL-1 | TNF-α | MMP-9 | sICAM | CD11a | ||
| Il-6 | TNFR60 | TGF-β1 | MCP-1 | TIMP-1 | sVCAM-1 | CD11b |
| IL-7 | TNFR80 | IL-10 | sP-Seletin | CD49d | ||
| CRP | IL-18 | sE-Selectin | CD40 | |||
To date, the PREDIMED study (Prevención con Dieta Mediterránea) is the only randomized trial that has evaluated the protective effect of a MDP supplemented with extra virgin olive oil (EVOO) or nuts versus a low-fat diet (LFD) in patients at high risk for CVD and the possible mechanisms involved in this protection. This large interventional study, including 7,447 subjects, showed that a MedDiet rich in olive oil or nuts reduces the risk of CVD by 30% when compared to a low-fat diet [41]. This study has also demonstrated that adherence to the MedDiet is associated with a reduced incidence of diabetes [19, 42], metabolic syndrome [43], hypertension [44], cardiovascular risk factors [9], oxidative stress [45], vascular inflammation [46-48], and endothelial dysfunction [23], all of which are factors involved in atheromatic plaque development. In the pilot study of the PREDIMED trial [9], we analyzed the effects of the MedDiet rich in olive oil or nuts and a LFD on 4 soluble adhesion molecules (ICAM-1, VCAM-1, IL-6 and CRP) on the first 772 participants recruited and after a 3-month follow up. In the short-term, plasma concentrations of IL-6, VCAM-1 and ICAM-1 decreased in the MedDiet groups supplemented with olive oil and nuts, while plasma concentrations of CRP only decreased in the MedDiet supplemented with EVOO (P < 0.05; all). Otherwise, plasma concentrations of VCAM-1 and ICAM-1 increased after 3 months in the LFD group (P < 0.05; both). In another sub-study of the PREDIMED trial, we demonstrated the anti-inflammatory effects of the MedDiet on circulating inflammatory biomarkers and immune cell activation biomarkers, all related to the atherosclerotic process, after a 3-month intervention [46]. We analyzed 106 subjects at high risk for CVD. We assessed changes in cellular and serum inflammatory biomarkers from baseline. Both MedDiets supplemented with EVOO or nuts showed down-regulated monocyte expression of CD49d and CD40 (P<0.05) after 3-months with the dietary intervention. Likewise, in this sub-study we also analyzed the changes in plasma concentrations of ICAM-1, VCAM-1, IL-6, E- and P-Selectin before and after 3 months. The results showed that both MedDiets reduced ICAM-1 levels whereas VCAM-1, IL-6 and CRP decreased only for the MedDiet+VOO (P<0.05). Since this had not been previously investigated, this study was a breakthrough for knowing the effects of the Med-Diet on adhesion molecule expression on circulating peripheral blood mononuclear cells linked to the development of atherosclerosis.
CRP C-reactive protein; sVCAM-1: soluble vascular cell adhesion molecule; sICAM-1: Soluble intercellular adhesion molecule-1; sP-Selectin: Soluble platelet selectin; sE-Selectin: soluble endothelial selectin; TNFR, TNF receptor; ; MMP-9: Metalloprotease-9 ; TNF-α: Tumor necrosis factor; TGF-β1:Transforming Growth Factor-β1; IL-: interleukins; TIMP-1: metalloproteinase inhibitor 1.
In a third sub-study of the PREDIMED trial [48], we analyzed the effects of 2 MedDiets (MedDiet+VOO and MedDiet+Nuts) and a LFD on 4 circulating inflammatory biomarkers related to atherogenesis (TNFR60, TNFR80, ICAM-1 and IL-6) in a total of 516 participants after a 1-year intervention. It is known that the activation of TNFR60 can induce the expression of adhesion molecules and activate NF-κβ, and TNFR80 which play a role in T cell proliferation [49]. Thus, at baseline and after 1 year (Table 2), the MedDiet groups had lower plasma concentrations of IL-6, TNFR60, and TNFR80 (P < 0.05;all), whereas ICAM-1, TNFR60, and TNFR80 concentrations increased in the LFD group (P < 0.005;all). For the first time it was possible to link a diminution in TNFR concentrations with a MDP.
Table 2. Changes in the expression of circulating markers of plaque instability and other inflammatory biomarkers in the short- and long-term.
| Inflammatory Molecules | Short-term | Long-term | ||||
|---|---|---|---|---|---|---|
| MedDiet+ EVOO | MedDiet+ Nuts | Low-fat diet | MedDiet+ EVOO | MedDiet+ Nuts | Low-fat diet | |
| sICAM-1, ng/mL | ↓ | ↓ | ↑ | ↓ | = | ↑ |
| sVCAM-1, ng/mL | ↓ | ↓ | ↑ | ↓ | ↓ | = |
| sE-Selectin, ng/mL | = | = | = | = | ↓ | = |
| sP-Selectin, ng/mL | = | = | = | ↓ | ↓ | = |
| IL-6, pg/mL | ↓ | ↓ | ↑ | ↓ | ↓ | ↑ |
| CRP, mg/L | ↓ | = | = | ↓ | ↓ | = |
| TNFR60, μg/L | ↓ | ↓ | ↑ | |||
| TNFR80, μg/L | ↓ | ↓ | ↑ | |||
| IL-18, pg/mL | = | ↓ | = | |||
| IL-10, pg/mL | = | = | = | |||
| IL-18/IL-10 ratio | ↓ | ↓ | = | |||
| MMP-9, ng/mL | = | = | ↑ | |||
| TIMP-1, ng/mL | = | = | = | |||
| MMP-9/TIMP-1 ratio | = | = | ↑ | |||
| TGF-β1, pg/mL | = | = | ↑ |
To date, data on the possible anti-inflammatory role of the MedDiet are scarce and are mainly based on observational studies [50] or short-term intervention studies [46]. In addition, serum markers related to plaque vulnerability have also been associated with cardiovascular events. Thus, high levels of MMP-9, a protease that can degrade the fibrous content of plaque and facilitate its rupture, have previously been detected in patients with acute coronary syndromes [51] or those with ulcerated plaque identified on coronary angiography [52], compared to healthy controls. Likewise, increased levels of TIMP-1 are related to a high risk of cardio- and cerebrovascular events [53], and IL-18 has been considered to be a predictor of myocardial infarction and death in patients with angina [54]. Finally, higher levels of TGF-β1 were observed in the control diet group, but there is no consensus on whether they are related to plaque stabilization [55].
Finally, a fourth study [47] made by our group showed that adherence to the MedDiet is associated with an increase in serum markers of atheromatic plaque stability which may explain, at least in part, the protective role of MedDiet against CVD. In this case, a total of 164 participants at high risk for cardiovascular disease were randomized into one of the three diet groups described previously. Then, we assessed the 12-month effects of two enhanced MedDiets compared to a LFD on the adhesion molecules for T-Lymphocytes and monocytes (CD11a, CD11b, CD49d and CD40), as well as inflammatory biomarkers related to atherosclerosis (sVCAM-1, sICAM-1, sE- and sP-selectin) and plaque vulnerability (CRP, IL-6, IL-18, IL-10, TGF-β1, MMP-9). As shown in Table 3, some anti-inflammatory effects were detected in the three diets studied, although they were more intense in subjects allocated to the two MedDiet interventions, supplemented with VOO and nuts, which showed a higher down-regulation of adhesion molecules in T-lymphocytes and monocytes compared to those in the control diet group. Moreover, serum levels of endothelial cell adhesion molecules were lower in subjects following both MedDiets, compared to control subjects, in whom some inflammatory molecules (e.g., sICAM-1) showed a significant increase. Likewise, parameters directly related to plaque vulnerability, such as IL-18, MMP-9, TIMP-1, TGF-β1, and IL-10 had a more favorable profile (towards stability) in participants in the MedDiet+nuts than those in the control group (Table 2). All these changes slow lymphocyte and monocyte adhesion to the endothelium and posterior transmigration to the subendothelial space to generate unstable plaque. Moreover, Casas et al. [47], observed a significant decrease in systolic and dyastolic BP and in plasma total-cholesterol concentrations in both MedDiet groups compared to the control group. The anti-inflammatory effect of the MedDiet seems to be greater and more intense in the mid-term compared to the short-term [46], while the effect on classical cardiovascular risk factors is similar, thereby suggesting that the MedDiet exerts its effects on lipids and blood pressure relatively quickly (at 3 mo), with the maximum effect on systemic inflammatory biomarkers being achieved later (at 1 y). Thus, in the short-term the effect on blood pressure and the lipid profile is higher, whereas in the mid-term the effect on chronic inflammatory response in the arterial wall is more pronounced. In brief, the results of this study suggest that the MedDiet, enriched with EVOO or nuts, may have a dual effect on the prevention of CVD: improving classical cardiovascular risk factors and having an intense anti-inflammatory effect.
Table 3. Changes in adhesion molecule expression in circulating T- lymphocytes and monocytes.
| Short-term | Long-term | |||||
|---|---|---|---|---|---|---|
| MedDiet+ EVOO | MedDiet+ Nuts | Low-fat diet | MedDiet+ EVOO | MedDiet+ Nuts | Low-fat diet | |
| T-LYMPHOCYTES | ||||||
| CD11a | = | = | = | ↓ | ↓ | ↓ |
| CD49d | ↓ | ↓ | = | ↓ | = | = |
| CD40 | = | = | = | ↓ | ↓ | = |
| MONOCYTES | ||||||
| CD11a | = | ↓ | = | ↓ | ↓ | ↓ |
| CD11b | ↓ | ↓ | = | ↓ | ↓ | ↓ |
| CD49d | ↓ | ↓ | = | ↓ | ↓ | = |
| CD40 | ↓ | = | = | ↓ | ↓ | = |
CRP, high-sensitivity C-reactive protein; EVOO, extra virgin olive oil; LFD, low-fat diet; MedDiet+EVOO, Mediterranean diet supplemented with extra virgin olive oil; MedDiet +Nuts, Mediterranean diet supplemented with nuts; IL-: interleukins; sVCAM-1: soluble vascular cell adhesion molecule; sICAM-1: Soluble intercellular adhesion molecule-1; sP-Selectin: Soluble platelet selectin; sE-Selectin: soluble endothelial selectin.; MMP-9: Metalloprotease-9; TNF-α: Tumor necrosis factor; TGF-β1: Transforming Growth Factor-β1; TNFR, TNF receptor; TIMP-1: metalloproteinase inhibitor 1; “↑”: increased plasma levels of biomarkers; “↓”: decreased plasma levels of biomarkers; “=”: no changes observed in the levels of the biomarkers.
MEDITERRANEAN DIET AND CANCER
Cancer involves a series of diseases caused primarily by exposure to environmental factors, habits and lifestyle, and is, thus, largely preventable. The MedDiet is based mainly on the consumption of plant foods, providing a high content of vitamins and antioxidants involved in cellular differentiation and proliferation in the synthesis and repair of DNA adduct formation and inhibition of the formation of carcinogenic chemicals in inflammatory response, enzyme induction and hormonal activity [56].
Since the late 50s and early 60s there is greater and growing evidence that greater adherence to a MDP is associated with a lower incidence of chronic diseases like CVD, type 2 diabetes, obesity, metabolic syndrome and certain types of cancer, as well as increased survival and longevity [5]. Several epidemiological studies have evaluated the causal relationship between the MedDiet and cancer risk. Thus, from the Seven Countries Study in the 1950s to the recent European Prospective Study and to Cancer and Nutrition (EPIC) study collaboration, the evaluation of the components of diet-affecting chronic diseases such as cardiovascular disease and cancer has been crucially based on the analysis of foods and nutrients characterizing the Mediterranean dietary habits. Ongoing findings from the EPIC study (Greek cohort: n=23,349 men and women, not previously diagnosed with cancer and with a mean follow-up time of 8.5 years), showed that greater adherence to a MedDiet was related to a significant reduction in total mortality [13]. On the other hand, the whole EPIC study (142,605 men and 335,873 women) demonstrated that 4.7% of cancers in men and 2.4% in women might have been avoided if patients had had greater adherence to the MDP [57]. Other studies such as SUVIMAX (Suppléments in Vitamines, et Mineraux Antioxidants) have shown that to stay the risk of various cancers, the best prevention is a rich and varied diet of fruits and vegetables [58, 59]. According to the World Cancer Research Foundation, of 130,000 cancer deaths per year between 30-40% could have been prevented with the right diet [60]. Finally, a meta-analysis that included 12 studies with a total of 1,574,299 participants concluded that the 2-point increase in Mediterranean diet adherence (distributed between 0-9 points) was associated with a 6% decrease in mortality from cancer [61]. These same authors have more recently published an update of the meta-analysis cited, including the latest available works which confirm these findings [16]. When the different types of cancer are considered, a case-control study in Greece showed that a greater adherence to a MedDiet was related to a reduced risk of upper aerodisgestive tract cancers [62]. Likewise, another study found a reduction in the risk of prostatic cancer for those individuals that followed a MedDiet compared with those following a Western diet [63].
EVOO; extra virgin olive oil; MedDiet+EVOO; Mediterranean diet supplemented with extra virgin olive oil; MedDiet +Nuts; Mediterranean diet supplemented with nuts. “↑”: increased expression of adhesion molecules; “↓”: decreased expression of adhesion molecules; “=”: no changes observed in the expression of the adhesion molecules.
Possible Biological Mechanisms Against Cancer
As we have already mentioned, the MedDiet is considered a healthy dietary pattern, a cultural model and a lifestyle of certain countries of the Mediterranean coast. It is characterized by a high intake of olive oil, vegetables, fruits, legumes, and complex carbohydrates with a moderate consumption of fish, and a low-to-moderate amount of red wine during meals [4]. Thus, the increased quantity and quality of phytochemicals (such as vitamin C and E, folate, carotenoids and polyphenols) contained by the MedDiet could contribute to these beneficial effects due to their antioxidant and anti-inflammatory propierties. These antioxidant compounds act in cell differentiation and proliferation, as well as in synthesis and DNA repair processes by inhibiting the endogenous formation of carcinogenic chemicals and reducing the formation of adducts in DNA [56]. Animal studies of induced breast cancer have shown that diets rich in extra virgin olive oil (EVOO) may inhibit proliferation, induce apoptosis, and minimize DNA damage [64]. A case-control study [65] including 255 newly diagnosed breast-cancer female patients (56 ± 12 yr) and 250 1-to-1 age-matched with the control patients was evaluated and showed an association between adherence to the MedDiet and its inherent constituents, with breast-cancer.
On the other hand, the MedDiet is also characterized by low consumption of red and processed meats. The latest studies have shown that a high consumption of red meat is associated with an increased risk of colorectal [66] and gastric cancer [67].
Mediterranean diet and Neurodegene- rative diseases
Alzheimer ’s disease (AD) is the main cause of dementia among people age 65 and older and currently affects more than 25 million people in the world. AD is characterized by a progressive neurodegenerative disorder associated with cognitive impairment and neuronal cell loss, and the pathology is characterized by the presence of several kinds of amyloid plaques and neurofibrillary tangles in the brain of AD patients. The end result is memory loss as well as personality changes [69]. It is known that AD and Parkinson's disease are two of the most common neurodegenerative diseases. In both cases, only a small percentage of cases are due to genetic mutations, although studies are now uncovering interactions with genetic and environmental factors. Animal studies have shown that dietary changes can disrupt the pattern of DNA methylation [70]. At present, APOEε4 is the only validated genetic risk factor for sporadic AD [69]. However, various non-genetic risk factors seem to be implicated in the pathophysiology of sporadic AD: brain trauma, cardiovascular diseases, stroke or transient ischemic attack, carotid atherosclerosis, and clinical history of hypertension, hypercholesterolemia and/or type-II diabetes.
Thus, higher adherence to a MedDiet has been associated with reduced cognitive decline and a protection against depression independently of the age of the patient [68]. Similarly, foods, and micro-, and macronutrients contained in the MedDiet seem to have a protective effect against dementia and pre-dementia syndromes [16, 71]. A recent meta-analysis showed that greater adherence to the MedDiet reduced cognitive impairment such as that in dementia or AD [72].
Possible Biological Mechanisms against Neuro- degenerative Diseases
Several observational studies have consistently shown a protective effect of vitamin E against neurodegenerative diseases such as AD. Nevertheless, these data run counter to those shown by a recent meta-analysis in which there seems to be no evidence related to patients with AD or mild cognitive impairment [73]. Regarding fatty acids, intake of saturated fatty acids seems to increase the risk of AD. In contrast, epidemiological evidence suggests a possible association between fish consumption, monounsaturated fatty acids, and polyunsaturated fatty acids omega-3, and reduced risk of cognitive decline and dementia. However, the current evidence about light to moderate alcohol intake is only suggestive of a protective effect for vascular dementia, cognitive decline, and AD [70, 74]. However, furthers studies are needed to know better the mechanisms by which nutrients, foods and dietary patterns may act on cognition mechanisms.
CONCLUDING REMARKS
In summary, the results of several studies suggest that the MedDiet may have a dual effect on the prevention of CVD, improving classical cardiovascular risk factors and also having an intense anti-inflammatory effect. In fact, epidemiological studies have shown that the MedDiet may exert its effect partly through mechanisms such as improved lipid profile and reductions in blood pressure or insulin resistance. Its anti-inflammatory effect seems to be greater and more intense in the mid-term compared to the short-term while the effect on classical cardiovascular risk factors is similar, thereby suggesting that the MedDiet exerts its effects on lipids and blood pressure relatively quickly (at 3 mo), with the maximum effect on systemic inflammatory biomarkers being achieved later (at 1 y). Thus, in the short-term the effect on blood pressure and the lipid profile is higher, whereas in the mid-term the effect on chronic inflammatory response in the arterial wall is more pronounced.
The present review also provides evidence that a MDP alone or one enriched with some of its main components (i.e. extra virgin olive oil and nuts), not only diminishes the classical cardiovascular risk factors, but is also associated with important reductions in circulating inflammatory biomarkers, cellular inflammatory biomarkers and improves endothelial dysfunction. Moreover, increased consumption of antioxidant-rich foods as in a MDP in general and of polyphenols in particular was associated with better cognitive performance in an elderly cohort at high cardio- vascular risk.
Therefore, the choice of a healthy diet such as the MedDiet associated with regular physical activity is critical in the fight against many chronic diseases. The protection against atherosclerosis by the MedDiet can probably be extended to other chronic inflammation-related diseases, including visceral obesity, the metabolic syndrome, and type-2 diabetes, cancer or neurodegenerative diseases, among others.
ACKNOWLEDGEMENTs
CIBER OBN is an initiative of the Instituto de Salud Carlos III, Spain.
CONFLICT OF INTEREST
The author(s) confirm that this article content has no conflict of interest.
REFERENCES
- 1.Gotsis E., Anagnostis P., Mariolis A., Vlachou A., Katsiki N., Karagiannis A. Health Benefits of the Mediterranean Diet: An Update of Research Over the Last 5 Years. Angiology. 2014. [DOI] [PubMed]
- 2.Keys A. Coronary heart disease; serum cholesterol; and the diet. Acta Med. Scand. 1980;207(3):153–160. doi: 10.1111/j.0954-6820.1980.tb09697.x. [DOI] [PubMed] [Google Scholar]
- 3.Serra-Majem L., Roman B., Estruch R. Scientific evidence of interventions using the Mediterranean diet: a systematic review. Nutr. Rev. 2006;64(2 Pt 2):S27–S47. doi: 10.1111/j.1753-4887.2006.tb00232.x. [DOI] [PubMed] [Google Scholar]
- 4.Trichopoulou A., Lagiou P. Healthy traditional Mediterranean diet: an expression of culture; history; and lifestyle. Nutr. Rev. 1997;55(11 Pt 1):383–389. doi: 10.1111/j.1753-4887.1997.tb01578.x. [DOI] [PubMed] [Google Scholar]
- 5.Castro-Quezada I., Román-Viñas B., Serra-Majem L. The Mediterranean diet and nutritional adequacy: a review. Nutrients. 2014;6(1):231–248. doi: 10.3390/nu6010231. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Kris-Etherton P., Eckel R.H., Howard B.V., St. Jeor S., Bazzarre T.L. Lyon Diet Heart Study: Benefits of a Mediterranean-Style; National Cholesterol Education Program/ American Heart Association Step I Dietary Pattern on Cardiovas- cular Disease. Circulation. 2001;103(13):1823–1825. doi: 10.1161/01.cir.103.13.1823. [DOI] [PubMed] [Google Scholar]
- 7.Estruch R., Martinez-Gonzalez M.A., Corella D., Basora-Gallisa J., Ruiz-Gutierrez V., Covas M.I., Fiol M., Gómez-Gracia E. [DOI] [PubMed]; López-Sabater M.C., Escoda R., Pena M.A., Diez-Espino J., Lahoz C., Lapetra J., Sáez G., Ros E., PREDIMED Study Investigators Effects of dietary fibre intake on risk factors for cardiovascular disease in subjects at high risk. J. Epidemiol. Community Health. 2009;63(7):582–588. doi: 10.1136/jech.2008.082214. [DOI] [PubMed] [Google Scholar]
- 8.Vasto S., Scapagnini G., Rizzo C., Monastero R., Marchese A., Caruso C. Mediterranean diet and longevity in Sicily: survey in a Sicani Mountains population. Rejuvenation Res. 2012;15(2):184–188. doi: 10.1089/rej.2011.1280. [DOI] [PubMed] [Google Scholar]
- 9.Estruch R., Martínez-González M.A., Corella D., Salas-Salvadó J., Ruiz-Gutiérrez V., Covas M.I., Fiol M., Gómez-Gracia E., López-Sabater M.C., Vinyoles E., Arós F., Conde M., Lahoz C., Lapetra J., Sáez G., Ros E., PREDIMED Study Investigators Effects of a Mediterranean-style diet on cardiovascular risk factors: a randomized trial. Ann. Intern. Med. 2006;145(1):1–11. doi: 10.7326/0003-4819-145-1-200607040-00004. [DOI] [PubMed] [Google Scholar]
- 10.Visioli F., Grande S., Bogani P., Galli C. The role of antioxidants in the mediterranean diets: focus on cancer. Eur. J. Cancer Prev. 2004;13(4):337–343. doi: 10.1097/01.cej.0000137513.71845.f6. [DOI] [PubMed] [Google Scholar]
- 11.Pitsavos C., Panagiotakos D.B., Tzima N., Chrysohoou C., Economou M., Zampelas A., Stefanadis C. Adherence to the Mediterranean diet is associated with total antioxidant capacity in healthy adults: the ATTICA study. Am. J. Clin. Nutr. 2005;82(3):694–699. doi: 10.1093/ajcn.82.3.694. [DOI] [PubMed] [Google Scholar]
- 12.Barbaresko J., Koch M., Schulze M.B., Nöthlings U. Dietary pattern analysis and biomarkers of low-grade inflammation: a systematic literature review. Nutr. Rev. 2013;71(8):511–527. doi: 10.1111/nure.12035. [DOI] [PubMed] [Google Scholar]
- 13.Giugliano D., Ceriello A., Esposito K. The effects of diet on inflammation: emphasis on the metabolic syndrome. J. Am. Coll. Cardiol. 2006;48(4):677–685. doi: 10.1016/j.jacc.2006.03.052. [DOI] [PubMed] [Google Scholar]
- 14.Lloyd-Jones D., Adams R., Carnethon M., De Simone G., Ferguson T.B., Flegal K., Ford E., Furie K., Go A., Greenlund K., Haase N., Hailpern S., Ho M., Howard V., Kissela B., Kittner S., Lackland D., Lisabeth L., Marelli A., McDermott M., Meigs J., Mozaffarian D., Nichol G., O'Donnell C., Roger V., Rosamond W., Sacco R., Sorlie P., Stafford R., Steinberger J., Thom T., Wasserthiel-Smoller S., Wong N., Wylie-Rosett J., Hong Y. Heart disease and stroke statistics--2009 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2009;119(3):480–486. doi: 10.1161/CIRCULATIONAHA.108.191259. [DOI] [PubMed] [Google Scholar]
- 15.Mente A., de Koning L., Shannon H.S., Anand S.S. A systematic review of the evidence supporting a causal link between dietary factors and coronary heart disease. Arch. Intern. Med. 2009;69(7):659–669. doi: 10.1001/archinternmed.2009.38. [DOI] [PubMed] [Google Scholar]
- 16.Sofi F., Abbate R., Gensini G.F., Casini A. Accruing evidence on benefits of adherence to the Mediterranean diet on health: an updated systematic review and meta-analysis. Am. J. Clin. Nutr. 2010;92(5):1189–1196. doi: 10.3945/ajcn.2010.29673. [DOI] [PubMed] [Google Scholar]
- 17.Kontogianni M.D., Panagiotakos D.B. Dietary patterns and stroke: A systematic review and re-meta-analysis. Maturitas. 2014;79(1):41–47. doi: 10.1016/j.maturitas.2014.06.014. [DOI] [PubMed] [Google Scholar]
- 18.Kastorini C-M., Milionis H.J., Esposito K., Giugliano D., Goudevenos J.A., Panagiotakos D.B. The effect of Mediterranean diet on metabolic syndrome and its components: a meta-analysis of 50 studies and 534,906 individuals. J. Am. Coll. Cardiol. 2011;57(11):1299–1313. doi: 10.1016/j.jacc.2010.09.073. [DOI] [PubMed] [Google Scholar]
- 19.Salas-Salvadó J., Bulló M., Babio N., Martínez-González M.Á., Ibarrola-Jurado N., Basora J., Estruch R., Covas M.I., Corella D., Arós F., Ruiz-Gutiérrez V., Ros E., PREDIMED Study Investigators Reduction in the incidence of type 2 diabetes with the Mediterranean diet: results of the PREDIMED-Reus nutrition intervention randomized trial. Diabetes Care. 2011;34(1):14–19. doi: 10.2337/dc10-1288. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Doménech M., Roman P., Lapetra J., García de la Corte F.J., Sala-Vila A., de la Torre R., Corella D., Salas-Salvadó J., Ruiz-Gutiérrez V., Lamuela-Raventós R.M., Toledo E., Estruch R., Coca A., Ros E. Mediterranean Diet Reduces 24-Hour Ambulatory Blood Pressure; Blood Glucose; and Lipids: One-Year Randomized; Clinical Trial. Hypertension. 2014 doi: 10.1161/HYPERTENSIONAHA.113.03353. [DOI] [PubMed] [Google Scholar]
- 21.Vincent-Baudry S., Defoort C., Gerber M., Bernard M-C., Verger P., Helal O., Portugal H., Planells R., Grolier P., Amiot-Carlin M.J., Vague P., Lairon D. The Medi-RIVAGE study: reduction of cardiovascular disease risk factors after a 3-mo intervention with a Mediterranean-type diet or a low-fat diet. Am. J. Clin. Nutr. 2005;82(5):964–971. doi: 10.1093/ajcn/82.5.964. [DOI] [PubMed] [Google Scholar]
- 22.Esposito K., Marfella R., Ciotola M., Di Palo C., Giugliano F., Giugliano G., D'Armiento M., D'Andrea F., Giugliano D. Effect of a Mediterranean-Style Diet on Endothelial Dysfunction and Markers of Vascular Inflammation in the Metabolic Syndrome: A Randomized Trial. JAMA. 2004;292(12):1440. doi: 10.1001/jama.292.12.1440. [DOI] [PubMed] [Google Scholar]
- 23.Marín C., Yubero-Serrano E.M., López-Miranda J., Pérez-Jiménez F. Endothelial aging associated with oxidative stress can be modulated by a healthy mediterranean diet. Int. J. Mol. Sci. 2013;14(5):8869–8889. doi: 10.3390/ijms14058869. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Rallidis L.S., Lekakis J., Kolomvotsou A., Zampelas A., Vamvakou G., Efstathiou S., Dimitriadis G., Raptis S.A., Kremastinos D.T. Close adherence to a Mediterranean diet improves endothelial function in subjects with abdominal obesity. Am. J. Clin. Nutr. 2009;90(2):263–268. doi: 10.3945/ajcn.2008.27290. [DOI] [PubMed] [Google Scholar]
- 25.Marin C., Ramirez R., Delgado-Lista J., Yubero-Serrano E.M., Perez-Martinez P., Carracedo J., Garcia-Rios A., Rodriguez F., Gutierrez-Mariscal F.M., Gomez P., Perez-Jimenez F., Lopez-Miranda J. Mediterranean diet reduces endothelial damage and improves the regenerative capacity of endothelium. Am. J. Clin. Nutr. 2011;93(2):267–274. doi: 10.3945/ajcn.110.006866. [DOI] [PubMed] [Google Scholar]
- 26.Llorente-Cortés V., Estruch R., Mena M.P., Ros E., González M.A., Fitó M., Lamuela-Raventós R.M., Badimon L. Effect of Mediterranean diet on the expression of pro-atherogenic genes in a population at high cardiovascular risk. Atherosclerosis. 2010;208(2):442–450. doi: 10.1016/j.atherosclerosis.2009.08.004. [DOI] [PubMed] [Google Scholar]
- 27.Hansson G.K., Hermansson A. The immune system in atherosclerosis. Nat. Immunol. 2011;12(3):204–212. doi: 10.1038/ni.2001. [DOI] [PubMed] [Google Scholar]
- 28.Kleemann R., Zadelaar S., Kooistra T. Cytokines and atherosclerosis: a comprehensive review of studies in mice. Cardiovasc. Res. 2008;79(3):360–376. doi: 10.1093/cvr/cvn120. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Vilahur G., Badimon L. Antiplatelet properties of natural products. Vascul. Pharmacol. 2013;59(3-4):67–75. doi: 10.1016/j.vph.2013.08.002. [DOI] [PubMed] [Google Scholar]
- 30.Finn A.V., Nakano M., Narula J., Kolodgie F.D., Virmani R. Concept of vulnerable/unstable plaque. Arterioscler. Thromb. Vasc. Biol. 2010;30(7):1282–1292. doi: 10.1161/ATVBAHA.108.179739. [DOI] [PubMed] [Google Scholar]
- 31.Koenig W., Khuseyinova N. Biomarkers of atherosclerotic plaque instability and rupture. Arterioscler. Thromb. Vasc. Biol. 2007;27(1):15–26. doi: 10.1161/01.ATV.0000251503.35795.4f. [DOI] [PubMed] [Google Scholar]
- 32.Dell’Agli M., Fagnani R., Mitro N., Scurati S., Masciadri M., Mussoni L., Galli G.V., Bosisio E., Crestani M., De Fabiani E., Tremoli E., Caruso D. Minor components of olive oil modulate proatherogenic adhesion molecules involved in endothelial activation. J. Agric. Food Chem. 2006;54(9):3259–3264. doi: 10.1021/jf0529161. [DOI] [PubMed] [Google Scholar]
- 33.Carluccio M.A., Siculella L., Ancora M.A., Massaro M., Scoditti E., Storelli C., Visioli F., Distante A., De Caterina R. Olive oil and red wine antioxidant polyphenols inhibit endothelial activation: antiatherogenic properties of Mediterranean diet phytochemicals. Arterioscler. Thromb. Vasc. Biol. 2003;23(4):622–629. doi: 10.1161/01.ATV.0000062884.69432.A0. [DOI] [PubMed] [Google Scholar]
- 34.Fitó M., Cladellas M., de la Torre R., Martí J., Muñoz D., Schröder H., Alcántara M., Pujadas-Bastardes M., Marrugat J., López-Sabater M.C., Bruguera J., Covas M.I., SOLOS Investigators Anti-inflammatory effect of virgin olive oil in stable coronary disease patients: a randomized; crossover; controlled trial. Eur. J. Clin. Nutr. 2008;62(4):570–574. doi: 10.1038/sj.ejcn.1602724. [DOI] [PubMed] [Google Scholar]
- 35.Sánchez-Taínta A., Estruch R., Bulló M., Corella D., Gómez-Gracia E., Fiol M., Algorta J., Covas M.I., Lapetra J., Zazpe I., Ruiz-Gutiérrez V., Ros E., Martínez-González M.A., PREDIMED group Adherence to a Mediterranean-type diet and reduced prevalence of clustered cardiovascular risk factors in a cohort of 3,204 high-risk patients. Eur. J. Cardiovasc. Prev. Rehabil. 2008;15(5):589–593. doi: 10.1097/HJR.0b013e328308ba61. [DOI] [PubMed] [Google Scholar]
- 36.Athyros V.G., Kakafika A.I., Papageorgiou A.A., Tziomalos K., Peletidou A., Vosikis C., Karagiannis A., Mikhailidis D.P. Effect of a plant stanol ester-containing spread; placebo spread; or Mediterranean diet on estimated cardiovascular risk and lipid; inflammatory and haemostatic factors. Nutr. Metab. Cardiovasc. Dis. 2011;21(3):213–221. doi: 10.1016/j.numecd.2009.08.014. [DOI] [PubMed] [Google Scholar]
- 37.Lopez-Garcia E., Schulze M.B., Fung T.T., Meigs J.B., Rifai N., Manson J.E., Hu F.B. Major dietary patterns are related to plasma concentrations of markers of inflammation and endothelial dysfunction. Am. J. Clin. Nutr. 2004;80(4):1029–1035. doi: 10.1093/ajcn/80.4.1029. [DOI] [PubMed] [Google Scholar]
- 38.Schwingshackl L., Hoffmann G.
- 39.Camargo A., Delgado-Lista J., Garcia-Rios A., Cruz-Teno C., Yubero-Serrano E.M., Perez-Martinez P., Gutierrez-Mariscal F.M., Lora-Aguilar P., Rodriguez-Cantalejo F., Fuentes-Jimenez F., Tinahones F.J., Malagon M.M., Perez-Jimenez F., Lopez-Miranda J. Expression of proinflammatory; proatherogenic genes is reduced by the Mediterranean diet in elderly people. Br. J. Nutr. 2012;108(3):500–508. doi: 10.1017/S0007114511005812. [DOI] [PubMed] [Google Scholar]
- 40.Ruiz-Canela M., Martínez-González M.A. Lifestyle and dietary risk factors for peripheral artery disease. Circ. J. 2014;78(3):553–559. doi: 10.1253/circj.cj-14-0062. [DOI] [PubMed] [Google Scholar]
- 41.Estruch R., Ros E., Salas-Salvadó J., Covas M-I., Corella D., Arós F., Gómez-Gracia E., Ruiz-Gutiérrez V., Fiol M., Lapetra J., Lamuela-Raventos R.M., Serra-Majem L., Pintó X., Basora J., Muñoz M.A., Sorlí J.V., Martínez J.A., Martínez-González M.A., PREDIMED Study Investigators Primary prevention of cardiovascular disease with a Mediterranean diet. N. Engl. J. Med. 2013;368(14):1279–1290. [Google Scholar]
- 42.Juanola-Falgarona M., Salas-Salvadó J., Estruch R., Portillo M.P., Casas R., Miranda J., Martínez-González M.A., Bulló M. Association between dietary phylloquinone intake and peripheral metabolic risk markers related to insulin resistance and diabetes in elderly subjects at high cardiovascular risk. Cardiovasc. Diabetol. 2013;12(1):7. doi: 10.1186/1475-2840-12-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Babio N., Ibarrola-Jurado N., Bulló M., Martínez-González M.Á., Wärnberg J., Salaverría I., Ortega-Calvo M., Estruch R., Serra-Majem L., Covas M.I., Sorli J.V., Salas-Salvadó J., PREDIMED Study Investigators White Blood Cell Counts as Risk Markers of Developing Metabolic Syndrome and Its Components in the Predimed Study. PLoS One. 2013;8(3):e58354. doi: 10.1371/journal.pone.0058354. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Toledo E., Delgado-Rodríguez M., Estruch R., Salas-Salvadó J., Corella D., Gomez-Gracia E., Fiol M., Lamuela-Raventós R.M., Schröder H., Arós F., Ros E., Ruíz-Gutiérrez V., Lapetra J., Conde-Herrera M., Sáez G., Vinyoles E., Martínez-González M.A. Low-fat dairy products and blood pressure: follow-up of 2290 older persons at high cardiovascular risk participating in the PREDIMED study. Br. J. Nutr. 2009;101(01):59. doi: 10.1017/S0007114508981496. [DOI] [PubMed] [Google Scholar]
- 45.Mitjavila M.T., Fandos M., Salas-Salvadó J., Covas M-I., Borrego S., Estruch R., Lamuela-Raventós R., Corella D., Martínez-Gonzalez M.Á., Sánchez J.M., Bulló M., Fitó M., Tormos C., Cerdá C., Casillas R., Moreno J.J., Iradi A., Zaragoza C., Chaves J., Sáez G.T. The Mediterranean diet improves the systemic lipid and DNA oxidative damage in metabolic syndrome individuals. A randomized; controlled; trial. Clin. Nutr. 2013;32(2):172–178. doi: 10.1016/j.clnu.2012.08.002. [DOI] [PubMed] [Google Scholar]
- 46.Mena M-P., Sacanella E., Vazquez-Agell M., Morales M., Fito M., Escoda R., Serrano-Martínez M., Salas-Salvadó J., Benages N., Casas R., Lamuela-Raventós R.M., Masanes F., Ros E., Estruch R. Inhibition of circulating immune cell activation: a molecular antiinflammatory effect of the Mediterranean diet. Am. J. Clin. Nutr. 2008;9(1):248–256. doi: 10.3945/ajcn.2008.26094. [DOI] [PubMed] [Google Scholar]
- 47.Casas R., Sacanella E., Urpi-Sarda M., Chiva-Blanch G. The effects of the Mediterranean diet on biomarkers of vascular wall inflammation and plaque vulnerability in subjects with high risk for cardiovascular disease. A randomized trial. PLoS One. 2014;9(6):e100084. doi: 10.1371/journal.pone.0100084. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Urpi-Sarda M., Casas R., Chiva-Blanch G., Romero-Mamani E.S., Valderas-Martínez P., Salas-Salvadó J., Covas M.I., Toledo E., Andres-Lacueva C., Llorach R., García-Arellano A., Bulló M., Ruiz-Gutierrez V., Lamuela-Raventos R.M., Estruch R. The Mediterranean dietary pattern and its main components are associated with lower plasma concentrations of tumor necrosis factor receptor 60 in patients at high risk for cardiovascular disease. J. Nutr. 2012;142(6):1019–1025. doi: 10.3945/jn.111.148726. [DOI] [PubMed] [Google Scholar]
- 49.Trichopoulou A., Bamia C., Trichopoulos D. Anatomy of health effects of Mediterranean diet: Greek EPIC prospective cohort study. BMJ. 2009;338:b2337. doi: 10.1136/bmj.b2337. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Bendinelli B., Masala G., Saieva C., Salvini S., Calonico C., Sacerdote C., Agnoli C., Grioni S., Frasca G., Mattiello A., Chiodini P., Tumino R., Vineis P., Palli D., Panico S. Fruit; vegetables; and olive oil and risk of coronary heart disease in Italian women: the EPICOR Study. Am. J. Clin. Nutr. 2011;93(2):275–283. doi: 10.3945/ajcn.110.000521. [DOI] [PubMed] [Google Scholar]
- 51.Hermus L., Lefrandt J.D., Tio R.A., Breek J-C., Zeebregts C.J. Carotid plaque formation and serum biomarkers. Atherosclerosis. 2010;213(1):21–29. doi: 10.1016/j.atherosclerosis.2010.05.013. [DOI] [PubMed] [Google Scholar]
- 52.Tanindi A., Sahinarslan A., Elbeg S., Cemri M. Association of matrix metalloproteinase-1; matrix metalloproteinase-9; tissue inhibitor of matrix metalloproteinase-1; and interleukin-6 with epicardial and myocardial perfusion. Coron. Artery Dis. 2011;22(4):253–258. doi: 10.1097/MCA.0b013e328343fc18. [DOI] [PubMed] [Google Scholar]
- 53.Hansson J., Vasan R.S., Ärnlöv J., Ingelsson E., Lind L., Larsson A., Michaëlsson K., Sundström J. Biomarkers of Extracellular Matrix Metabolism (MMP-9 and TIMP-1) and Risk of Stroke; Myocardial Infarction; and Cause-Specific Mortality: Cohort Study. PLoS One. •••;6(1):e16185. doi: 10.1371/journal.pone.0016185. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Trøseid M., Seljeflot I., Arnesen H. The role of interleukin-18 in the metabolic syndrome. Cardiovasc. Diabetol. 2010;9(1):11. doi: 10.1186/1475-2840-9-11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Aihara K-I., Ikeda Y., Yagi S., Akaike M., Matsumoto T. Transforming Growth Factor-β1 as a Common Target Molecule for Development of Cardiovascular Diseases; Renal Insufficiency and Metabolic Syndrome. Cardiol. Res. Pract. 2010;2011:175381. doi: 10.4061/2011/175381. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.González C. A La dieta mediterránea en la prevención del cáncer. ¿Es posible la dieta mediterránea en el siglo XXI? Spain: International Marketing & Communication S.A.; 2011. pp. 191–201. [Google Scholar]
- 57.Couto E., Boffetta P., Lagiou P., Ferrari P., Buckland G., Overvad K., Dahm C.C., Tjønneland A., Olsen A., Clavel-Chapelon F., Boutron-Ruault M.C., Cottet V., Trichopoulos D., Naska A., Benetou V., Kaaks R., Rohrmann S., Boeing H., von Ruesten A., Panico S., Pala V., Vineis P., Palli D., Tumino R., May A., Peeters P.H., Bueno-de-Mesquita H.B., Büchner F.L., Lund E., Skeie G., Engeset D., Gonzalez C.A., Navarro C., Rodríguez L., Sánchez M.J., Amiano P., Barricarte A., Hallmans G., Johansson I., Manjer J., Wirfärt E., Allen N.E., Crowe F., Khaw K.T., Wareham N., Moskal A., Slimani N., Jenab M., Romaguera D., Mouw T., Norat T., Riboli E., Trichopoulou A. Mediterranean dietary pattern and cancer risk in the EPIC cohort. Br. J. Cancer. 2011;104(9):1493–1499. doi: 10.1038/bjc.2011.106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Agudo A., Cabrera L., Amiano P., Ardanaz E., Barricarte A., Berenguer T., Chirlaque M.D., Dorronsoro M., Jakszyn P., Larrañaga N., Martínez C., Navarro C., Quirós J.R., Sánchez M.J., Tormo M.J., González C.A. Fruit and vegetable intakes, dietary antioxidant nutrients, and total mortality in Spanish adults: findings from the Spanish cohort of the European Prospective Investigation into Cancer and Nutrition (EPIC-Spain). Am. J. Clin. Nutr. 2007;85(6):1634–1642. doi: 10.1093/ajcn/85.6.1634. [DOI] [PubMed] [Google Scholar]
- 59.Hercberg S., Czernichow S., Galan P. Antioxidant vitamins and minerals in prevention of cancers: lessons from the SU.VI.MAX study. Br. J. Nutr. 2006;96(Suppl. 1):S28–S30. doi: 10.1079/bjn20061695. [DOI] [PubMed] [Google Scholar]
- 60.Peta C. Tackling diet-related disease by promoting fruit and vegetables. Nutr. Food Sci. 1999;99(4):173–179. [Google Scholar]
- 61.Sofi F., Cesari F., Abbate R., Gensini G.F., Casini A. Adherence to Mediterranean diet and health status: meta-analysis. BMJ. 2008;337:a1344. doi: 10.1136/bmj.a1344. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Samoli E., Lagiou A., Nikolopoulos E., Lagogiannis G., Barbouni A., Lefantzis D., Trichopoulos D., Brennan P., Lagiou P. Mediterranean diet and upper aerodigestive tract cancer: the Greek segment of the Alcohol-Related Cancers and Genetic Susceptibility in Europe study. Br. J. Nutr. 2010;104(9):1369–1374. doi: 10.1017/S0007114510002205. [DOI] [PubMed] [Google Scholar]
- 63.Ferrís-Tortajada J., Berbel-Tornero O., García-Castell J., Ortega-García J.A., López-Andreu J.A. Dietetic factors associated with prostate cancer: protective effects of Mediterranean diet. Actas Urol. Esp. 2012;36(4):239–245. doi: 10.1016/j.acuro.2011.08.002. [DOI] [PubMed] [Google Scholar]
- 64.Escrich E., Moral R., Solanas M. Olive oil, an essential component of the Mediterranean diet, and breast cancer. Public Health Nutr. 2011;14(12A):2323–2332. doi: 10.1017/S1368980011002588. [DOI] [PubMed] [Google Scholar]
- 65.Mourouti N., Kontogianni M.D., Papavagelis C., Plytzanopoulou P., Vassilakou T., Malamos N., Linos A., Panagiotakos D.B. Adherence to the Mediterranean Diet is associated with lower likelihood of breast cancer: a case-control study. Nutr. Cancer. 2014;66(5):810–817. doi: 10.1080/01635581.2014.916319. [DOI] [PubMed] [Google Scholar]
- 66.World Cancer Research Fund & American Investigation of Cancer Research . Food, Nutrition and the Prevention Cancer: a global perspective. USA: BANTA Book Group Menasha; 2007. [Google Scholar]
- 67.González C.A., Jakszyn P., Pera G., Agudo A., Bingham S., Palli D., Ferrari P., Boeing H., del Giudice G., Plebani M., Carneiro F., Nesi G., Berrino F., Sacerdote C., Tumino R., Panico S., Berglund G., Simán H., Nyrén O., Hallmans G., Martinez C., Dorronsoro M., Barricarte A., Navarro C. Meat intake and risk of stomach and esophageal adenocarcinoma within the European Prospective Investigation Into Cancer and Nutrition (EPIC). J. Natl. Cancer Inst. 2006;98(5):345–354. doi: 10.1093/jnci/djj071. [DOI] [PubMed] [Google Scholar]
- 68.Dolores C., Xavier P., Martínez-González M.Á., Estruch R., Ros E. Polyphenol-Rich Foods in the Mediterranean Diet are Associated with Better Cognitive Function in Elderly Subjects at High Cardiovascular Risk. J. Alzheimers Dis. 2012;29(4):773–782. doi: 10.3233/JAD-2012-111799. [DOI] [PubMed] [Google Scholar]
- 69.Matrone C., Djelloul M., Taglialatela G., Perrone L. Inflammatory risk factors and pathologies promoting Alzheimer`s disease progression: is RAGE the key? Histol. Histopathol. 2014 doi: 10.14670/HH-30.125. [Epub ahead of print]. [DOI] [PubMed] [Google Scholar]
- 70.Toledo Atucha J. Comportamiento, dieta, factores de riesgo cardiovascular y enfermedades neurodegenerativas. ¿Es posible la dieta mediterránea en el siglo XXI? Spain: International Marketing & Communication S.A.; 2011. pp. 203–214. [Google Scholar]
- 71.Solfrizzi V., Frisardi V., Seripa D., Logroscino G., Imbimbo B.P., D'Onofrio G., Addante F., Sancarlo D., Cascavilla L., Pilotto A., Panza F. Mediterranean diet in predementia and dementia syndromes. Curr. Alzheimer Res. 2011;8(5):520–542. doi: 10.2174/156720511796391809. [DOI] [PubMed] [Google Scholar]
- 72.Psaltopoulou T., Sergentanis T.N., Panagiotakos D.B., Sergentanis I.N., Kosti R., Scarmeas N. Mediterranean diet, stroke, cognitive impairment, and depression: A meta-analysis. Ann. Neurol. 2013;74(4):580–591. doi: 10.1002/ana.23944. [DOI] [PubMed] [Google Scholar]
- 73.Isaac MGEKN. Vitamin E for Alzheimer’s disease and mild cognitive impairment. Cochrane Database Syst. Rev. 2008;(3):CD002854. doi: 10.1002/14651858.CD002854.pub2. [DOI] [PubMed] [Google Scholar]
- 74.Frisardi V., Panza F., Seripa D., Imbimbo B.P., Vendemiale G., Pilotto A., Solfrizzi V. Nutraceutical properties of Mediterranean diet and cognitive decline: possible underlying mechanisms. J. Alzheimers Dis. 2010;22(3):715–740. doi: 10.3233/JAD-2010-100942. [DOI] [PubMed] [Google Scholar]
- 75.Seneviratne A.N., Sivagurunathan B., Monaco C. Toll-like receptors and macrophage activation in atherosclerosis. Clin. Chim. Acta. 2012;413(1-2):3–14. doi: 10.1016/j.cca.2011.08.021. [DOI] [PubMed] [Google Scholar]
- 76.Lundberg A.M., Hansson G.K. Innate immune signals in atherosclerosis. Clin. Immunol. 2010;134(1):5–24. doi: 10.1016/j.clim.2009.07.016. [DOI] [PubMed] [Google Scholar]