

Abstract
The optimal immunosuppressive strategy for renal transplant recipients at high immunologic risk remains a topic of investigation. This prospective single arm pilot study was undertaken to evaluate the safety and efficacy of a combined tacrolimus and sirolimus regimen in recipients at immunological high risk and to compare outcomes with a contemporaneous control group received tacrolimus and mycophenolate mofetil. Patients that received a renal allograft between 2010 and 2011 at high risk (defined as panel reactive antibodies > 50%, 4 or more human leukocyte antigen mismatches, or retransplantation) were enrolled. All patients received basiliximab induction and corticosteroids. A total of 28 recipients treated with tacrolimus and sirolimus were enrolled in this study and 69 recipients were retrospectively reviewed as a control group. The sirolimus group showed a higher, but not statistically significant, incidence of biopsy proven acute rejection and a lower glomerular filtration rate than the control group. Furthermore, sirolimus group was associated with significant increases in BKV infection (P = 0.031), dyslipidemia (P = 0.004), and lymphocele (P = 0.020). The study was terminated prematurely due to a high incidence of adverse events. A de novo tacrolimus/sirolimus combination regimen may not be an ideal choice for recipients at high immunological risk.
Graphical Abstract
Keywords: Sirolimus, Tacrolimus, Kidney Transplantation, Graft Rejection
INTRODUCTION
Recent immunosuppressive agent developments and patient management improvements have increased overall early graft survival after renal transplantation. However, certain subpopulations with a high titer of panel reactive antibodies (PRAs), four or more human leucocyte antigen (HLA) mismatches, or a history of previous allograft loss remain at high risk of acute rejection and allograft loss (1). To reduce acute rejection rates, clinicians have tried to maintain high concentrations of immunosuppressants (2, 3), but optimal drug levels for patients at high immunological risk have not been clearly defined. Furthermore, the nephrotoxic effects of calcineurin inhibitors (CNIs) contribute to progressive graft dysfunction and diminish long-term graft survival (4, 5).
Sirolimus is a macrocyclic lactone antibiotic produced from Streptomyces hygroscopicus and a potent immunosuppressive agent with a multifaceted action mechanism quite distinct from that of CNIs. Sirolimus forms a complex with FKBP-12, which binds to the mammalian target of rapamycin (mTOR), and thus, inhibits cytokine-induced signal transduction pathways and arrests the cell cycle (6). Furthermore, early preclinical experience indicates that the sirolimus-tacrolimus combination exhibits immunosuppressive synergy (7).
In an attempt to reduce acute rejection and minimize the toxicity of tacrolimus, several authors have investigated the use of tacrolimus and sirolimus in combination (8, 9, 10). We designed this study to assess the clinical safety and efficacy of a tacrolimus/sirolimus regimen in renal allograft recipients at high immunological risk.
MATERIALS AND METHODS
Inclusion criteria
Adult patients (>18 yr) with end stage renal disease scheduled to receive renal transplantation and at high immunological risk (defined as a PRA >50% during the previous 6 months, 4 or more HLA mismatches, or a history of previous graft loss) were eligible for enrollment. The retrospective contemporaneous control group also consisted of patients at high immunological risk.
Immunosuppression
All patients received 20 mg basiliximab on day 0 and 4 after transplantation. The initial dose of methylprednisolone (500-1,000 mg) was tapered to oral prednisolone (5-10 mg/day). Patients with a high PRA (having a PRA >50%) received one dose (375 mg/m2) of rituximab two days prior to transplantation.
Sirolimus group
Initial tacrolimus was administered orally at 0.1 mg/kg twice daily. Subsequent doses were adjusted to maintain a whole blood trough concentration from 10 to 15 ng/mL between days 1 and 14 post-transplantation, from 5 to 10 ng/mL between days 15 and 180, and from 3 to 7 ng/mL between days 181 and 360.
Sirolimus was started with a 6mg loading dose on day 3, and then reduced to maintain a whole blood trough concentration (as determined by an antibody conjugated magnetic immunoassay) of 5-10 ng/mL until day 14 and of 10-15 ng/mL between days 15 and 360.
Contemporaneous control group
These patients were managed by triple drug immunosuppression consisting of tacrolimus, mycophenolate mofetil (MMF), and corticosteroids. Target trough concentrations of tacrolimus were similar to those in the sirolimus group (5-10 ng/mL until day 180, and 3-7 ng/mL between day 181 and 360).
Endpoints
The study efficacy variables were the incidence of biopsy proven acute rejection (BPAR) and estimated glomerular filtration rates (eGFR) at 6 and 12 months. BPAR events were classified using the Banff 2007 classification. Safety variables included the incidences of specific adverse events of particular interest (viral infections, pneumonitis, new onset diabetes mellitus, dyslipidemia, lymphocele, wound complications, and malignancy) and of adverse events leading to study discontinuation. A predefined acceptable serious adverse events threshold of 50% was implemented.
Crossmatch
HLA crossmatch was determined using a complement-dependent lymphocytotoxicity (CDC) assay. The NIH (National Institute of Health) and AHG (anti-human globulin)-enhanced CDC (complement-dependent cytotoxicity) assays were performed to detect antibodies against donor T cells. The CDC assay was used to detect warm antibodies against B cells.
Panel reactive HLA IgG antibodies (PRA) were identified by LIFECODES Class I and Class II ID assay kits (Tepnel Lifecodes Molecular Diagnostics, Stamford, CT, USA), which utilize the multiplex bead-based immunoassay principle.
Statistical analysis
Demographic and background information was summarized using frequency counts (percentages) for categorical variables, and using descriptive statistics, that is, means, standard deviations, medians, minima, and maxima for continuous variables. Efficacy and safety analyses were conducted according to the intention to treat (ITT) principle and included all patients that received at least one dose of the study regimen (tacrolimus plus sirolimus or MMF). The student's t-test was used to determine the significances of differences between the means of numerical variables in the sirolimus and control groups. The chi-square test with Fisher's exact test was used to compare nominal variables. P values less than 0.05 were considered statistically significant, and the analysis was performed using SPSS software (version 20.0; SPSS Inc., Chicago, IL, USA).
Ethics statement
This prospective, 12-month, open-labeled, single arm pilot study was approved by the institutional review board of Severance Hospital, Yonsei University Health System (4-2009-0294). Informed consent was waived by the board.
RESULTS
A total of 28 patients were enrolled, and these were compared with a contemporaneous control group consisting of 69 recipients. Initially, we planned to recruit 50 recipients, but because of efficacy and safety concerns, our data and safety monitoring board recommended discontinuation of further enrollment. This pilot study was stopped prematurely, but 20 patients (71.4%) completed the study on protocol drugs.
Demographic and baseline characteristics are summarized in Table 1. No statistical differences were observed between the sirolimus and control groups in terms of recipient, donor, or immunologic factors, with the exception of mean number of HLA-DR mismatches and deceased donor proportion, which was significantly higher in the control group. However, there were no significant differences between re-transplantation, high PRA titer, or total number of HLA mismatches. Donor-specific anti-HLA antibodies were not routinely assessed during the study period. Mean serum tacrolimus and sirolimus concentrations during the study period are provided in Fig. 1.
Table 1. Patient demographics.
| Factors | Sirolimus group (n=28) |
Control group (n=69) |
P value |
|---|---|---|---|
| Recipient factors | |||
| Age (yr) | 47.71±9.01 | 44.94±10.76 | 0.232 |
| Male recipients | 12 (42.9%) | 38 (55.1%) | 0.275 |
| Donor factors | |||
| Deceased donor | 4 (14.3%) | 33 (47.8%) | 0.002 |
| Donor age (yr) | 44.96±10.90 | 43.43±12.31 | 0.569 |
| Male donors | 12 (42.9%) | 35 (50.7%) | 0.482 |
| Immunologic factors | |||
| Previous renal transplant | 6 (21.4%) | 8 (11.6%) | 0.219 |
| High PRA | 14 (50.0%) | 27 (39.1%) | 0.326 |
| HLA-mismatch | 3.89±1.45 | 3.59±1.44 | 0.357 |
| A | 1.07±0.72 | 1.03±0.69 | 0.786 |
| B | 1.43±0.63 | 1.46±0.68 | 0.814 |
| DR | 1.39±0.57 | 1.10±0.67 | 0.045 |
| Total HLA mismatch ≥4 | 18 (64.3%) | 50 (72.5%) | 0.425 |
PRA, panel reactive antibody; HLA, human leukocyte antigen.
Fig. 1. Mean study drug trough levels by visit window. (A) Tacrolimus, (B) Sirolimus; mean values with±standard deviations at each time point. The dashed lines represent the respective target trough levels, (C) Mean tacrolimus trough levels of sirolimus group and control group.

In sirolimus group (n=28), 8 patients (28.6%) were withdrawn from the study from the study. Mean time to discontinuation was 74.3 days. Four discontinued because of rejection, two for infection, one for drug-induced pneumonitis, and one for cardiac arrest. Most patients who discontinued assigned therapies were switched to tacrolimus and MMF.
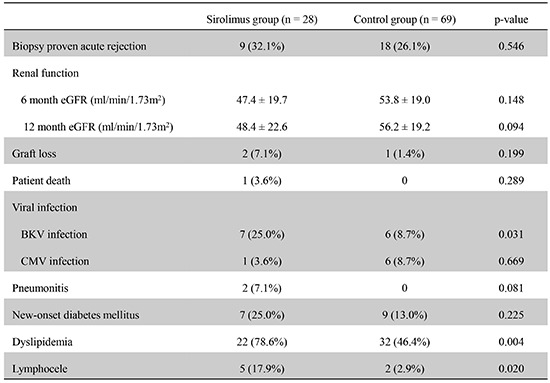
Efficacy and safety results are summarized in Table 2. Renal function was assessed using mean estimated glomerular filtration rate (eGFR, calculated using the modification of diet in renal disease formula). Mean eGFR of the control group was higher than in the sirolimus group at the time points, but this was not statistically significant. Overall rejection rates were similar in the two groups (32.1% in the sirolimus group, 26.1% in the control group, P=0.546). The anti-rejection treatments and responses to treatment are summarized in Table 3. In the sirolimus group, two recipients showed T cell-mediated rejection with transplant glomerulitis. Both were C4d negative in peritubular capillaries and recovered renal function after anti-rejection therapy consisting of steroid pulse and anti-thymocyte globulin (ATG). In the control group, three recipients developed antibody-mediated rejection.
Table 2. Efficacy and safety results.
| Parameters | Sirolimus group (n = 28) |
Control group (n = 69) |
P value |
|---|---|---|---|
| Renal function | |||
| 6 month eGFR (mL/min/1.73 m2) | 47.4±19.7 | 53.8±19.0 | 0.148 |
| 12 month eGFR (mL/min/1.73 m2) | 48.4±22.6 | 56.2±19.2 | 0.094 |
| Biopsy proven acute rejection | 9 (32.1%) | 18 (26.1%) | 0.546 |
| Graft loss | 2 (7.1%) | 1 (1.4%) | 0.199 |
| Patient death | 1 (3.6%) | 0 | 0.289 |
| Delayed graft function | 3 (10.7%) | 11 (15.9%) | 0.751 |
| Viral infection | |||
| BKV infection | 7 (25.0%) | 6 (8.7%) | 0.031 |
| BK viremia | 7 (25.0%) | 6 (8.7%) | |
| BKV nephropathy | 4 (14.3%) | 1 (1.4%) | |
| CMV infection | 1 (3.6%) | 6 (8.7%) | 0.669 |
| Pneumonitis | 2 (7.1%) | 0 | 0.081 |
| New-onset diabetes mellitus | 7 (25.0%) | 9 (13.0%) | 0.225 |
| Dyslipidemia | 22 (78.6%) | 32 (46.4%) | 0.004 |
| Lymphocele | 5 (17.9%) | 2 (2.9%) | 0.020 |
| Wound complication | 2 (7.1%) | 2 (2.9%) | 0.577 |
| Malignancy | 0 | 1 (1.4%) | >0.99 |
eGFR, estimated glomerular filtration rate (MDRD, modification of diet in renal disease formula); TCMR, T cell mediated rejection; CMV, cytomegalovirus.
Table 3. Acute rejections during the study period.
| Rejection factors | Sirolimus | Control | P value |
|---|---|---|---|
| Biopsy proven acute rejection | 9 (32.1%) | 18 (26.1%) | 0.546 |
| TCMR | 9 | 15 | |
| AMR | 0 | 1 | |
| Mixed rejection | 0 | 2 | |
| Time to first BPAR, day (median, range) | 61 (5-373) | 29 (5-175) | 0.455 |
| Anti-rejection treatment | |||
| Antibody therapy* | 3 (33.3%) | 4 (22.2%) | 0.653 |
| Therapeutic plasmapheresis | 1 (11.1%) | 2 (11.1%) | >0.99 |
*Antithymocyte globulin (ATG). TCMR, T cell mediated rejection; AMR, antibody-mediated rejection; BPAR, Biopsy proven acute rejection.
One patient in the sirolimus group succumbed to fungal pneumonia (Day 45), and one graft was lost due to BK virus nephropathy (Day 253) during the 12 month study period. In the control group, one graft failure occurred due to mixed rejection. No significant intergroup difference was found for cytomegalovirus (CMV) infection. However, BKV infection, dyslipidemia, and lymphocele rates were significantly higher in the sirolimus group.
In the sirolimus group, drug-induced pneumonitis occurred in 2 patients. Lymphocele occurred in 5 patients (17.9%), and of these five, three underwent laparoscopic fenestration and one percutaneous catheter drainage. No malignancy was reported during the study period.
In the control group, one case of lymphocele was treated conservatively. One patient developed Kaposi's sarcoma at 7 months post-transplant, and was switched from tacrolimus to sirolimus with MMF discontinuation. He responded well to treatment and remained well at 3 yr post-transplant.
DISCUSSION
Several authors have reported that tacrolimus and sirolimus in combination can achieve low rates of acute rejection (8, 9). Furthermore, in a randomized large cohort study, de novo regimens containing sirolimus with CNIs were found to be efficacious and well tolerated in high risk recipients (10, 11). We decided to perform this pilot study in the hope of reducing acute rejection rates and improving renal function. Although statistically not significant, we found the BPAR rate was higher and mean eGFR was lower in the sirolimus group than in the control group. Furthermore, we encountered a high withdrawal rate (28.6%), which was attributed to significant increases in BKV infection, lymphocele, and dyslipidemia.
No therapeutic target ranges have been established for the de novo sirolimus/tacrolimus combination (12). In the present study, relatively high drug concentrations were maintained than in prior studies that adopted de novo tacrolimus plus sirolimus regimens (13, 14). However, target drug levels in the present study were similar to those reported in previous studies on recipients at high immunological risk (10, 11). But, unlike these previous studies, we observed a high incidence of acute rejection. Although, there is no accepted definition of "high immunological risk" (15), most authors have classified African Americans as being at high risk, and in such studies the proportion of African American exceeded 70% (10, 11). Accordingly, the results of prior studies should be interpreted with caution as they included only a small proportion of other ethnic recipients with immunologic risk factors. In the present study, the high incidence of acute rejection observed may have been due to underlying immunological risk. Nevertheless, the rejection preventing effects of sirolimus in this study were inadequate even at a high trough level, and sirolimus did not show any advantage in renal function as compared with the tacrolimus/MMF treated controls.
Induction therapy also plays an important role in the prevention of acute rejection. We used basiliximab as an induction therapy and a potent maintenance regimen (tacrolimus plus sirolimus). Basiliximab and ATG are widely used for induction therapy in kidney transplantation, and ATG has usually been used in high risk or black recipients (16). However, optimal induction therapy remains a subject of debate because of the developments of more potent immunosuppressive drugs and the risk of over-immunosuppression. In a recent prospective study, it was shown that ATG induction is effective in black recipients, but not effective in sensitized patients with high PRAs (17).
The impact that high drug trough levels have on the development of adverse events is an important finding of the present study, and has been reported previously in several studies. Sirolimus related toxicities are known to exhibit dose-dependent characteristics (18, 19, 20), and a high proportion of recipients in present study discontinued sirolimus due to adverse events. As mentioned above, the majority of studies on high risk recipients have been conducted on African Americans, and previous studies have shown these patients tend to need higher immunosuppressant levels to optimize graft outcomes (10, 21). Thus, the high withdrawal and adverse event rates observed in this study could be related to the use of relatively high target trough levels for non-black recipients. We suggest that efforts be made to determine optimal target drug levels for different ethnicities, because of the narrow therapeutic window of sirolimus.
The high incidence of viral infections encountered in this trial was unexpected, because mTOR inhibitors, like sirolimus, are known to have anti-viral effects (22, 23). In this study, a high proportion of patients received powerful immunosuppressive drugs in addition to mTOR inhibitors. Some of them received steroid pulse or ATG treatment for acute rejection. In addition, patients with a high PRA titer received rituximab prior to transplantation. The patient's net state of immunosuppression may be attributable to the relatively high incidence of viral infection (24, 25).
Immunosuppressive drugs all have positive and negative characteristics. Recent randomized trials demonstrated comparable efficacies and renal functions for de novo CNI/mTOR inhibitor and CNI/MMF combinations. Furthermore, similar results have been achieved for reduced CNI plus low dose mTOR inhibitor therapy. It has been shown that mTOR inhibitors are potent immunosuppressants, but in patients at immunological low risk (26, 27, 28). In the present study, high levels of sirolimus were maintained to overcome immunological risk, but contrary to expectation, high trough level of sirolimus did not reduce the incidence of acute rejection in our high immunological risk patients. Rather, these high levels were found to be associated with high incidences of adverse events, which contributed to study discontinuation. This was consistent with findings from recent studies, in which a higher rate of discontinuation due to adverse events occurred in high level mTOR inhibitor group (27, 28).
The availability of more sensitive tests would allow individuals at immunologic risk to be characterized more precisely. However, traditional risk factors, such as, high PRA and poor HLA matching remain problematic and optimal immunosuppressive strategies for recipients at high immunologic risk are still being investigated (29). Furthermore, because of their small numbers and heterogeneous degrees of risk, patients at high immunologic risk have been excluded from clinical trials. Accordingly, special efforts are needed to identify proper immunosuppression strategies for these recipients.
Several limitations of our study require consideration. First, it was a single arm study conducted on a small population, and the trial was terminated prematurely due to high rates of acute rejection and withdrawal due to adverse events. Therefore, we retrospectively compared the results of this pilot study with those of a nonrandomized contemporaneous control group. Second, the study is limited by its 12-month follow-up, which prevents predictions of long-term outcomes. Despite the high rate of discontinuation encountered, we are continuing to collate follow-up data to gain access to long-term outcomes. Third, we did not routinely measure donor-specific anti-HLA antibodies during the study period, because the clinical use of solid phase test for antibody detection was not well established during the design phase of this study. Further randomized studies across ethnicities with longer follow-ups are required to prove the effectiveness of immunosuppressive strategies in recipients at high immunological risk.
We conclude that the tacrolimus/sirolimus combination regimen may not be an ideal choice for recipients at high immunologic risk. Further investigations should be conducted to determine optimal target blood levels of tacrolimus and sirolimus to reduce side effects.
Footnotes
This investigator-initiated study was supported by Wyeth Korea, which was acquired by Pfizer pharmaceuticals in 2010 (WS1234554, 2009).
DISCLOSURE: The authors of this manuscript have potential conflicts of interest to disclose. Lee J, Lee JJ, and Lee JG have declared no conflicts of interest. Huh KH and Kim BS have participated in clinical trials sponsored by and received research grants from Astellas and Norvatis. Kim YS has participated in clinical trials sponsored by Astellas, Novartis, Roche, CKD, and Wyeth, and he has received research grants from Astellas, Novartis, Roche, and CKD. No one has stocks of the respective pharmaceutical companies.
AUTHOR CONTRIBUTION: Conceived and designed the experiments: Kim YS. Performed the experiments: Kim BS, Huh KH, Kim YS. Enrolled patients: Lee JJ, Huh KH, Kim YS. Analyzed the data: Lee J, Lee JJ, Lee JG. Contributed reagents/materials/analysis tools: Lee JG, Park Y, Kim YS. Wrote the first draft of the manuscript: Lee J, Lee JJ. Wrote the paper: Lee J, Lee JJ, Huh HK, Kim BS, Kim YS. ICMJE criteria for authorship read and met: Lee J, Lee JJ, Kim BS, Lee JG, Huh KH, Park Y, Kim YS. Agree with manuscript results and conclusions: all authors.
References
- 1.Foster BJ, Dahhou M, Zhang X, Platt RW, Hanley JA. Relative importance of HLA mismatch and donor age to graft survival in young kidney transplant recipients. Transplantation. 2013;96:469–475. doi: 10.1097/TP.0b013e318298f9db. [DOI] [PubMed] [Google Scholar]
- 2.Borobia AM, Romero I, Jimenez C, Gil F, Ramirez E, De Gracia R, Escuin F, Gonzalez E, Sansuán AJ. Trough tacrolimus concentrations in the first week after kidney transplantation are related to acute rejection. Ther Drug Monit. 2009;31:436–442. doi: 10.1097/FTD.0b013e3181a8f02a. [DOI] [PubMed] [Google Scholar]
- 3.O'Seaghdha CM, McQuillan R, Moran AM, Lavin P, Dorman A, O'Kelly P, Mohan DM, Little P, Hickey DP, Conlon PJ. Higher tacrolimus trough levels on days 2-5 post-renal transplant are associated with reduced rates of acute rejection. Clin Transplant. 2009;23:462–468. doi: 10.1111/j.1399-0012.2009.01021.x. [DOI] [PubMed] [Google Scholar]
- 4.Larson TS, Dean PG, Stegall MD, Griffin MD, Textor SC, Schwab TR, Gloor JM, Cosio FG, Lund WJ, Kremers WK, et al. Complete avoidance of calcineurin inhibitors in renal transplantation: a randomized trial comparing sirolimus and tacrolimus. Am J Transplant. 2006;6:514–522. doi: 10.1111/j.1600-6143.2005.01177.x. [DOI] [PubMed] [Google Scholar]
- 5.Lamb KE, Lodhi S, Meier-Kriesche HU. Long-term renal allograft survival in the United States: a critical reappraisal. Am J Transplant. 2011;11:450–462. doi: 10.1111/j.1600-6143.2010.03283.x. [DOI] [PubMed] [Google Scholar]
- 6.Halloran PF. Immunosuppressive drugs for kidney transplantation. N Engl J Med. 2004;351:2715–2729. doi: 10.1056/NEJMra033540. [DOI] [PubMed] [Google Scholar]
- 7.Vu MD, Qi S, Xu D, Wu J, Fitzsimmons WE, Sehgal SN, Dumont L, Busque S, Daloze P, Chen H. Tacrolimus (FK506) and sirolimus (rapamycin) in combination are not antagonistic but produce extended graft survival in cardiac transplantation in the rat. Transplantation. 1997;64:1853–1856. doi: 10.1097/00007890-199712270-00039. [DOI] [PubMed] [Google Scholar]
- 8.van Hooff JP, Squifflet JP, Wlodarczyk Z, Vanrenterghem Y, Paczek L. A prospective randomized multicenter study of tacrolimus in combination with sirolimus in renal-transplant recipients. Transplantation. 2003;75:1934–1939. doi: 10.1097/01.TP.0000071301.86299.75. [DOI] [PubMed] [Google Scholar]
- 9.Vitko S, Wlodarczyk Z, Kyllönen L, Czajkowski Z, Margreiter R, Backman L, Perner F, Rigotti P, Jaques B, Abramowicz D, et al. Tacrolimus combined with two different dosages of sirolimus in kidney transplantation: results of a multicenter study. Am J Transplant. 2006;6:531–538. doi: 10.1111/j.1600-6143.2005.01193.x. [DOI] [PubMed] [Google Scholar]
- 10.Gaber AO, Kahan BD, Van Buren C, Schulman SL, Scarola J, Neylan JF Sirolimus High-Risk Study Group. Comparison of sirolimus plus tacrolimus versus sirolimus plus cyclosporine in high-risk renal allograft recipients: results from an open-label, randomized trial. Transplantation. 2008;86:1187–1195. doi: 10.1097/TP.0b013e318187bab0. [DOI] [PubMed] [Google Scholar]
- 11.Lo A, Egidi MF, Gaber LW, Shokouh-Amiri MH, Nazakatgoo N, Fisher JS, Gaber AO. Observations regarding the use of sirolimus and tacrolimus in high-risk cadaveric renal transplantation. Clin Transplant. 2004;18:53–61. doi: 10.1111/j.1399-0012.2004.00116.x. [DOI] [PubMed] [Google Scholar]
- 12.Shihab F, Christians U, Smith L, Wellen JR, Kaplan B. Focus on mTOR inhibitors and tacrolimus in renal transplantation: pharmacokinetics, exposure-response relationships, and clinical outcomes. Transpl Immunol. 2014;31:22–32. doi: 10.1016/j.trim.2014.05.002. [DOI] [PubMed] [Google Scholar]
- 13.Mendez R, Gonwa T, Yang HC, Weinstein S, Jensik S, Steinberg S Prograf Study Group. A prospective, randomized trial of tacrolimus in combination with sirolimus or mycophenolate mofetil in kidney transplantation: results at 1 year. Transplantation. 2005;80:303–309. doi: 10.1097/01.tp.0000167757.63922.42. [DOI] [PubMed] [Google Scholar]
- 14.Sampaio EL, Pinheiro-Machado PG, Garcia R, Felipe CR, Park SI, Casarini DE, Moreira S, Franco MF, Tedesco-Silva H, Jr, Medina-Pestana JO. Mycophenolate mofetil vs. sirolimus in kidney transplant recipients receiving tacrolimus-based immunosuppressive regimen. Clin Transplant. 2008;22:141–149. doi: 10.1111/j.1399-0012.2007.00756.x. [DOI] [PubMed] [Google Scholar]
- 15.Lebranchu Y, Baan C, Biancone L, Legendre C, Morales JM, Naesens M, Thomusch O, Friend P. Pretransplant identification of acute rejection risk following kidney transplantation. Transpl Int. 2014;27:129–138. doi: 10.1111/tri.12205. [DOI] [PubMed] [Google Scholar]
- 16.Brennan DC, Daller JA, Lake KD, Cibrik D, Del Castillo D Thymoglobulin Induction Study Group. Rabbit antithymocyte globulin versus basiliximab in renal transplantation. N Engl J Med. 2006;355:1967–1977. doi: 10.1056/NEJMoa060068. [DOI] [PubMed] [Google Scholar]
- 17.Pilch NA, Taber DJ, Moussa O, Thomas B, Denmark S, Meadows HB, McGillicuddy JW, Srinivas TR, Baliga PK, Chavin KD. Prospective randomized controlled trial of rabbit antithymocyte globulin compared with IL-2 receptor antagonist induction therapy in kidney transplantation. Ann Surg. 2014;259:888–893. doi: 10.1097/SLA.0000000000000496. [DOI] [PubMed] [Google Scholar]
- 18.Peddi VR, Wiseman A, Chavin K, Slakey D. Review of combination therapy with mTOR inhibitors and tacrolimus minimization after transplantation. Transplant Rev (Orlando) 2013;27:97–107. doi: 10.1016/j.trre.2013.06.001. [DOI] [PubMed] [Google Scholar]
- 19.Murakami N, Riella LV, Funakoshi T. Risk of metabolic complications in kidney transplantation after conversion to mTOR inhibitor: a systematic review and meta-analysis. Am J Transplant. 2014;14:2317–2327. doi: 10.1111/ajt.12852. [DOI] [PubMed] [Google Scholar]
- 20.Lee HS, Huh KH, Kim YS, Kim MS, Kim HJ, Kim SI, Joo DJ. Sirolimus-induced pneumonitis after renal transplantation: a single-center experience. Transplant Proc. 2012;44:161–163. doi: 10.1016/j.transproceed.2011.11.059. [DOI] [PubMed] [Google Scholar]
- 21.Patel N, Taber DJ, Weimert NA, Fleming JN, Egidi FM, McGillicuddy J, Bratton CF, Lin A, Chavin KD, Baliga PK. Potential differences in kidney allograft outcomes between ethnicities when converting to sirolimus base immunosuppression. Transplant Proc. 2009;41:4131–4137. doi: 10.1016/j.transproceed.2009.09.088. [DOI] [PubMed] [Google Scholar]
- 22.Nashan B, Gaston R, Emery V, Säemann MD, Mueller NJ, Couzi L, Dantal J, Shihab F, Mulgaonkar S, Seun Kim Y, et al. Review of cytomegalovirus infection findings with mammalian target of rapamycin inhibitor-based immunosuppressive therapy in de novo renal transplant recipients. Transplantation. 2012;93:1075–1085. doi: 10.1097/TP.0b013e31824810e6. [DOI] [PubMed] [Google Scholar]
- 23.Andrassy J, Hoffmann VS, Rentsch M, Stangl M, Habicht A, Meiser B, Fischereder M, Jauch KW, Guba M. Is cytomegalovirus prophylaxis dispensable in patients receiving an mTOR inhibitor-based immunosuppression? a systematic review and meta-analysis. Transplantation. 2012;94:1208–1217. doi: 10.1097/TP.0b013e3182708e56. [DOI] [PubMed] [Google Scholar]
- 24.Grim SA, Pham T, Thielke J, Sankary H, Oberholzer J, Benedetti E, Clark NM. Infectious complications associated with the use of rituximab for ABO-incompatible and positive cross-match renal transplant recipients. Clin Transplant. 2007;21:628–632. doi: 10.1111/j.1399-0012.2007.00700.x. [DOI] [PubMed] [Google Scholar]
- 25.Fishman JA. Infection in solid-organ transplant recipients. N Engl J Med. 2007;357:2601–2614. doi: 10.1056/NEJMra064928. [DOI] [PubMed] [Google Scholar]
- 26.Langer RM, Hené R, Vitko S, Christiaans M, Tedesco-Silva H, Jr, Ciechanowski K, Cassuto E, Rostaing L, Vilatoba M, Machein U, et al. Everolimus plus early tacrolimus minimization: a phase III, randomized, open-label, multicentre trial in renal transplantation. Transpl Int. 2012;25:592–602. doi: 10.1111/j.1432-2277.2012.01465.x. [DOI] [PubMed] [Google Scholar]
- 27.Cibrik D, Silva HT, Jr, Vathsala A, Lackova E, Cornu-Artis C, Walker RG, Wang Z, Zibari GB, Shihab F, Kim YS. Randomized trial of everolimus-facilitated calcineurin inhibitor minimization over 24 months in renal transplantation. Transplantation. 2013;95:933–942. doi: 10.1097/TP.0b013e3182848e03. [DOI] [PubMed] [Google Scholar]
- 28.Shihab FS, Cibrik D, Chan L, Kim YS, Carmellini M, Walker R, Zibari G, Pattison J, Cornu-Artis C, Wang Z, et al. Association of clinical events with everolimus exposure in kidney transplant patients receiving reduced cyclosporine. Clin Transplant. 2013;27:217–226. doi: 10.1111/ctr.12045. [DOI] [PubMed] [Google Scholar]
- 29.Dunn TB, Noreen H, Gillingham K, Maurer D, Ozturk OG, Pruett TL, Bray RA, Gebel HM, Matas AJ. Revisiting traditional risk factors for rejection and graft loss after kidney transplantation. Am J Transplant. 2011;11:2132–2143. doi: 10.1111/j.1600-6143.2011.03640.x. [DOI] [PMC free article] [PubMed] [Google Scholar]