

Abstract
Silver nitrate is sometimes used as a means of chemical cauterization for control of minor bleeding and management of hypergranulation tissue following bedside head and neck procedures. There are only few reports available on the imaging appearance of silver nitrate and its potential to mimic a foreign body. We report a case of a patient presenting with dysphagia, odynophagia, and fever following dental work who had a peritonsillar incision and drainage for treatment of a deep neck space infection. During the procedure, silver nitrate was applied to halt the bleeding. Patient was subsequently transferred to another institution. Since the patient was not showing significant clinical improvement on antibiotic therapy, a computed tomography (CT) scan was performed demonstrating a hyperdense structure lodged in the pharyngeal mucosal space in the oropharynx and soft palate that was mistaken for a foreign body such as bone. Silver nitrate can have density similar to bone but does not have the normal architecture of bone with cortex and marrow on CT. Familiarity with the appearance of silver nitrate on CT, lack of bone architecture, and proper documentation and communication of the use of silver nitrate to the consultant radiologist and medical personnel could help avoid misdiagnosis and potentially unnecessary surgical exploration.
Keywords: Silver nitrate, Computed tomography, Bony foreign body, Soft tissues neck, Deep neck infections, Pharyngeal mucosal space
Core tip: This manuscript describes the imaging features of silver nitrate on computed tomography (CT). Silver nitrate is sometimes used as a means of chemical cauterization during bedside head and neck procedures. Silver nitrate has high attenuation on CT and has the potential to mimic a radio-opaque foreign body such as bone. However, it does not have the normal architecture of bone with cortex and marrow on CT. Familiarity with the appearance of silver nitrate on CT and proper communication of its use to the consultant radiologist could help avoid misinterpretation as a foreign body on imaging.
INTRODUCTION
Silver nitrate is a form of chemical cautery commonly used for control of minor hemorrhage in the head and neck and in the management of hypergranulation tissue. Only few case reports describe the radiographic appearance of silver nitrate and its potential for imitation of a foreign body. We report a case of silver nitrate residue within the pharyngeal mucosal space in the oropharynx and soft palate imitating a foreign body on computed tomography (CT) imaging. Knowledge of the radiographic appearance of silver nitrate as well communication and documentation of its use can help prevent misdiagnosis as a foreign body and unnecessary surgical exploration.
CASE REPORT
A 52-year-old man presented to an outside emergency department with dysphagia, odynophagia, and fever following recent dental work. On examination, the patient was febrile with a temperature of 38.6 °C and swelling and tenderness of the anterior triangle of the neck on the left. A CT scan of the neck was performed, demonstrating phlegmon involving the pharyngeal mucosal space and parapharyngeal space including phlegmon in the peritonsillar region with only minimal areas of liquefaction (Figure 1). Complete blood count demonstrated an elevated white count with left shift. An outside consultant incised the peritonsillar space to rule out a peritonsillar abscess. Intravenous antibiotic therapy was initiated, and the patient was transferred to our service the following day.
Figure 1.
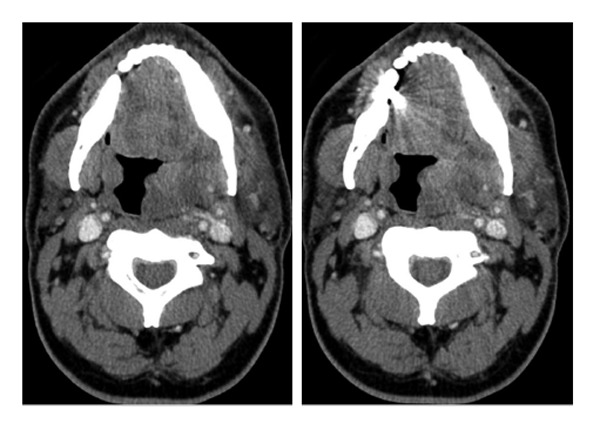
Axial computed tomography images at the level of the oropharynx prior to incision, drainage and silver nitrate application demonstrate swelling and enlargement of the left palatine tonsil and peritonsillar tissues with heterogeneous relatively low attenuation areas.
Forty eight hours later, the patient showed no significant improvement and therefore a repeat CT scan of the neck was performed. The scan demonstrated a linear hyperdense structure with irregular margins along the pharyngeal mucosal space in the oropharynx and soft palate (Figure 2). The density of the structure was between approximately 380 and 580 Hounsfield units. The possibility of a foreign body, such as a chicken bone, was entertained based on the appearance, even though typical bone architecture with cortex and medulla was not identified. The patient’s clinical history was, however, inconsistent with ingested foreign body impaction and its location was somewhat unusual. Furthermore, there was no sign of a foreign body on direct visualization. A thorough review of the management at the outside hospital was then performed, revealing that silver nitrate had been applied at the time of the peritonsillar incision for control of minor bleeding. A presumptive diagnosis of hyperdensity secondary to silver nitrate application was then made, supported by a literature review and identification of a few case reports describing that silver nitrate can be radiopaque on X-ray[1-3]. The patient’s outside CT scan obtained prior to peritonsillar incision was then obtained and revised at our institution, revealing no evidence of a foreign body. This confirmed that silver nitrate was the source of the hyperdense structure. Conservative management with intravenous antibiotic therapy and observation was continued. The patient’s symptoms resolved, and he was discharged 5 d following admission.
Figure 2.
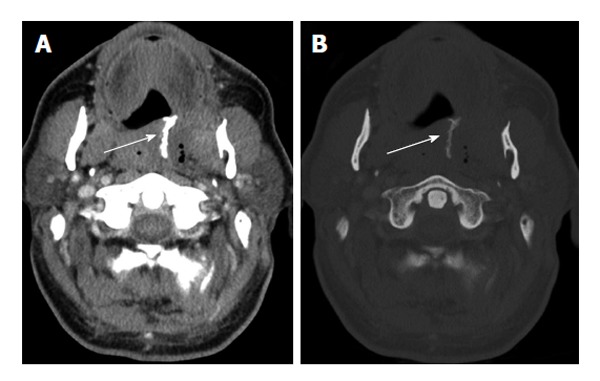
Axial computed tomography images from a scan performed 2 d after surgical exploration are shown, displayed in (A) soft tissue and (B) bone windows. The images demonstrate post-treatment changes with fluid and gas in the left palatine tonsil and peritonsillar region. In addition, there is a radiodense structure (arrow) in the pharyngeal mucosal space of the oropharynx and soft palate with density similar to bone, corresponding to the region of silver nitrate application. Note the absence of normal bone architecture such as cortex and medulla.
DISCUSSION
This report presents a case of a patient with a surgically explored pharyngeal mucosal space and peritonsillar region phlegmon who was not responding to treatment with the radiologic diagnosis confounded by silver nitrate application imitating a foreign body.
Infection of deep neck spaces can result in life threatening complications including airway compromise, sepsis, acute respiratory distress syndrome, jugular vein thrombosis, mediastinitis, disseminated intravascular coagulation, and death[4]. Foreign body trauma to the pharynx, dental infections, and oral surgical procedures are all known to initiate deep neck infections. CT scan is currently considered the gold standard imaging modality in the setting of a deep space neck infection. CT is widely available, can be obtained rapidly, and is helpful in identifying the etiology, establishing the extent of disease, and guiding the management of these patients.
Silver nitrate is an inorganic compound often used in emergency departments as topical chemical cautery due to its efficacy and ease of use. Silver nitrate is an oxidizing agent, producing free radicals and heat in aqueous solution, resulting in a necrosis and coagulation hemostasis[5]. Silver nitrate has also been used as an antiseptic for centuries, and has been shown to have antibacterial properties[6]. It is often used for coagulation of minor head and neck procedural bleeding. Importantly, silver nitrate is also radiopaque on X-ray[1-3].
There is a general lack of published literature regarding the radiographic appearance of silver nitrate, particularly on cross-sectional imaging and in the head and neck. To the best of our knowledge, there are 3 case reports describing the radiodense appearance of silver nitrate on plain radiographs of the extremities[1-3]. Madan et al[2] described a case of silver nitrate mimicking a foreign body on plain radiographs of the foot, where manual exploration was done and no foreign body found. Healy et al[1] reported two cases where silver nitrate was mistaken for a foreign body and/or dystrophic calcification on plain radiographs of the fingers[1]. Finally, Tong et al[3] reported a case of silver nitrate masquerading as an avulsion fracture or foreign body in the finger. The patient was managed conservatively and subsequent X-rays performed 2 wk later showed spontaneous resolution of the opacity. Our report appears to be the first case report describing the misleading appearance of silver nitrate both in terms of imaging modality (CT) and location in the soft tissues of the head and neck. In this case, we were able to avoid unnecessary pharyngeal exploration through careful analysis of the clinical context and CT images, supported by the limited medical literature on the topic.
This case highlights many important points. The use of silver nitrate in cauterizing soft tissue must be clearly documented and communicated to medical personnel, particularly in complex cases and those involving transfer of patient care to another institution. Furthermore, it is of special importance to communicate such history to the consultant radiologist. Although the lack of normal bone architecture in the hyperdensity reported raises the possibility of other etiologies as an imaging differential diagnosis, the provision of proper clinical information in such cases enables a much more confident diagnosis and helps avoid a misdiagnosis as a foreign body. This is of paramount importance in the context of pharyngeal mucosal space or parapharyngeal foreign bodies and deep space neck infections, where there is potential for unnecessary surgical exploration and associated morbidity for the patient. Given the widespread use of CT imaging in the evaluation and diagnosis of head and neck infections, it is important for radiologists and otolaryngologists to be familiar with the appearance of silver nitrate on CT and its potential to mimic radiodense foreign bodies and bone. Other imaging clues that may help avoid misdiagnosis include the absence of a typical bone structure such as cortex and medullary cavity.
COMMENTS
Case characteristics
Fifty five years old man transferred from another hospital post incision and drainage for a deep neck space infection who is not improving clinically on antibiotics.
Clinical diagnosis
Persistent swelling and pain in the neck without obvious abscess or foreign body on physical exam.
Differential diagnosis
Slowly resolving infection, infection resistant to antibiotic regimen, or infection complicated by abscess or other etiology such as foreign body.
Laboratory diagnosis
White blood cell count 16.1 × 109/L.
Imaging diagnosis
Computed tomography (CT) scan demonstrated a hyperdense linear structure along the pharyngeal mucosal space in the oropharynx and soft palate with density ranging between approximately 380 and 580 Hounsfield units that was initially interpreted as a potential foreign body such as bone. Re-review of the CT scan revealed no evidence of typical bone architecture, the patient’s clinical history was inconsistent with ingested foreign body, and there was no sign of a foreign body on direct visualization. A thorough review of the management at the outside hospital was then performed, revealing that silver nitrate had been applied at the time of the peritonsillar incision. The CT scan at the time of initial presentation was also subsequently obtained and did not demonstrate any evidence of foreign body prior to incision and drainage and application of silver nitrate.
Treatment
Conservative management with intravenous antibiotic therapy was continued and the patient’s symptoms resolved and patient discharged 5 d following admission.
Related reports
There are only few reports in the literature on silver nitrate mimicking foreign body on X-rays in the extremities. To the best of our knowledge, there are no descriptions of silver nitrate in the neck or on CT.
Term explanation
Silver nitrate is an inorganic compound often used in emergency departments as topical chemical cautery and also used for coagulation of bleeding associated with minor head and neck procedures.
Experiences and lessons
Awareness of the imaging appearance of silver nitrate and its use can prevent false diagnosis as a foreign body.
Peer-review
It is a well written case report.
Footnotes
P- Reviewer: Kamburoglu K, Triantopoulou C S- Editor: Ji FF L- Editor: A E- Editor: Liu SQ
Ethics approval: The study was reviewed and approved by the Institutional Review Board of the Jewish General Hospital and informed consent was waived.
Informed consent: The study was reviewed and approved by the Institutional Review Board of the Jewish General Hospital and informed consent was waived.
Conflict-of-interest: The authors do not have any conflict of interest to declare pertaining to this manuscript.
Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Peer-review started: December 26, 2014
First decision: January 8, 2015
Article in press: April 7, 2015
References
- 1.Healy C, Canney M, Murphy A, Regan P. Silver nitrate masquerading as a radiopaque foreign body. Emerg Radiol. 2007;14:63–64. doi: 10.1007/s10140-006-0542-4. [DOI] [PubMed] [Google Scholar]
- 2.Madan SI, Heilpern KL. Silver nitrate as a radiopaque foreign body. J Emerg Med. 1999;17:1045. doi: 10.1016/s0736-4679(99)00137-7. [DOI] [PubMed] [Google Scholar]
- 3.Tong SHY, Chan WL, Lee YL. Silver nitrate stain masquerading as an avulsion fracture of the finger. Hong Kong J Emerg Med. 2011;18:47–49. [Google Scholar]
- 4.Vieira F, Allen SM, Stocks RM, Thompson JW. Deep neck infection. Otolaryngol Clin North Am. 2008;41:459–483, vii. doi: 10.1016/j.otc.2008.01.002. [DOI] [PubMed] [Google Scholar]
- 5.Barr GD. Silver nitrate cautery and epistaxis. Arch Emerg Med. 1989;6:233. doi: 10.1136/emj.6.3.233. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Spacciapoli P, Buxton D, Rothstein D, Friden P. Antimicrobial activity of silver nitrate against periodontal pathogens. J Periodontal Res. 2001;36:108–113. doi: 10.1034/j.1600-0765.2001.360207.x. [DOI] [PubMed] [Google Scholar]