

Abstract
Background
Nasolabial flap (NLF) is one of the oldest described soft tissue flaps. Despite the great advances in maxillofacial reconstruction it still has a stable location in the reconstructive ladder of the face and oral cavity. Reconstruction of the lips, which are important structures that connect the oral cavity to the facial skin, with this flap is the interest of the surgeons.
Patients and Methods
Experience of the authors for reconstruction of the upper lip philtrum, correction of lower lip contracture and subtotal reconstruction of the lower lip with emphasis on simultaneous correction of the red lip (volume and color) is explained in five cases.
Results
Satisfactory functional and aesthetic results were obtained. Iatrogenic epidermoid cyst occurred in one patient.
Conclusion
One stage reconstruction of lateral lower lip defects with/without commissural involvement in full or partial thickness defects is possible by NLF. Supplementary flaps are needed when the vermilion needs simultaneous reconstruction.
Keywords: Nasolabial flap, Lip reconstruction, Philtrum
Introduction
Nasolabial flap (NLF) was introduced in 700 BC by Sushruta [1]. Since then it has been used for reconstruction of the facial skin in nasal reconstructions, alar reconstruction, skin dome replacement, and internal lining of the nose. Reconstruction of the skin in long axis of nasolabial fold as high as near the medial canthus can be done by this flap [2–6]. In oral cavity it is used to resurface anterior floor of the mouth defects, replacement of buccal mucosa, oronasal fistula closure in palate (anterior or posterior) and finally tongue reconstruction [7–10].
Usefulness of this flap in reconstruction of both lip defects is known capacity of this flap [11, 12]. In this article experience of the authors in this topic is presented and the ways to create the red zone over the transferred NLF in lower lip reconstructions are explained.
Patients and Methods
Experience of the authors for reconstruction of the upper lip philtrum, correction of lower lip contracture and subtotal reconstruction of the lower lip with emphasis on simultaneous correction of the red lip (volume and color) is explained in five cases.
Case 1
Reconstruction of the Philtrum
The patient was 27 year-old with bilateral cleft lip. The upper lip philtrum was hairless and distorted. The area was excised according to the subunit principles of the upper lip and the region was reconstructed with superiorly based subcutaneous island pedicled tunnelized NLF. Distal end of the flap was placed at hair bearing skin overlying the mandible and NLF was extended to include the hairs of the beard. The flap was deepithelialized at flap base then a subcutaneous tunnel was created between the nasolabial incision and prepared philtrum. The flap was transferred through the tunnel and sutured to the adjacent skin. Figure 1 shows the results.
Fig. 1.
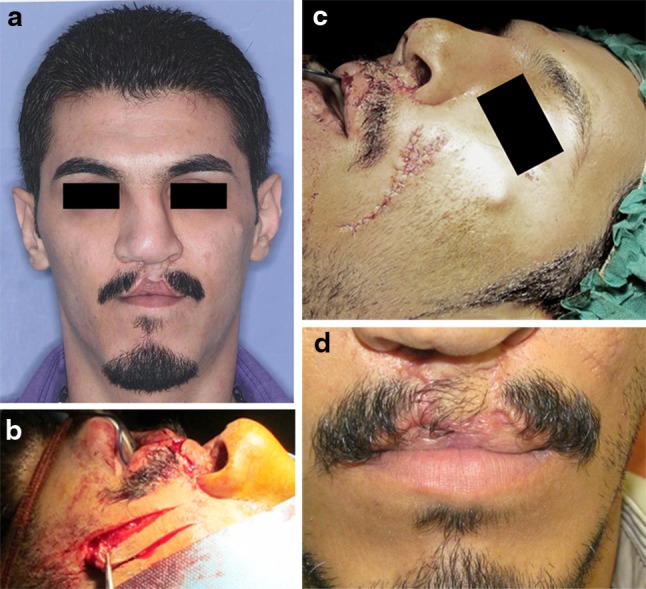
a Deformed philtrum in bilateral adult cleft lip patient. b Superiorly based subcutaneous NLF with inclusion of hair bearing skin. c Final results immediately after operation. d 2 years follow up
Case 2
Correction of the Lower Lip Downward slanting
The patient was a 22 year-old man. He experienced gunshot wound to the face with resulted through and through buccal composite defect. The region was reconstructed with submental island flap but scar contracture results in downward slanting of the lower lip. Superiorly based tunnelized subcutaneous island pedicled NLF was used for correction of this problem (Fig. 2).
Fig. 2.

a Downward slanting of lower lip. b Superiorly based subcutaneous NLF. c Deepithelialization at flap base. d Postoperative results immediately after operation. e Results 1 year later note inconspicuous skin scar
Case 3
Reconstruction of Full Thickness Lower Lip Defect (size = 50 % of Initial Lip Dimensions)
The patient was a 64 year-old man with biopsy proven verrucous carcinoma of the lower lip. The lesion was extended from left commissure to the midline. Lower limit of the lesion was mental crease. The patient preferred local anesthesia, so the lesion was resected with safety margins under this condition.
The defect was repaired by inferiorly based subcutaneous transposition pedicled NLF. For creating the red color and volume, over the NLF, vermilion advancement flap from unaffected side of the lip was elevated, advanced and covered the raw surface of the NLF (Fig. 3).
Fig. 3.

a Verrocous carcinoma of lower lip extends from left commissure to midline. b Inferiorly based musculocutaneous NLF concomitant with vermilion advancement flap. c Results 1 month after operation
Case 4
Reconstruction of Lower Lip Defect. (size = 60 % of Initial Lip Dimension)
The patient was a 54 year-old female with left lower labial skin basal cell carcinoma that had involved the left commissure and lateral lip segment.
The lesion was resected under general anesthesia. After resection with 5 mm safety margins, the resulted defect had large dimensions so inferiorly based musculo cutaneous NLF was used for reconstruction of the lost skin. Buccal mucosal transposition flap was used for red lip reconstruction (Fig. 4).
Fig. 4.

a Basal cell carcinoma of labial skin. b Inferiorly based musculotaneous NLF for reconstruction. c Hinged buccal mucosal flap for vermilion reconstruction. d Results of reconstruction 2 months postoperation
Case 5
Reconstruction of Left Lower Labial Partial Thickness Skin Defect
The patient was a 20 year-old man who had lost the skin of left lower labial region in a human bite attack.
After debridement and 2 weeks wet/dry dressing, inferiorly based subcutaneous NLF was used for reconstruction. The edge of the flap was deepithelialized and inserted below the skin edges of remaining lip skin to improve the bulk at the periphery.
The small segment of the vermilion that was avulsed in this event was reconstructed with mucosal V–Y advancement flap based on orbicularis oris muscle (Fig. 5).
Fig. 5.

a Lower lip skin defect resulted from human bite. b Part of NLF that interfers with red lip vermilion was removed. c Mucosal advancement flap based on orbicularis oris muscle. d Schematic picture. e Result immediately after operation. f Deepithelialized distal part of NLF for advancement below skin edges
Results
Post-operative period was uneventful except for one case of iatrogenic epidermoid cyst 3 years after surgery. Four of the five patients were males. NLF was used for reconstruction of the lips in five patients, three cases resulted from trauma and in two patients for reconstruction after pathologic resections. Difference in mean age of the patients in these two groups was 36 years. All patients were satisfied with the result of surgery.
Discussion
Reconstruction of the lips with their complex anatomy and function is a challenge [13]. Generally the reconstructive procedure depends on the size and location of the defect. Lower labial defects less than one-third of the lip can repair with primary closure while larger defects need local flap [14]. The skin of the face lateral to the nasolabial fold act as a reservoir for facial reconstructive procedures. The skin of this region is used in two flap designs: fan flap and NLF [15, 16].
NLF can be used combined with the other flaps, like, forehead, submental, webster, upper or lower lip switch, and platysma flap [17–21]. NLFs have been classified based on composition of the flap and blood supply (Table 1).
Table 1.
Classification of NLF based on composition of the flap
| Type of NLF | Composition |
|---|---|
| Subcutaneous NLF | S–SQ |
| Musculocutaneous NLF | S–SQ. Em |
| Full thickness NLF | S–SQ. Em–Bm |
| Deepithelialized NLF | Any thickness withought S |
S skin, SQ subcutaneous, Em expression muscles of the face, Bm buccal mucosa, NLF nasolabial flap
NLFs are used in forms of advancement, transposition, rotation, interpolated and tunnelized [22–26]. One stage lip reconstruction is possible by rotation, transposition, and tunnelized variants (Fig. 6).
Fig. 6.

Schematic picture of NLF for reconstruction of the lips. Rotation and transposition flaps in left and tunnelized NLF in right side of the picture are illustrated. Pivotal point (asterisk) for rotation and transposition NLF is superior to the oral commissure and in tunnelized NLF lateral to the nasal ala
In full thickness and musculocutaneous NLFs, if facial arteries are included in the flap design, then they are arterialized, and hence can be used with more reliability. Arterialized NLFs can be orthograde in inferiorly based and reverse flow in superiorly based NLFs (Fig. 7) [27, 28].
Fig. 7.
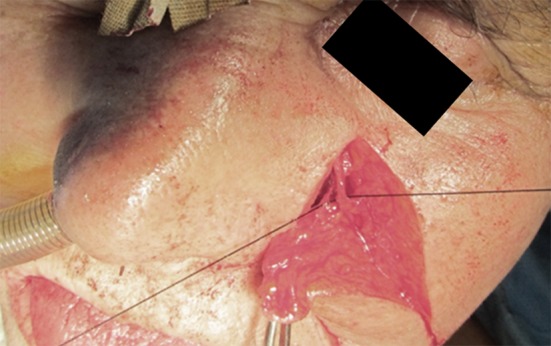
Arterialized NLF with inclusion of facial artery in flap
Deepithelialized variant of NLF is used for facial contouring, when the whole skin is removed from the flap (buried NLF) [29]. Proximal end deepithelialization changes pedicled NLF to island variant. Deepithelialized part of the flap can be sandwiched in subcutaneous tunnel to reach the defect site [30]. This will eliminate the need for second surgery for pedicle division that is necessary in interpolated NLFs.
Deepithelialization of distal part in NLF is indicated when the periphery of the defect opposite to the flap tip is depressed [31]. In deepithelialized variant, it is very important to remove all epithelium and hair follicles to prevent iatrogenic epidermoid cyst (Fig. 8).
Fig. 8.
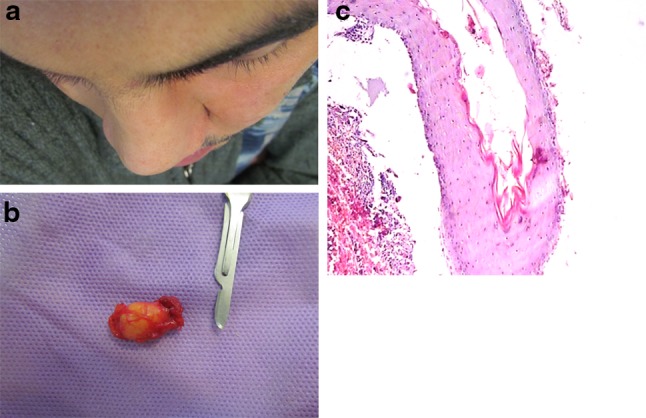
a Bulging at the base of NLF 3 years after surgery. b Excised lesion. c Keratin filled cystic cavity compatible with epidermoid cyst (H-E X × 100)
NLFs can have different thickness. It can be used for reconstruction of the lips with different tissue losses. Cases 1 and 2 need the least possible thickness, so including the subdermal vascular plexus was sufficient. In cases 3 and 4 NLF was used for reconstruction of full thickness lower lip defects, then bulkier flap was used.
Reconstruction of upper lip philtrum is a delicate procedure. Traumatic loss of this esthetic unit is reported in bite injuries and burns [32, 33]. Reconstruction of the philtrum in adult bilateral cleft patient with distorted hairless skin between upper vermilion and clomella is a very useful way to restore the lip balance. Abbe cross lip flap that corrects both vermilion and skin defects has no more application in this case [34]. Superiorly based NLFs for lifting up the lower lip is reported in traumatic events and correction of senile drooling [35, 36]. In our case (number 2) NLF not only had both effects of scar releasing and anchoring for the lower lip, but also had a Z-plasty effect.
In the last three cases where this flap was used for reconstruction of lower lip, the problem of the red lip was an integral part of reconstruction.
NLF cannot reconstruct the vermilion defect and reconstruction of this special unit had paramount importance to regain the lost esthetics. Suggested ways in this article are demonstrated at Table 2.
Table 2.
Suggested ways for one stage reconstruction of vermilion, simultaneous with NLF
| Indication | Suggested way | Example |
|---|---|---|
| Small red lip defects | Mucosal V–Y advancement flap based on orbicularis oris muscle | Case 5 |
| Remaining red vermilion equal to 50 % of total vermilion | Vermilion advancement flap | Case 3 |
| Remaining vermilion less than 50 % of total vermilion | Hinged buccal mucosal flap | Case 4 |
Vermilion advancement flap was introduced by Goldstein [37]. In classic form, this flap is useful for reconstruction of the vermilion concomitant with NLF when the lip defect is not full thickness and labial mucosa forms the inner lining. NLF reconstructs the bulk of resection and Goldstein flap makes the red lip.
When full thickness lip defect is present and NLF concomitant with classic vermilion flap is used to reconstruct the inner surface of the defect, raw surface of NLF undergoes secondary epithelialization with resulted obliteration of the vestibular depth. In such situations, full thickness NLF with inclusion of buccal mucosa or modification of vermilion advancement flap that includes labial mucosa of the lip with vermilion flap (Split Lip Advancement Technique) is recommended [38]. This technique was first described for treatment of congenital sinuses of the lower lip, but found its way in red lip reconstruction after pathologic resections [39, 40].
If there is more demand for red lip bulk, the tongue flaps from the ventral surface and facial artery musculomucosal flap (FAMM) with anterior base is recommended [41, 42]. Medical tattooing is also a useful aid in this topic [43].
NLF can be used for reconstruction of central lower lip defects in the form of bilateral interpolated flap or in near total lower lip reconstruction [44]. In these situations the left and right NLFs are sutured together in midline, edge to edge or top to bottom.
Limitations and benefits of NLF for reconstruction of the lips are listed at Table 3. One major drawback in NLF for lower lip reconstruction when it is used to replace the orbicularis oris muscle fibers is that circumoral sphincter function cannot be obtained [45]. Although full thickness and musculocutaneous NLFs contain muscle fibres of lavator labii superioris and levator labi superior alaeque nasi and electromyographic evaluation showed increased activity when this variant was used for lower lip reconstruction, but does not provide the sphincter function of orbicularis oris specially during the functions of eating and speaking [46]. Despite this limitation, in practice there is actually little concern about this problem.
Table 3.
Limitations and benefits in NLF reconstruction of lip defects
| Limitation | Benefit |
|---|---|
| Skin scar specially in young patients | Old age patients with medically compromised conditions |
| Asymmetry in unilateral cases | Concomitant with neck dissection |
| Not providing sphincter function | Previous radiotherapy is not problematic |
| Provides different thickness | |
| Inability to reconstruct the red lip | Excellent color and texture match for external skin |
| Completely denervated flap | Possibility of doing surgery under local anesthesia |
Reconstruction of external lip skin with NLF in males, specially in genders with heavy beards, create patchy appearance. These patients should be alerted about this condition and the hair of the beard around the reconstructed area should be shaved every day.
Conclusion
In this article usefulness of NLF for reconstruction of lip defects from small partial thickness to large full thickness labial defects is demonstrated. One stage reconstruction of lateral lower lip defects with/without commissural involvement in full or partial thickness defects is possible by NLF. Supplementary flaps are needed when the vermilion needs simultaneous reconstruction.
Acknowledgments
This study was supported by a grant from the Vice Chancellor of Research of Mashhad University of Medical Sciences.
Conflict of interest
None.
Contributor Information
Amin Rahpeyma, Phone: +98-511-8829501, FAX: +98-511-8829500, Email: rahpeymaa@mums.ac.ir.
Saeedeh khajehahmadi, Phone: +98-511-8829501, Email: khajehahmadis@mums.ac.ir.
References
- 1.Schmidt BL, Dierks EJ. The nasolabial flap. Oral Maxillofac Surg Clin North Am. 2003;15:487–495. doi: 10.1016/S1042-3699(03)00063-3. [DOI] [PubMed] [Google Scholar]
- 2.Köse R, Okur MI. Reconstruction of the defects in the middle of the nose with subcutaneous pedicled nasolabial island flap: report of two cases. Kulak Burun Bogaz Ihtis Derg. 2009;19:272–276. [PubMed] [Google Scholar]
- 3.Sohn WI, Choi JY, Seo BF, Jung SN. Reconstruction of nasal ala with nasolabial perforator flap after cancer removal. Head Neck Oncol. 2012;4:83. [Google Scholar]
- 4.Thornton JF, Weathers WM. Nasolabial flap for nasal tip reconstruction. Plast Reconstr Surg. 2008;122:775–781. doi: 10.1097/PRS.0b013e318182370b. [DOI] [PubMed] [Google Scholar]
- 5.Meyer TN. The nasolabial flap for nasal lining defects. Plast Reconstr Surg. 2002;109:400. doi: 10.1097/00006534-200201000-00074. [DOI] [PubMed] [Google Scholar]
- 6.Zhang Y, Wu HL, Lu YM. Contralateral nasolabial flap for reconstruction of midface defects. Aesthetic Plast Surg. 2012;36:1175–1178. doi: 10.1007/s00266-012-9943-9. [DOI] [PubMed] [Google Scholar]
- 7.El-Marakby HH, Fouad FA, Ali AH. One stage reconstruction of the floor of the mouth with a subcutaneous pedicled nasolabial flap. J Egypt Natl Canc Inst. 2012;24:71–76. doi: 10.1016/j.jnci.2012.02.002. [DOI] [PubMed] [Google Scholar]
- 8.Lazaridis N, Tilaveridis I, Karakasis D. Superiorly or inferiorly based “islanded” nasolabial flap for buccal mucosa defects reconstruction. J Oral Maxillofac Surg. 2008;66:7–15. doi: 10.1016/j.joms.2006.06.285. [DOI] [PubMed] [Google Scholar]
- 9.Govila A. Nasolabial myocutaneous island flap for reconstruction of palatal fistula (a case report) Acta Chir Plast. 1990;32:40–45. [PubMed] [Google Scholar]
- 10.Varghese BT, Sebastian P, Cherian T, Mohan PM, Ahmed I, Koshy CM, Thomas S. Nasolabial flaps in oral reconstruction: an analysis of 224 cases. Br J Plast Surg. 2001;54:499–503. doi: 10.1054/bjps.2001.3651. [DOI] [PubMed] [Google Scholar]
- 11.Cook JL. The reconstruction of two large full-thickness wounds of the upper lip with different operative techniques: when possible, a local flap repair is preferable to reconstruction with free tissue transfer. Dermatol Surg. 2013;39:281–289. doi: 10.1111/dsu.12033. [DOI] [PubMed] [Google Scholar]
- 12.Chiummariello S, Angelisanti M, Somma F, Calzoni C, Arleo S, Alfano C. Reconstruction of full-thickness loss of substance of lower lip. Our experience. Ann Ital Chir. 2012;83:325–330. [PubMed] [Google Scholar]
- 13.Calhoun KH. Reconstruction of small- and medium-sized defects of the lower lip. Am J Otolaryngol. 1992;13:16–22. doi: 10.1016/0196-0709(92)90093-9. [DOI] [PubMed] [Google Scholar]
- 14.Harris L, Higgins K, Enepekides D. Local flap reconstruction of acquired lip defects. Curr Opin Otolaryngol Head Neck Surg. 2012;20:254–261. doi: 10.1097/MOO.0b013e3283557dcf. [DOI] [PubMed] [Google Scholar]
- 15.Nakajima T, Yoshimura Y, Kami T. Reconstruction of the lower lip with a fan-shaped flap based on the facial artery. Br J Plast Surg. 1984;37:52–54. doi: 10.1016/0007-1226(84)90042-0. [DOI] [PubMed] [Google Scholar]
- 16.Tei TM, Larsen J. Use of the subcutaneously based nasolabial flap in lower eyelid reconstruction. Br J Plast Surg. 2003;56:420–423. doi: 10.1016/S0007-1226(03)00179-6. [DOI] [PubMed] [Google Scholar]
- 17.Paddack AC, Frank RW, Spencer HJ, Key JM, Vural E. Outcomes of paramedian forehead and nasolabial interpolation flaps in nasal reconstruction. Arch Otolaryngol Head Neck Surg. 2012;138:367–371. doi: 10.1001/archoto.2012.69. [DOI] [PubMed] [Google Scholar]
- 18.Daya M, Mahomva O, Madaree A. Multistaged reconstruction of the oral commissures and upper and lower lip with an island submental flap and a nasolabial flap. Plast Reconstr Surg. 2001;108:968–971. doi: 10.1097/00006534-200109150-00023. [DOI] [PubMed] [Google Scholar]
- 19.Minagawa T, Maeda T, Shioya R. Esthetic and safe lower lip reconstruction of an asymmetric defect due to cancer resection: a modified Webster method combined with a nasolabial flap. J Oral Maxillofac Surg. 2011;69:e256–e259. doi: 10.1016/j.joms.2011.01.007. [DOI] [PubMed] [Google Scholar]
- 20.Panje WR. Lip reconstruction. Otolaryngol Clin North Am. 1982;15:169–178. [PubMed] [Google Scholar]
- 21.Yeo JF, Egyedi P. Reconstruction of soft tissues of the chin and lower lip region following excision of a basal cell carcinoma. J Craniomaxillofac Surg. 1988;16:337–339. doi: 10.1016/S1010-5182(88)80074-X. [DOI] [PubMed] [Google Scholar]
- 22.El-Marakby HH. The versatile naso-labial flaps in facial reconstruction. J Egypt Natl Canc Inst. 2005;17:245–250. [PubMed] [Google Scholar]
- 23.Aslan A, Ozkan AC, Aydin H, Koldaş T, Tunçer S. Orocutaneous fistula arising secondary to irritation of an external dental prosthesis and its reconstruction using a nasolabial island flap. Ann Plast Surg. 2001;47:95–96. doi: 10.1097/00000637-200107000-00022. [DOI] [PubMed] [Google Scholar]
- 24.Burget GC, Hsiao YC. Nasolabial rotation flaps based on the upper lateral lip subunit for superficial and large defects of the upper lateral lip. Plast Reconstr Surg. 2012;130:556–560. doi: 10.1097/PRS.0b013e31825dc09f. [DOI] [PubMed] [Google Scholar]
- 25.Pharis DB, Papadopoulos DJ. Superiorly based nasolabial interpolation flap for repair of complex nasal tip defects. Dermatol Surg. 2000;26:19–24. doi: 10.1046/j.1524-4725.2000.99057.x. [DOI] [PubMed] [Google Scholar]
- 26.Georgiade NG, Mladick RA, Thorne FL. The nasolabial tunnel flap. Plast Reconstr Surg. 1969;43:463–466. doi: 10.1097/00006534-196905000-00002. [DOI] [PubMed] [Google Scholar]
- 27.Pochet F, Gueganton C, Gas C, Collin JF, Combelles R. Use of reverse blood flow vascular island nasolabial pedicle flap in the repair of the columella. Ann Chir Plast Esthet. 1994;39:785–788. [PubMed] [Google Scholar]
- 28.Le-Quang C. Reversed vascular full-thickness nasolabial flap. Ann Chir Plast Esthet. 1994;38:273–278. [PubMed] [Google Scholar]
- 29.Toomey JM, Spector CJ. The buried nasolabial flap. Laryngoscope. 1979;89:847–848. doi: 10.1288/00005537-197905000-00026. [DOI] [PubMed] [Google Scholar]
- 30.Rifaat MA. Lower lip reconstruction after tumor resection; a single author’s experience with various methods. J Egypt Natl Canc Inst. 2006;18:323–333. [PubMed] [Google Scholar]
- 31.Jin X, Teng L, Lu J, Xu J, Zhang C, Xu M, Zhao J. Upper-lip vermilion reconstruction with a modified cross-lip vermilion flap in hemifacial atrophy. J Plast Reconstr Aesthet Surg. 2013;66:e101–e106. doi: 10.1016/j.bjps.2012.12.012. [DOI] [PubMed] [Google Scholar]
- 32.Bento M, Carmo L, Trigo M, Rebelo N, Garcia P. The island nasolabial flap in philtrum reconstruction after bite avulsion: a case report. J Plast Reconstr Aesthet Surg. 2009;62:e487–e489. doi: 10.1016/j.bjps.2008.08.069. [DOI] [PubMed] [Google Scholar]
- 33.Tirone L, Moscatiello F, Molea G. Reconstruction of the upper lip and philtrum. J Plast Reconstr Aesthet Surg. 2006;59:865–866. doi: 10.1016/j.bjps.2005.11.025. [DOI] [PubMed] [Google Scholar]
- 34.Raschke GF, Rieger UM, Bader RD, Schultze-Mosgau S. Lip reconstruction: an anthropometric and functional analysis of surgical outcomes. Int J Oral Maxillofac Surg. 2012;41:744–750. doi: 10.1016/j.ijom.2012.02.005. [DOI] [PubMed] [Google Scholar]
- 35.Parsons RW, Beckwith MM, Thering HR. Surgical rehabilitation after extensive losses in the lower face from war injuries. Plast Reconstr Surg. 1972;49:533–536. doi: 10.1097/00006534-197205000-00010. [DOI] [PubMed] [Google Scholar]
- 36.Pacifico MD, Ritz M. Correction of senile drooling using the nasolabial sling. J Plast Reconstr Aesthet Surg. 2010;63:757–762. doi: 10.1016/j.bjps.2009.01.061. [DOI] [PubMed] [Google Scholar]
- 37.Goldstein MH. The elastic flap for lip repair. Plast Reconstr Surg. 1990;85:446–452. doi: 10.1097/00006534-199003000-00021. [DOI] [PubMed] [Google Scholar]
- 38.Mutaf M, Sensöz O, Ustüner ET. The split-lip advancement technique (SLAT) for the treatment of congenital sinuses of the lower lip. Plast Reconstr Surg. 1993;92:615–620. doi: 10.1097/00006534-199309001-00009. [DOI] [PubMed] [Google Scholar]
- 39.Tokat C, Bilkay U, Songur E, Akin Y. Van der Woude syndrome in twins. J Craniofac Surg. 2005;16:936–939. doi: 10.1097/01.scs.0000168777.01851.cd. [DOI] [PubMed] [Google Scholar]
- 40.Alvarez GS, Siqueira EJ, de Oliveira MP. A new technique for reconstruction of lower-lip and labial commissure defects: a proposal for the association of Abbe-Estlander and vermilion myomucosal flap techniques. Oral Surg Oral Med Oral Pathol Oral Radiol. 2013;115:724–730. doi: 10.1016/j.oooo.2012.10.009. [DOI] [PubMed] [Google Scholar]
- 41.Kheradmand AA, Garajei A. Ventral tongue myomucosal flap: a suitable choice for shaved lower vermilion border reconstruction. J Craniofac Surg. 2013;24:e114–e116. doi: 10.1097/SCS.0b013e31826683f6. [DOI] [PubMed] [Google Scholar]
- 42.Sacak B, Gurunluoglu R (2013) The innervated gracilis muscle for microsurgical functional lip reconstruction: review of the literature. Ann Plast Surg [DOI] [PubMed]
- 43.Furuta S, Hataya Y, Watanabe T, Yuzuriha S. Vermilion plasty using medical tattooing after radical forearm flap. Br J Plast Surg. 1994;47:422–424. doi: 10.1016/0007-1226(94)90071-X. [DOI] [PubMed] [Google Scholar]
- 44.Sun G, Lu M, Hu Q. Reconstruction of extensive lip and perioral defects after tumor excision. J Craniofac Surg. 2013;24:360–362. doi: 10.1097/SCS.0b013e318267bb98. [DOI] [PubMed] [Google Scholar]
- 45.Spinelli HM, Tabatabai N, Muzaffar AR, Isenberg JS. Upper lip reconstruction with the alar crescent flap: a new approach. J Oral Maxillofac Surg. 2006;64:1566–1570. doi: 10.1016/j.joms.2005.12.031. [DOI] [PubMed] [Google Scholar]
- 46.Tan NC, Hsieh CH, Riva FM, Jeng SF. Nasolabial flap as a one-stage procedure for reconstruction of intermediate-to-large lip defects with functional and aesthetic assessments. J Plast Reconstr Aesthet Surg. 2013;66:352–357. doi: 10.1016/j.bjps.2012.10.008. [DOI] [PubMed] [Google Scholar]