

Abstract
Tongue Drive System (TDS) is a wireless tongue-operated assistive technology (AT), developed for people with severe physical impediments to control their environments using their tongue motion. We have developed a new intraoral TDS (iTDS) in a form of a dental retainer, which can tightly clasp onto the upper teeth, completely hidden inside the mouth, using commercial off-the-shelf components (COTS). The iTDS retainer was tested by two healthy subjects and their performance was compared with that of an external TDS (eTDS) implemented in the form of a headset. The iTDS retainer showed comparable performance with the eTDS headset. The iTDS is expected to improve the stability and robustness of the TDS, while giving users a certain degree of privacy.
I. Introduction
Tongue Drive System (TDS) is a wireless assistive technology (AT), which utilizes the voluntary movements of the tongue and enables its users to control their environments. This system wirelessly and unobtrusively detects the position of a small permanent magnetic tracer, secured on the tongue via tissue adhesives or piercing, and translates a set of user-defined tongue positions and gestures into specific user-defined tongue commands [1].
We have successfully proven the TDS functionality using the external TDS (eTDS) headset in various experimental setups involving both able-bodied subjects and people with high-level spinal cord injury (SCI) in clinical trials [2], [3]. We evaluated the eTDS in several computer access and power wheelchair navigation tasks. We concluded that the in general TDS has several advantages over other ATs, such as sip and puff, eye trackers, head pointers, electromyography (EMG) switches, and voice recognition software [4], [5].
Nevertheless, in certain real-life conditions, such as being on a bumpy road or colliding with objects, the eTDS headset may show mechanical stability issues due to the poor stability of the headset on the head. If the sensor positions on the headset are shifted with respect to the tongue position by more than a few mm, the eTDS may lose its calibration and misclassify the user commands. Furthermore, wearing the eTDS headset over long periods may not be comfortable, or some users may be sensitive to its appearance despite the fact that it looks like a fashionable music headset [6].
For these reasons, the intraoral TDS (iTDS) has been developed in a form of a dental retainer to be mounted under the palate inside the user’s mouth. The iTDS is mechanically more robust than the eTDS because it can tightly clasp onto the upper teeth, and be protected inside the mouth. Also, being completely hidden in the mouth, it gives the user a certain degree of privacy, and does not become a sign of disability. The first iTDS prototype was implemented in the form of an application specific integrated circuit (ASIC) and reported in [7]. That approach can result in the most features embedded in the smallest possible space. However, the cost of developing ASICs in a small scale can be quite high. In this paper, we introduce a new version of the iTDS that only utilizes commercial off-the-shelf (COTS) components, and communicates with an external receiver (Rx) via a 2.4 GHz wireless link. Despite more absorption in the tissue compared with the 27/432 MHz bands used in the ASIC version, the size of the optimal antenna at 2.4 GHz can be smaller.
II. iTDS Hardware Implementation
The iTDS hardware has been implemented on a small trapezoidal PCB, shown in Fig. 1. It consists of a CC2510 (Texas Instrument, Dallas, TX), which is a system-on-chip that integrates a microcontroller and an RF transceiver, four AMI306 digital magnetic sensors (Aichi-Steel, Japan) located at each vertex, and a charging coil on one side of the PCB. Additionally, there are a 2.4 GHz spiral antenna, a rechargeable Li-Ion polymer battery (3.7 V, 110 mAh, 18×24×3.5 mm3), a charging indicator LED, and a battery charging circuitry on the other side of the PCB. The entire PCB is smaller than 20×35 mm2 and it is designed in the form of a trapezoid to easily fit inside a dental retainer.
Fig. 1.
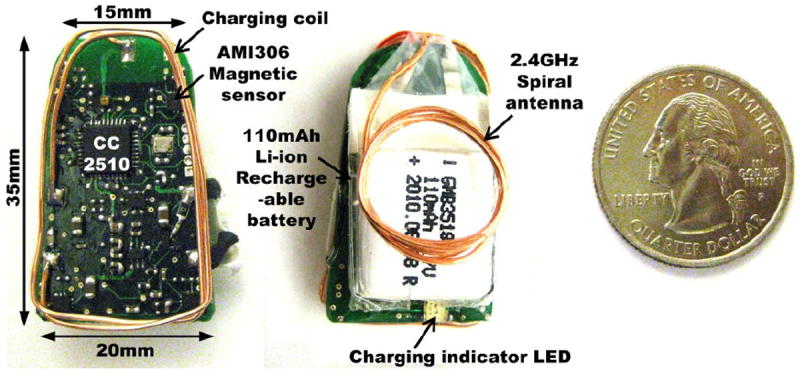
iTDS circuitry implemented on a small trapezoidal PCB.
Four AMI306 3-axial digital magnetic sensors measure the magnetic field strength at their locations and digitize it with 12-bit resolution. This leads to a total of 12 measurements. The CC2510 collects the magnetic field data from the sensors and transmits them inside a 28-byte packet via its built-in 2.4 GHz ISM band transceiver. The Li-Ion polymer battery is rechargeable through a 13.56 MHz inductive link, formed between the charging coil embedded in the iTDS and an external coil that is connected to an RFID reader. The wireless charging capability is vital for the iTDS because there is no direct connection available after the iTDS is molded and hermetically sealed inside the dental retainer.
The iTDS circuits are coated with silicone or Parylene to be water resistant and molded inside the dental retainer, as shown in Fig. 2. The retainer is made of dental acrylic resin, which is commonly used in orthodontic appliances. With this dual coating, the iTDS circuitry is expected to be protected from leakage and risks of electrostatic discharge. However, we have not tested its lifetime in the harsh oral environment yet. The iTDS dental retainer is built based on the user’s dental impression to perfectly fit his/her oral anatomy, and currently occupy 18-20 mL of space. The retainer tightly secures onto the upper teeth with four ball clasps.
Fig. 2.
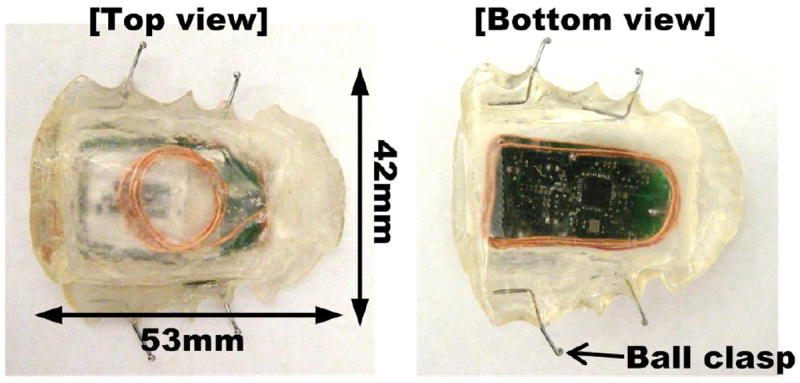
iTDS electronics molded inside an acrylic dental retainer.
Fig. 3 shows the iTDS block diagram. It also includes a customized external Rx, which wirelessly receives the iTDS sensors’ data using a second CC2510. It also provides an interface to communicate with PC or smartphone.
Fig. 3.
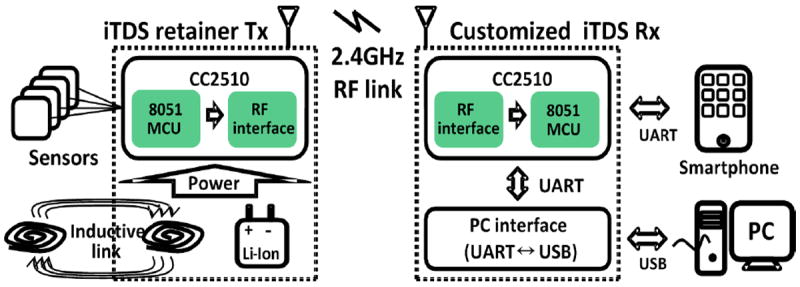
Simplified iTDS block diagram.
Fig. 4 shows similar hardware for the eTDS headset, implemented on a pair of small bean-shaped PCBs with sensor on two separate PCBs. The eTDS headset incorporates the same microcontroller with RF transceiver, a chip antenna, and magnetic sensors. However, there is a slight difference in the charging circuitry and the antenna because the eTDS headset does not have to be charged inductively and the efficiency of the chip antenna is sufficient for the eTDS headset, since it is not surrounded by the oral tissue.
Fig. 4.
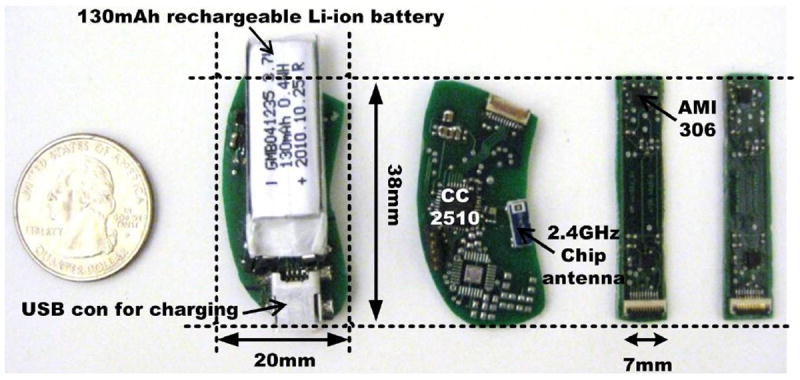
eTDS circuitry including a rechargeable battery and 4 sensors.
III. Methods
To evaluate the performance of the new iTDS retainer, two healthy subjects, one male and one female, aged 32 and 27 years old, respectively, conducted 6-command training, center-out tapping task, and maze-navigation task, similar to [8]. They used the iTDS retainers that were customized for their oral anatomies by a dental technician. The same subjects also conducted the same tasks with the latest eTDS headset prototype to compare its performance with the iTDS retainer. Both subjects (co-authors of this article) had prior experience with the eTDS operation and knew its technical details. This preliminary experiment was meant to show whether the iTDS was ready for more extensive trials in a clinical setting [3]. A secondary purpose of the trial was to compare the robustness of the iTDS retainer with the eTDS headset for real-life conditions. For this purpose, we added a walking task in between two successive trials to observe the effects of inertial forces and mechanical vibrations. End users sitting on wheelchairs experience such interferences when driving on a bumpy road or when they are onboard a vehicle.
The test setup for the iTDS trial is shown in Fig. 5. A small magnetic tracer was attached to the subject’s tongue using dental adhesives (Cyanoacrylate, GluStitch, Point Roberts, WA). The graphical user interface (GUI) was developed in the LabVIEW environment and presented to the subjects sitting ~1 m away from a 22” LCD monitor with 1280 × 800 pixel resolution. The task window was a white 610 × 610 pixel square in the center. Details of tongue positions that were considered as TDS commands can be found in [2], [8].
Fig. 5.
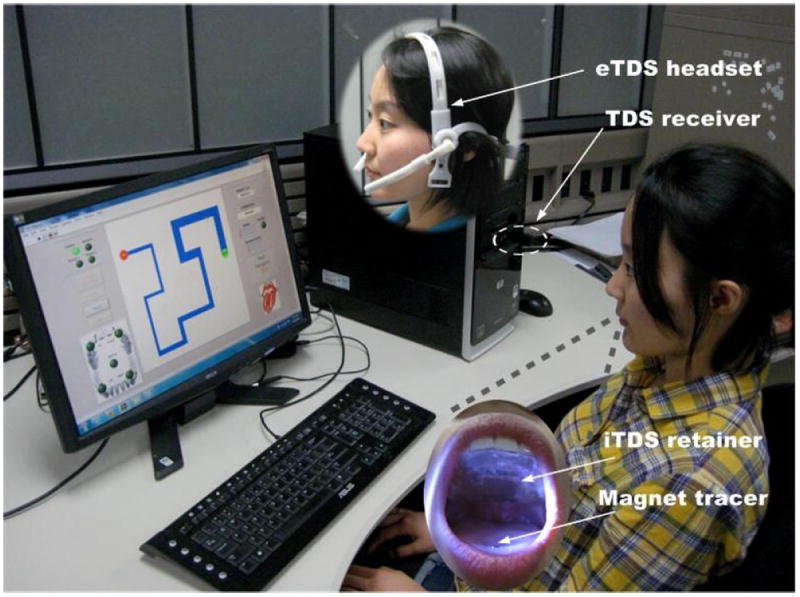
Test setup for the iTDS dental retainer and the eTDS headset.
In the 6-command training, subjects were asked to issue each TDS command (left, right, up, down, left-click, double-click), plus the tongue resting position as the neutral command, ten times while the PC saved the magnetic sensor data. A principle component analysis (PCA) maps the raw data onto a 3D feature space. Considering the fact that sensors on the iTDS retainer are much closer to the magnet on the tongue than the eTDS headset, we used disk-shaped permanent magnetic tracers (K&J Magnetics, Jamison, PA) with different sizes for each case. Table I summarizes the specifications of these magnetic tracers.
Table I.
Disk-Shaped Permanent Magnetic Tracer Specifications*
| Device | Diameter (mm) | Thickness (mm) | Material | Surface field (Gauss) | Brmax (Gauss) |
|---|---|---|---|---|---|
| eTDS | 4.8 | 1.5 | NdFeB – N52 | 4022 | 14800 |
| iTDS | 3.2 | 0.8 | NdFeB – N52 | 3309 | 14800 |
Source: http://www.kjmagnetics.com/
In the center-out tapping task, circular targets with three different diameters (W = 30, 61, and 122 pixels) and three different distances from the center of the screen (D = 61, 122, and 244 pixels) generated 6 D-W pair conditions. Each trial began with the cursor at the center and targets appeared randomly on the screen, one at a time, as shown in Fig. 6a. Using the iTDS/eTDS, subjects moved the mouse pointer towards the target and issued a mouse click command as close as possible to the center of the target for 48 times per round (8 per D-W pair). The task was repeated for four rounds and parameters including throughout (speed and accuracy), completion time, and error rate were calculated similar to [8].
Fig. 6.
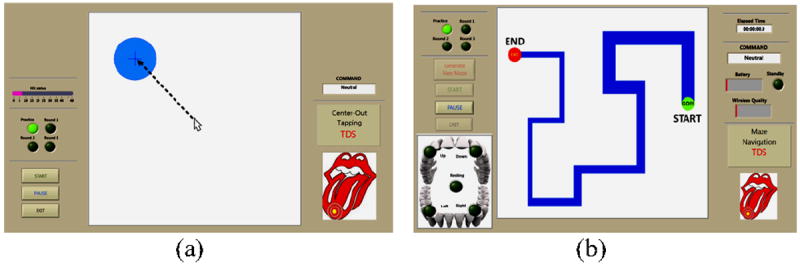
GUIs for the well-known (a) center-out tapping and (b) maze-navigation tasks, similar to what was reported in [8].
In the maze-navigation task, the maze pattern was randomly selected from a set of 8 predefined patterns and showed on the screen as a blue path in Fig. 6b. Using the iTDS, subjects were instructed to move the cursor as quickly as possible while keeping the cursor within the blue track through the maze, from the START green circle to the END red circle and issue a tongue click. Each subject was asked to complete four rounds of maze-navigation task with different maze patterns to eliminate the learning bias. Measured and calculated parameters included completion time and deviation from the path, as described in [8].
Following the 1st set of trials, subjects were asked to walk four flights of stairs up and down (192 steps in total), while wearing either the iTDS retainer or eTDS headset. Subjects then performed the 2nd set of trials, consisting of four rounds of the center-out tapping and maze- navigation tasks, without re-calibrating or re-training the system.
IV. Experimental Results
Fig. 7 shows the PCA spaces generated from the 6-command training of one of the subjects with the iTDS retainer and eTDS headset. There is also a 7th cluster for the tongue resting position, which is considered neutral. They show that the command clusters are separated enough to be easily distinguishable from each other in the sensor signal processing algorithm (SSP). Based on the two figures-of-merit (FoM) defined in [9], the clusters shown in Figs. 7a and 7b show FoM1/FoM2 of 18.2/21.2 and 42.9/30.8 for the iTDS and eTDS, respectively, which are within the acceptable range for both systems.
Fig. 7.
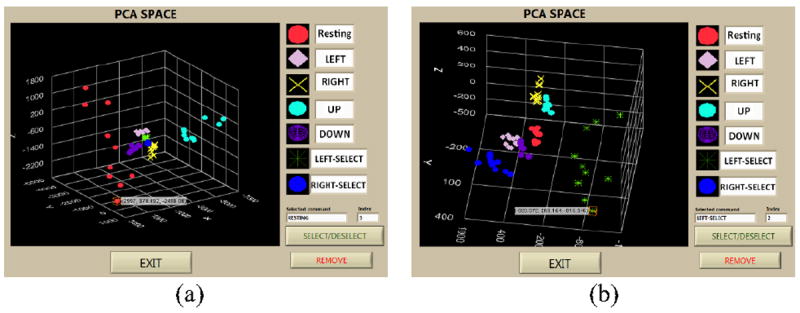
Separated dots corresponding to each command in virtual 3D space obtained from (a) the iTDS retainer and (b) the eTDS headset
Every cursor trace navigated by the users was recorded for further analysis, as shown in Fig. 8. Figs. 9 and 10 summarize the results obtained from the center-out tapping and maze-navigation tasks, respectively, for two sets of trials before and after walking. In order to check the validity of the experimental results, we compared the eTDS throughput from this experiment for the center-out tapping task before walking the stairs with the results from a similar task in the last (5th) session of a similar task in our previous publication [8]. The former resulted in 1.58 bits/s vs. 1.5 bits/s, reported in the latter. Therefore, considering the familiarity of the subjects in the current trial with the eTDS, the experimental results seem to be valid and in agreement with prior human subject trials.
Fig. 8.
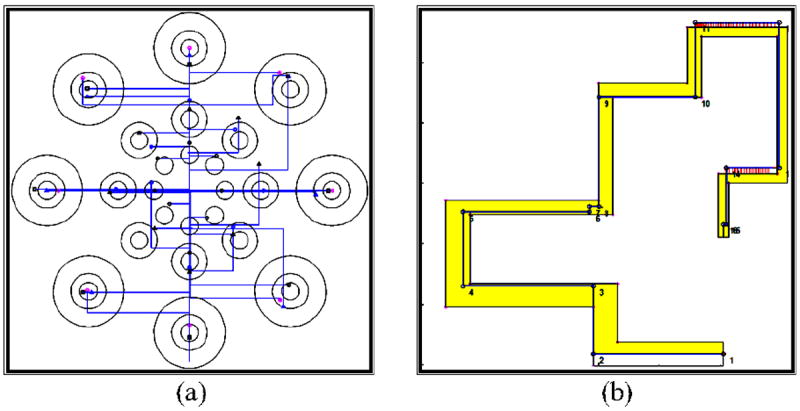
Example of the recorded mouse cursor traces of a subject in the (a) center-out tapping and (b) maze navigation tasks.
Fig. 9.
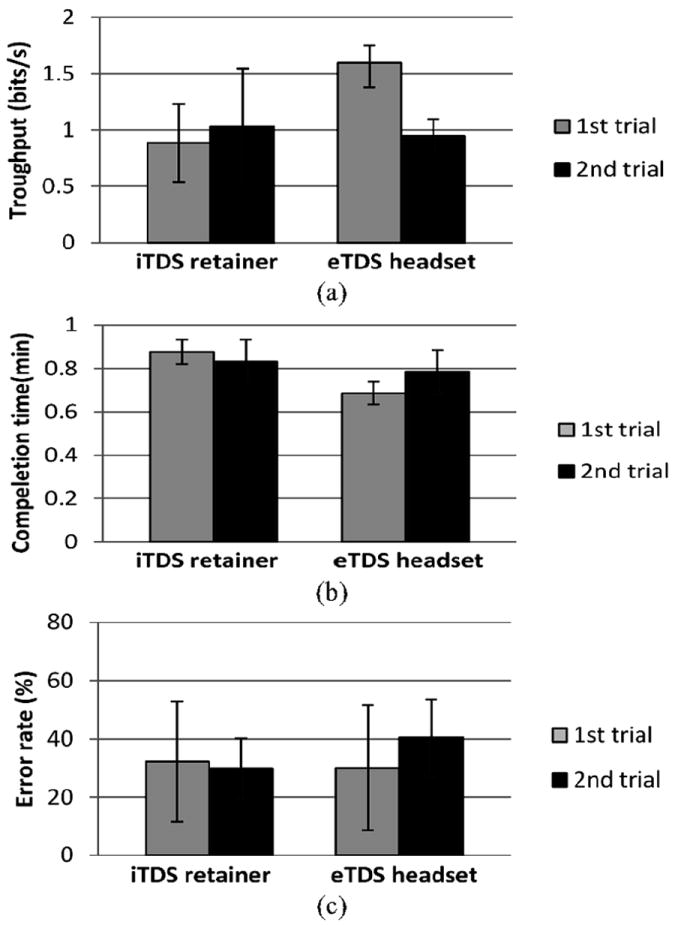
Results for the center-out tapping task: (a) Throughput, (b) Completion time, and (c) Error rate. For definitions of these parameters please refer to [8].
Fig. 10.
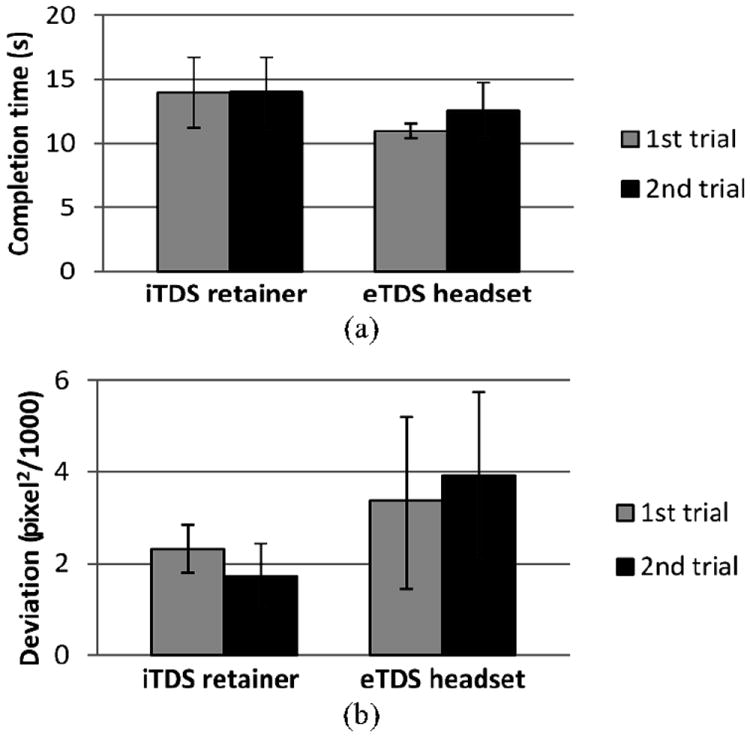
Results for the maze navigation task: (a) Completion time and (b) Deviation from the path. For definitions please refer to [8].
Results from the 1st trial, before walking, show that the subjects’ performance with the eTDS headset is better than the iTDS retainer in every measure of the center-out tapping task. In the maze-navigation task, however, the performances are more or less the same, within the measurement errors. This can be attributed to the following reasons: 1) subjects were more familiar with the eTDS than the iTDS; 2) the quality of trainings, i.e. separation between the command clusters in the eTDS were better than the iTDS, resulting in higher FoM1 and FoM2; and 3) the iTDS dental retainer occupied 18.7% and 19% of the two subjects’ oral spaces, leaving less room for their tongue movements.
The robustness of the iTDS retainer was, however, better than the eTDS headset, considering the test result from before and after walking (gray vs. black bars in Figs. 9 and 10). For the iTDS, every performance measure stayed almost the same or even slightly improved. Every measure for the eTDS, on the other hand, was degraded in the 2nd set of trials.
V. Conclusion
A new iTDS prototype was designed and built using only COTS components, and molded inside a dental retainer made of the user’s dental impression. The subjects’ performance was measured with both eTDS and iTDS based on the separation between TDS commands in the PC A feature space after training, as well as the speed- accuracy measures through well-known center-out tapping and maze-navigation tasks. The iTDS retainer shows approximately the same level of performance as the eTDS headset in terms of the maze-navigation task. However, its performance in the center-out tapping task is inferior to that of the eTDS headset.
Our hypothesis that the iTDS has improved robustness over the eTDS was supported by our experimental results. The iTDS retainer was secured on the roof of the mouth by tightly clasping onto the upper teeth, helping the magnetic sensors maintain their positions with respect to the tongue despite inertial and mechanical forces. Another benefit of the iTDS retainer is that it can be completely hidden inside the mouth and eliminate the concern of being a sign of disability. Additionally, the size of the magnetic tracer used for the iTDS is much smaller than the eTDS because of its proximity to the magnetic sensors. This would help shrinking the size of the tongue ring, and increase the possibility of using a tongue implant. A downside of the iTDS over eTDS is occupying a space in the users’ oral space and limiting their tongue movements. This would require further reduction in the overall volume of the future iTDS revisions.
Considering the benefits and limitations of the iTDS over the eTDS, the authors consider it a better option as a primary AT for daily activities. Nonetheless, clinical trials and real life user experiences are needed before a solid conclusion can be reached. In the meantime we are going to improve the performance of both versions of this new AT.
Acknowledgments
This work was supported in part by the National Institute of Biomedical Imaging and Bioengineering grant 1RC1EB010915 and the National Science Foundation award CBET-0828882 and IIS-0803184.
Footnotes
34th Annual International Conference of the IEEE EMBS San Diego, California USA, 28 August - 1 September, 2012
References
- 1.Huo X, Wang J, Ghovanloo M. A magneto-inductive sensor based wireless tongue-computer interface. IEEE Trans Neural Syst Rehab Eng. 2008 Oct;16(5):497–504. doi: 10.1109/TNSRE.2008.2003375. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Huo X, Ghovanloo M. Evaluation of a wireless wearable tongue computer interface by individuals with high level spinal cord injuries. J Neural Eng. Mar 2010;7(2):026008. doi: 10.1088/1741-2560/7/2/026008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Kim J, Huo X, Minocha J, Holbrook J, Laumann A, Ghovanloo M. Evaluation of a smartphone platform as a wireless interface between tongue drive system and electric-powered wheelchairs. IEEE Trans Biomed Eng. 2012 Jun;59(6):1787–1796. doi: 10.1109/TBME.2012.2194713. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Adaptive Switch Labs. [Online]. Available: http://www.asl-inc.com/
- 5.Nuance Communications, Inc. [Online]. Available: http://www.nuance.com/dragon/index.htm.
- 6.Park H, Kim J, Hwang I, Huo X, Ghovanloo M. New ergonomic headset for tongue drive system with wireless smartphone interface. Proc IEEE Eng inMed Biol Conf (EMBC’ll) 2011 Sep;:7344–7347. doi: 10.1109/IEMBS.2011.6091713. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Park H, Gosselin B, Kiani M, Lee H, Kim J, Huo X, Ghovanloo M. A wireless magnetoresistive sensing system for an intra- oral tongue-computer interface. IEEE ISSCC Dig Tech Papers. 2012 Feb;:124–125. doi: 10.1109/TBCAS.2012.2227962. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Yousefi B, Huo X, Veledar E, Ghovanloo M. Quantitative and comparative assessment of learning in a tongue-operated computer input device. IEEE Trans Info Tech in Biomedicine. 2011 Sep;15(5):747–757. doi: 10.1109/TITB.2011.2158608. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Yousefi B, Huo X, Kim J, Veledar E, Ghovanloo M. Quantitative and comparative assessment of learning in a tongue-operated computer input device - Part II: Navigation tasks. IEEE Trans Info Tech in Biomedicine. doi: 10.1109/TITB.2012.2191793. To appear in. [DOI] [PMC free article] [PubMed] [Google Scholar]