

Abstract
Gossypiboma is a term used to describe a foreign mass within the body that is composed of a cotton matrix. Gossypiboma can cause infection or abscess formation from an early stage, or it can remain clinically silent for many years. Gossypiboma can be diagnosed using several methods including abdominal X-ray films, US of the abdomen, contrast-enhanced computed tomography of the abdomen, and during surgery. However, the variable appearance of gossypiboma can lead to diagnostic misinterpretations. Here, we report a successful diagnosis of gossypiboma using a novel method, that is, endoscopic ultrasound-fine-needle aspiration.
Keywords: A forward-view, endoscopic ultrasound-fine-needle aspiration, gossypiboma
INTRODUCTION
Gossypiboma (retained surgical sponge) describes a mass of cotton or sponge that is left behind in the body cavity during a surgical operation. These foreign bodies can often mimic tumors or abscesses when detected clinically or with radiation. In fact, surgical sponges without opaque markers are the leading cause for the difficulty of a correct diagnosis.[1,2] Here, we present a case in which a foreign body, gauze without radiopaque markers, was left behind during a procedure that involved the removal of an intrapelvic tumor. After a computed tomography (CT) scan had revealed information leading to an inaccurate diagnosis, an accurate diagnosis of gossypiboma was successfully made using endoscopic ultrasound-fine-needle aspiration (EUS-FNA).
CASE REPORT
A 60-year-old female patient was referred with an unexpected detection of an intrapelvic tumor during a routine CT scan. The patient's medical history included a hysterectomy and a left side ovariectomy at the age of 27. The CT scan revealed a 45 mm tumor in the patient's pelvis [Figure 1a and b], which was diagnosed as a gastrointestinal stromal tumor (GIST), a chronic expanding hematoma or leiomyoma. A forward-view EUS (TGF-UC260J, Olympus Optical Co., Tokyo, Japan) identified a low echoic lesion when scanned from the sigmoid colon. FNA was performed with a 22-gauge needle (EZShot2, Olympus Optical Co., Tokyo, Japan) by using the forward-view EUS [Figure 2]. Examination of the FNA specimen revealed a foreign body (string of gauze) displaying macrophage cells and necrotic tissue [Figure 3; hematoxylin and eosin, original magnification ×40]. During the surgery, the foreign body composed of gauze was located and removed. The site was deemed clean as no remaining foreign bodies were detected. The site was free of infection and without abscess. Histological examination of the tissue adjacent to the foreign body revealed granuloma formations with fragmented silken threads [Figure 4; hematoxylin and eosin, original magnification, ×100 and ×200].
Figure 1.

Intrapelvic tumor. a: Sagittal section (black arrow); b: Horizontal section (black arrow).
Figure 2.
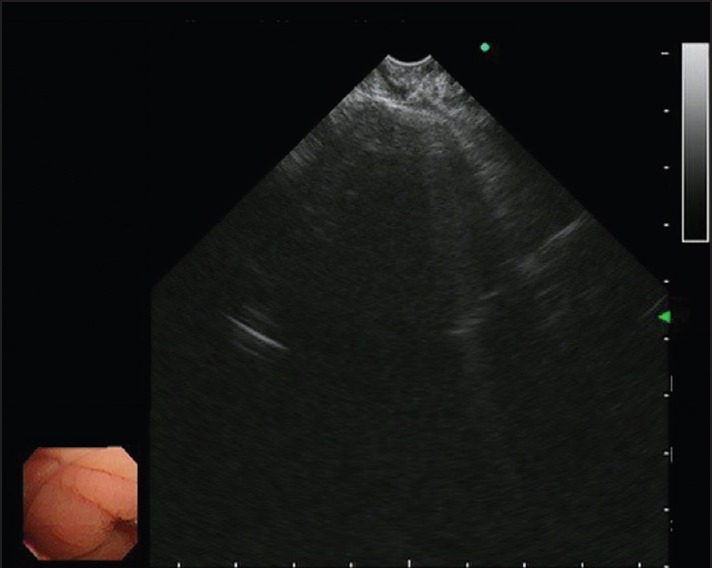
Endoscopic ultrasound (EUS)-fine-needle aspiration using forward-view EUS
Figure 3.
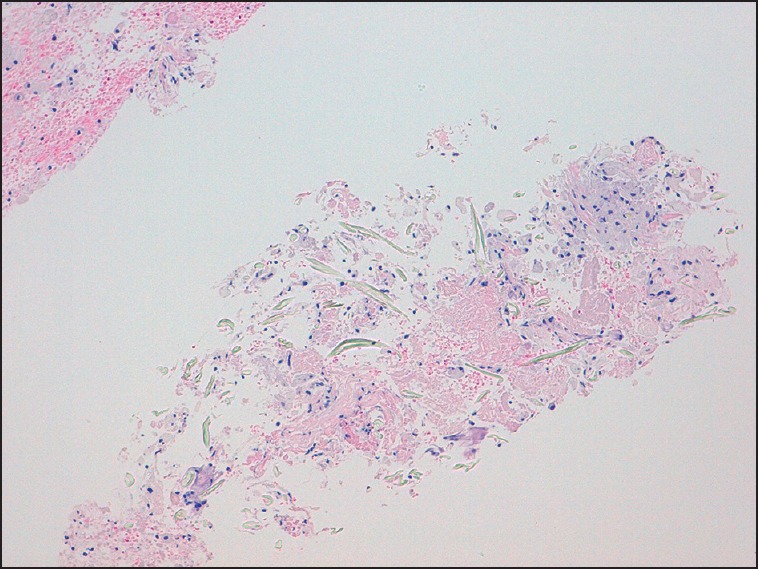
A foreign body (string of gauze) obtained using the 22-gauge needle, with macrophage cells and necrotic tissue
Figure 4.
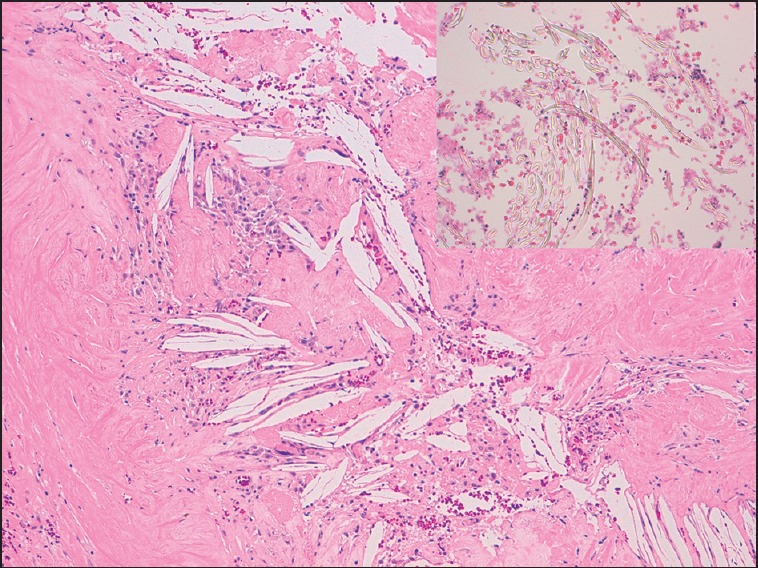
Granuloma formations with fragmented silken threads
DISCUSSION
Gossypiboma describes a mass of cotton or a sponge that is retained in the body after a surgery. Gossypiboma causes foreign body reactions of the surrounding tissue since they are inert and show no specific decomposition.[3] In this case, radiopaque sponges were not used, and there were no adverse symptoms in the 30 years postsurgery. The typical appearance of gossypiboma shows a spongiform pattern with gas bubbles.[1] In typical cases, CT scan is very accurate in diagnosing and localizing abdominal gossypiboma. However, it can be difficult to diagnose the disorder with CT scans in cases without gas bubbles. In the case described in this paper, radiologists using findings from a CT scan, initially and incorrectly diagnosed the lesion as GIST with fibrosis. However, the disorder was correctly diagnosed by a team of gastroenterologists using EUS-FNA. The EUS-FNA procedure revealed a segment of string in a fixed foreign body in the pelvis. We currently believe there are no case reports diagnosing gossypiboma by EUS-FNA. The application of EUS using curved linear array (CLA) endoscopes in the lower GI tract has been limited to the rectum and distal sigmoid colon because of the oblique-viewing optics.[4] There were case reports using oblique-viewing CLA echoendoscopes to evaluate lesions proximal to the sigmoid colon, but advancement of the CLA echoendoscope beyond the sigmoid required the use of an overtube or a guide wire previously placed with a colonoscope.[5,6] Dr. Binmoeller et al. have reported the feasibility and safety of the front-view forward-array echoendoscope for evaluating right colon lesions.[7] Thus, we used a front-view forward-array echoendoscope to safely evaluate the intrapelvic tumor and sample the tissue. A correct diagnosis was obtained using this method. In summary, this is the first known case report diagnosing gossypiboma by EUS-FNA.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Kopka L, Fischer U, Gross AJ, et al. CT of retained surgical sponges (textilomas): Pitfalls in detection and evaluation. J Comput Assist Tomogr. 1996;20:919–23. doi: 10.1097/00004728-199611000-00009. [DOI] [PubMed] [Google Scholar]
- 2.Choi BI, Kim SH, Yu ES, et al. Retained surgical sponge: Diagnosis with CT and sonography. AJR Am J Roentgenol. 1988;150:1047–50. doi: 10.2214/ajr.150.5.1047. [DOI] [PubMed] [Google Scholar]
- 3.Williams RG, Bragg DG, Nelson JA. Gossypiboma – The problem of the retained surgical sponge. Radiology. 1978;129:323–6. doi: 10.1148/129.2.323. [DOI] [PubMed] [Google Scholar]
- 4.Bhutani MS, Nadella P. Utility of an upper echoendoscope for endoscopic ultrasonography of malignant and benign conditions of the sigmoid/left colon and the rectum. Am J Gastroenterol. 2001;96:3318–22. doi: 10.1111/j.1572-0241.2001.05332.x. [DOI] [PubMed] [Google Scholar]
- 5.Fehring A, Schmulewitz N. EUS-guided FNA diagnosis of recurrent follicular lymphoma in the transverse colon. Gastrointest Endosc. 2006;64:652–3. doi: 10.1016/j.gie.2006.02.033. [DOI] [PubMed] [Google Scholar]
- 6.Sasaki Y, Niwa Y, Hirooka Y, et al. The use of endoscopic ultrasound-guided fine-needle aspiration for investigation of submucosal and extrinsic masses of the colon and rectum. Endoscopy. 2005;37:154–60. doi: 10.1055/s-2004-826152. [DOI] [PubMed] [Google Scholar]
- 7.Nguyen-Tang T, Shah JN, Sanchez-Yague A, et al. Use of the front-view forward-array echoendoscope to evaluate right colonic subepithelial lesions. Gastrointest Endosc. 2010;72:606–10. doi: 10.1016/j.gie.2010.03.1126. [DOI] [PubMed] [Google Scholar]