

Abstract
Dystonia can be focal, segmental, multifocal, generalized, or hemidystonia. Focal dystonia is localized to a specific part of the body. Overall upper limb is more commonly involved in focal dystonia than lower limb and since it starts from hand, focal hand dystonia (FHD) is a more accepted terminology. Writer's cramp and musician dystonia are commonest types of FHD. Typically this dystonia is task specific, but in some patients this specificity may be lost over a period of time. Segmental or generalized dystonia may also start as FHD, so a detailed clinical assessment is required, which should be supplemented by relevant investigations. Treatment includes oral medications, injection botulinum toxin, neurosurgery including neurostimulation, and rehabilitation. Role of injection botulinum toxin has been extensively studied in writer's cramp patients and found to be effective; however, selection of muscles and techniques of injection are crucial in getting best results.
Keywords: Botulinum toxin, dystonia, writer's cramp
Introduction
Dystonia is a movement disorder characterized by sustained or intermittent muscle contractions causing abnormal, often repetitive, movements, postures, or both.[1] Based on extent of body parts involved, focal hand dystonia (FHD) is a common form of adult onset focal dystonia.[2] They are usually task specific where the hand has been repeatedly used for a particular activity for a long period of time.[3] Task specific dystonia is characterized by patients having difficulty in executing a specific activity with otherwise no other difficulties in using hand. They can virtually arise from any task, can remain task specific or can lose specificity over time. A common type is writer's cramp, while another is musician's dystonia seen in patients using string instruments or piano.[4] Other forms include telegraphist's cramp, golfer's yips, and relatively uncommonin hairdressers, surgeons, tailors, and cobblers.[5]
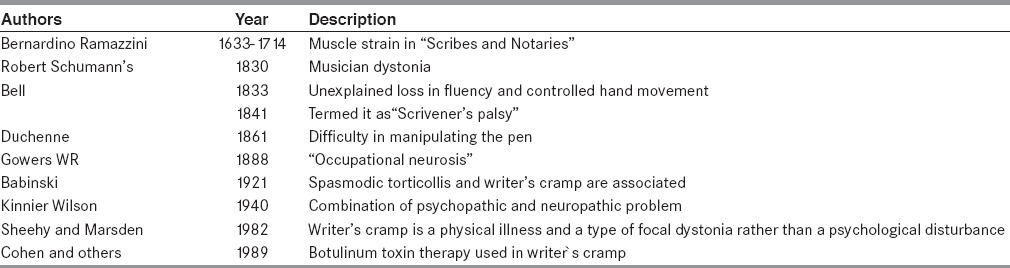
History: Earliest description of FHD was discussed by Bernardino Ramazzini as muscle strain in “Scribes and Notaries” [Table 1].[6,7,8,9,10,11,12,13,14] Kinner Wilson in 1940 opined that the pathogenesis of FHD is a combination of underlying psychiatric state of the patient and peripheral neuropathy.[12] In 1982, Sheehy and Marsden coined the term as writer's cramp and gave a detailed description of the condition highlighting that this is a physical illness and a type of focal dystonia.[13]
Table 1.
Important milestones in the pathogenesis of focal hand dystonia
Pathophysiology
FHD pathogenesis includes a putative mechanisms including loss of inhibition, sensorimotor abnormalities, and maladaptive plasticity.[15]
Loss of inhibition
Any particular movement in our body requires a balance between activation of the agonist muscles that are responsible for that movement and simultaneous inhibition of the antagonist muscles that inhibit the movement. This loss of balance has been found at various levels of the nervous system in these patients. Patients of FHD have been found to have a loss of reciprocal inhibition at the level of spinal cord causing co-contraction of antagonist muscles along with the agonist muscles.[16] Techniques such as transcranial magnetic stimulation has found abnormal intracortical inhibition in patients with FHD.[17] Surround inhibition has also been found to be abnormal in such patients.[15] Inhibitory interneurons that use gamma-aminobutyric acid have been found to be deficient in such patients.[18] Abnormal motor programming has been found in patients with FHD.[19,20] Interestingly, studies have found defective intracortical inhibition only during movement, but not at rest.[21]
Sensory abnormalities
FHD patients have been found to have an enlarged and disorganized somatosensory receptive field.[22,23] Sensory retraining in the form of tactile discrimination has been found to reduce the motor symptoms.[24] The role sensory modulation is further strengthened by the fact that some patients use sensory trick in which their symptoms are improved on touching or holding the affected hand by the contralateral hand.[15]
Maladaptive plasticity
Homeostatic plasticity allows the nervous system to adapt to the dynamic external environment and facilitates learning and memory. This mechanism has been found to be abnormal in patients of FHD.[25,26] Neuronal plasticity has been found to be abnormally increased in such patients which could further explain that repetitive movement ofa hand can lead to alteration in the sensorimotor maps in the cortex, eventually leading to the development of dystonia.
Clinical Evaluation of FHD Patients
Detailed history taking and physical examination is important in the diagnosis and management of FHD patients. Secondary dystonias due to antidopaminergic drugs, metabolic disorders such as Wilson's disease, and neurodegenerative disorders like dopa responsive dystonia should be ruled out. It is important to remember that many primary generalized dystonias such as DYT1 may start as FHD. Treatment and prognosis of all these disorders will be different than FHD.
Treatment
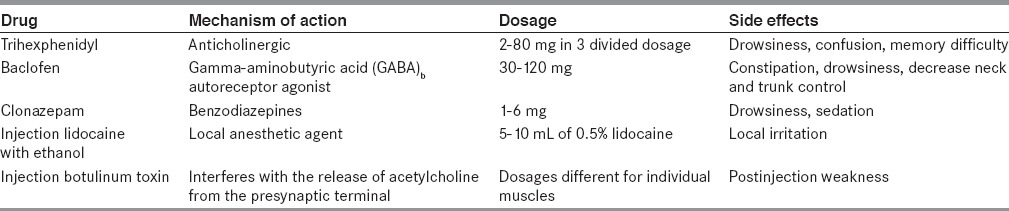
Oral medications including anticholinergic drugs and benzodiazepine, botulinum toxin injection, brain surgery, and experimental treatments such as limb immobilization are used for the treatment of FHD [Table 2]. Brain surgery includes lesionectomy and more recently deep brain stimulation of ventralis oralis (Vo) nucleus of thalamus. Limb immobilization using a plastic splint, motor training by asking the patient to write using individual fingers, and sensory training by reading and practicing Braille have been used.
Table 2.
Different pharmacological treatment used in focal hand dystonia patients
Botulinum Toxin in FHD
Botulinum toxin is the main modality of treatment in patients of FHD. Different types of botulinum toxins are available [Table 3]. Most of the therapeutic trials on FHD have been with botulinum toxin type A (BONT-A). Botulinum toxin is given intramuscular and acts at the neuromuscular junction by inhibiting the release of acetylcholine. It gets internalized in the presynaptic axon where it cleaves SNARE (soluble NSF attachment protein receptor) protein, resulting in inhibition of acetylcholine exocytosis.[27] Botulinum toxin has also been thought to have central effects. Studies in animal models show that botulinum toxin undergoes retrograde and transynaptic transport to affect the spinal cord and brain.[28,29] Many studies have been conducted to assess the efficacy of botulinum toxin in FHD, with the majority of studies being focused on writer's cramp and musician's dystonia [Table 4].
Table 3.
Types of botulinum toxin used in focal hand dystonia patients
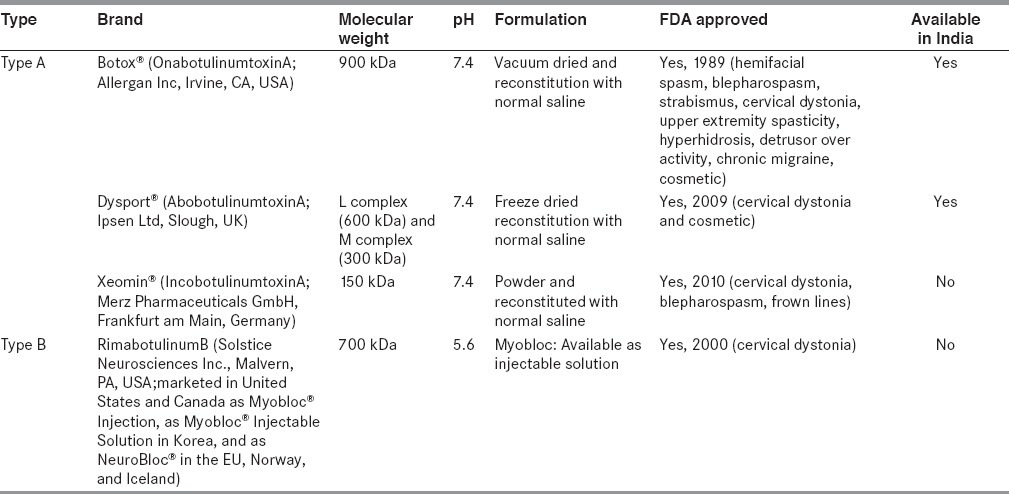
Table 4.
Studies of botulinum toxin in focal hand dystonia
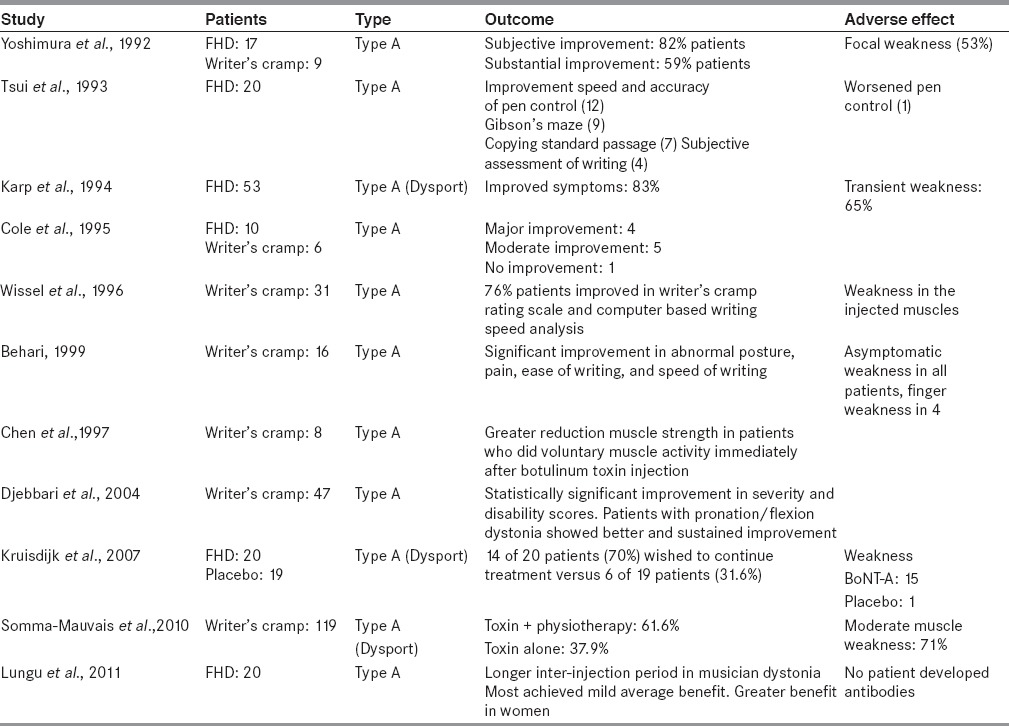
Yoshimura et al., in their study of 17 FHD patients found subjective and substantial improvement in 82 and 59% of their patients, respectively.[30] Fifty-three percent of the patients developed focal weakness after injection. Similarly, Tsui et al., in their study of 20 patients of writer's cramp found improvement in terms of speed and accuracy in pen holding, Gibson's maze, and subjective assessment of writing.[31] Cole et al., in their double blind study compared the efficacy of botulinum toxin with that of placebo in terms of subjective rating, objective testing, and physician's rating.[32] Out of 10 patients studied, eight showed improvement in subjective rating that was later confirmed by at least one objective test in six of those patients. Two patients showed no improvement to botulinum toxin. In a study of 31 patients with writer's cramp, Wissel et al., assessed the response to botulinum toxin in terms of writer's cramp rating scale and computer-based writing speed analysis.[33] With a mean injection dosage of 133.2 units per session, up to 76% of the patients showed improvement at 1 year, while weakness was found to be the most common side effect (72% of the follow-up visits). Behari in a study of 16 patients of writer's cramp found significant improvement in terms of ease of writing, abnormal posture and pain.[34] The mean duration of effect was found to be 9.47 weeks. Four patients developed symptomatic finger weakness. Djebbari et al., in their study of 47 patients with writer's cramp found significant improvement in both severity and disability scores.[35] They also found a better response inpatients with pronation/flexion type of dystonias. A randomized, double blind study by Kruisdijk et al., in 40 patients receiving botulinum A toxin found improvement in clinical scales of impairment and disability.[36] Somma-Mauvais et al., in their study of 119 patients found botulinum toxin to be effective in patients of writer's cramp with greater effects when it was combined with physiotherapy as compared to when given in isolation.[37] Lungu et al., followed 20 patients of FHD treated with botulinum toxin and found it to be an effective modality of treatment.[38] Greater response was found in patients with musician's dystonia and in female patients. No antibody against botulinum toxin was found in the long-term follow-up. No serious side effect was observed. Karp et al., in their study of 53 patients of FHD who had received botulinum toxin for atleast once, found improvement in the symptoms.[39] They traced their patients to a follow-up of up to 6 years and found this treatment to be a safe and effective modality.
To summarize the above studies, botulinum toxin is an effective and safe therapeutic modality in patients with FHD and, besides focal weakness and pain, it is not associated with serious side effects. Long-term studies have also found no adverse effects of its use and the possibility of antibody formation against botulinum toxin in the longer run is remote.
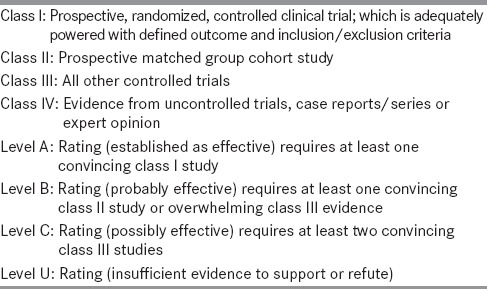
The drawbacks however include its short duration of beneficial action and the cost. The American Academy of Neurology in their guidelines find botulinum toxin to be probably effective in treatment of FHD and recommend it should be considered in such patients [Tables 5 and 6].[40] Botulinum toxin might still not have clear cut evidence to be unequivocally effective in this group of patients, however with the lack of other effective treatment modalities it remains the mainstay of therapy in patients with FHD.
Table 5.
Recommendations for using botulinum toxin in focal upper limb dystonia
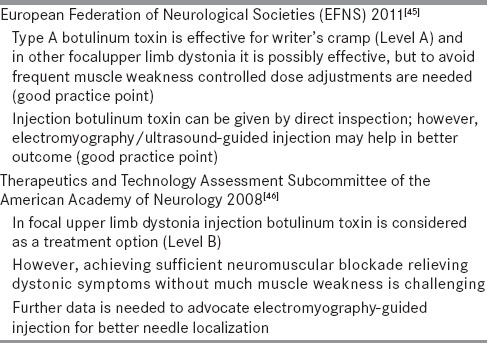
Table 6.
Clinical evaluation and muscle selection for botulinum toxin injection in writer's cramp [Table 7]
Table 7.
Checklist before injecting
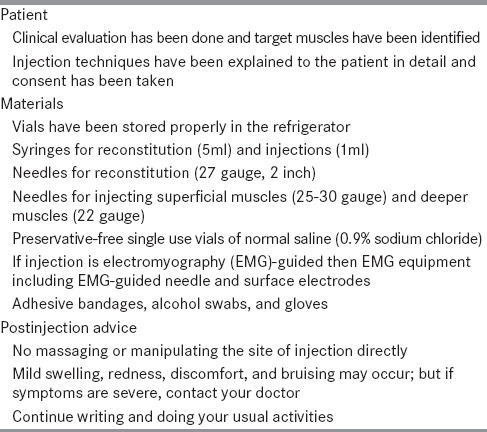
Muscle selection for botulinum toxin injection in writer's cramp is decided on clinical grounds, based on the muscle responsible for causing the postural deviations. Assessment should be done to classify whether the writer's cramp is simple or complex (more than one task involved), local (3 fingers involved) or generalized (more than 3 fingers involved), muscles effected (flexor, extensor, or combination), and any other associated dystonias present. A study found that the muscles most commonly injected in writer's cramp patients includeflexor carpi ulnaris, flexor digitorum superficialis (FDS), extensor carpi radialis, and flexor pollicis longus (FPL).[33] Responsible muscles can also be selected by identifying co-contraction bursts on surface electromyography(EMG) [Figure 1]. The most important step is to find out the muscle showing severe spasm and differentiate the dystonic movement and compensatory movement. Eliciting mirror dystonia by asking the patient to write using the contralateral hand and allowing the dystonic hand to relax is helpful in approximately 50% patients. In difficult situations, EMG-guided injection is useful in identifying muscles and guiding the injection. In a study only 37% of needle placement attempt reached the target muscles or muscle fascicles without EMG guidance, demonstrating the importance of EMG guidance.[41] Ultrasonography is emerging as an important tool in correct identification and localization of muscles in FHD patients. Writer's cramp rating scale has been extensively used for detailed clinical assessment and follow-up.[27] Patients should be encouraged to exercise after the injections as it will improve the efficacy and symptom reduction.
Figure 1.
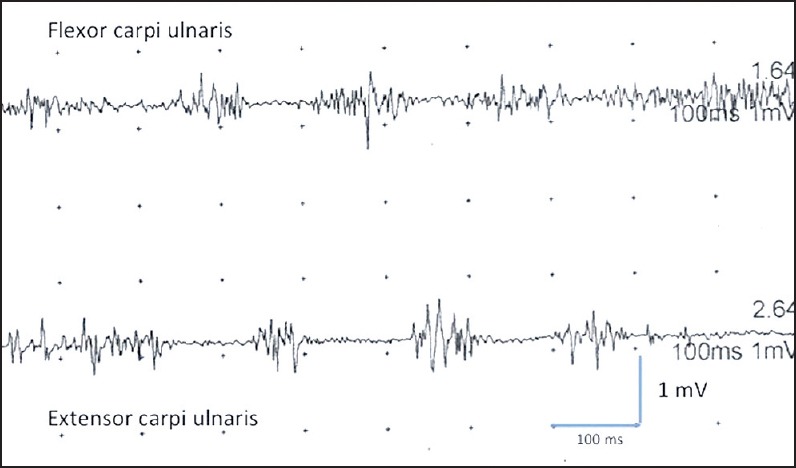
Surface electromyography is showing task related (during writing) 4-5 Hz irregular or jerky rhythmictremor secondary to co-contraction of agonist (flexor carpi ulnaris) and antagonist (extensor carpi ulnaris) muscles
Depending upon the muscle involvement, writer's cramp has been broadly classified as flexor and extensor type.
Flexor type
In flexor type finger, thumb and wrist flexors may be involved in isolation or combination [Figure 2a]. Overall long-term prognosis of this type of writer's cramp is found to be good.
Figure 2.

(a) Flexor type and (b) Extensor typeof writer's cramp. (c) Weakness in right extensor digitorum muscle 7 days after botulinum toxin injection as patient is not able to fully extend his right fingers at metacarpophalangeal and interphalengeal joints (extension in left fingers is normal)
FDS [Figure 3a]
Figure 3.
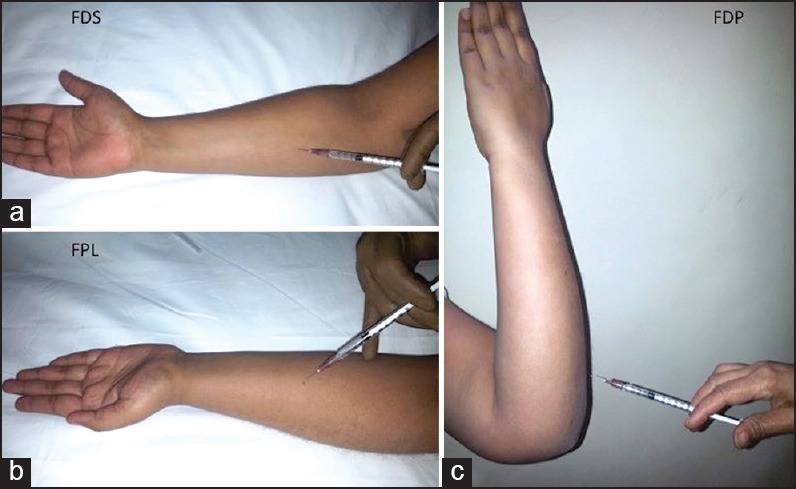
((a) Injection technique for flexor digitorum superficialis (FDS). (b) Injection technique for flexor pollicis longus (FPL). (c) Injection technique for flexor digitorum profundus (FDP)
FDS flexes the interphalangeal and metacarpophalangeal joints II-V. Injection is best given in the midfoream on the ulnar side and each fascicle can be identified using the respective movement. During the injection, elbow should be supinated while wrist and fingers should be extended.
Usual dosages: Botox (25-50 U), Dysport(75-150 U)
Needle depth: 10-20 mm
FPL [Figure 3b]
Thumb flexion at interphalangeal joint is done by FPL muscle. Patient is injected in the middle of the forearm with direction of needle towards the radius.
Usual dosages: Botox (5-20 U), Dysport (20-50 U)
Needle depth: 10-20 mm
Flexor digitorum profundus (FDP) [Figure 3C]
FDP is the only flexor of the distal interphalangeal joint. We can approach through the flexor (this way muscles is too deep) or extensor (superficial and relatively easy) aspect of the forearm. The muscle is best injected when the hand is supinated, elbow is flexed, and needle is inserted 2-3 cm above the olecranon process. Individual injection should be targeted for digit II-V using finger movements.
Usual dosages: Botox (20-60 U), Dysport (60-120 U)
Needle depth: 10-20 mm
Flexor carpi radialis (FCR) [Figure 4a]
Figure 4.
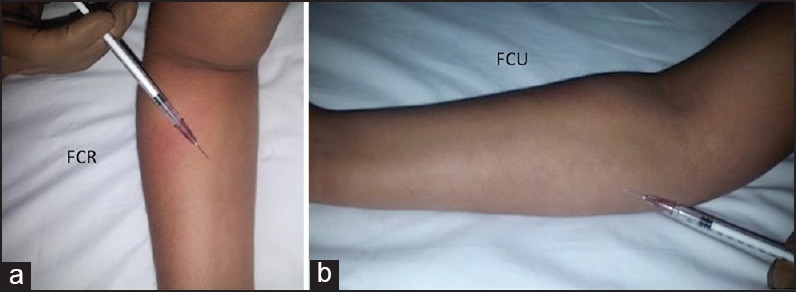
(a) Injection technique for flexor carpi radialis (FCR). (b) Injection technique for flexor carpi ulnaris (FCU)
FCR flexes the wrist and abducts the hand. The muscle is best localized while elbow is mid flexed, supinated and wrist is abducted. The needle is inserted at one-third distance from medial epicondyle.
Usual dosages: Botox (20-50 U), Dysport (60-120 U)
Needle depth: 20-30 mm
Flexor carpi ulnaris (FCU) [Figure 4b]
FCU flexes the wrist and does the adduction leading to ulnar deviation. Injection is done between the proximal third of the line joining the medial epicondyle and styloid process of the ulna.
Usual dosages: Botox (15-60 U), Dysport (50-120 U)
Needle depth: 20-30 mm
Extensor type: Finger, wrist extensor, or individual extensor muscles of thumb and index fingers may be involved [Figure 2B].
Extensor digitorum communis (EDC) [Figure 5a]
Figure 5.

(a) Injection technique for extensor digitorum communis (EDC). (b) Injection technique for extensor pollicis longus (EPL). (c) Injection technique for extensor indicis (EI)
EDC extends the wrist and all finger joints. Muscle is best localized between the first and second thirds in the middle of the muscles at line joining the lateral epicondyle and ulnar styloid.
Usual dosages: Botox (10-25 U), Dysport (30-70 U)
Needle depth: 10-15 mm
Extensor pollicis longus (EPL) [Figure 5b]
EPL extends the thumb and abducts it. This muscle lies beneath the other extensors and best localized while the arm is pronated. The injection site is middle third of the forearm between radius and ulna.
Usual dosages: Botox (5-20 U), Dysport (15-60 U)
Needle depth: 10-20 mm
Extensor indicis (EI) [Figure 5c]
EI extends the index finger only. Best position to inject is while arm is pronated while wrist and fingers are extended. Muscle is localized approximately 4 cm proximal to the ulnar styloid process.
Usual dosages: Botox (5-10 U), Dysport (15-40 U)
Needle depth: <10 mm
Extensor carpi radialis longus (ECRL) [Figure 6a]
Figure 6.
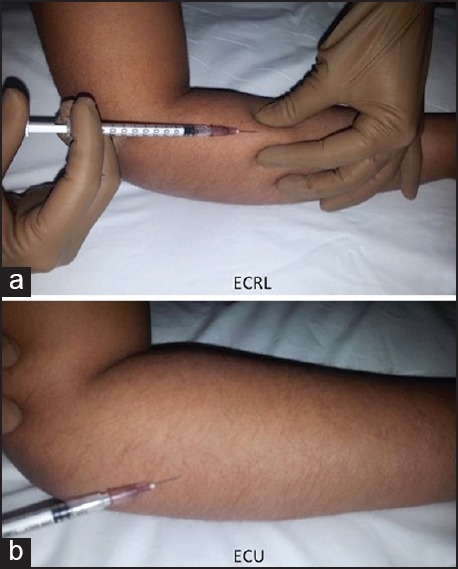
(a) Injection technique for extensor carpi radialis longus (ECRL). (b) Injection technique for Extensor carpi ulnaris (ECU)
ECRL extend the wrist and abduct the hand. Extensor carpi radialis brevis works with ECRL. During injection both muscles are difficult to differentiate and best injected, while elbow is flexed and pronated. Muscle is localized approximately 2-3 cm distal to elbow joint.
Usual dosages: Botox (5-20 U), Dysport (15-60 U)
Needle depth: 10-20 mm
Extensor carpi ulnaris (ECU) [Figure 6b]
ECUextend the wrist and adducts the hand. The muscle is best localaized while elbow is flexed and hand is pronated. Injection is given above the osseous edge in the middle of ulna.
Usual dosages: Botox (5-20 U), Dysport (15-60 U)
Needle depth: 10-20 mm
Long-term efficacy and safety of botulinum toxin injection
In majority of the FHD patients, long-term efficacy, safety, and postinjection weakness with botulinum toxin is an important issue [Figure 2c]. In a recent study, 20 patients who received injection botulinum toxin for FHD continued treatment for 10 years or more.[38] Five had musician's dystonia (two piano, one guitar, one drums, and one trumpet), nine had writer's cramp, five were having mixed dystonia, and one was typist. Most patients (11/20) experienced mild average benefit and only mild weakness was present in patients (9/20); however, there was no correlation between weakness and benefit. There were no serious adverse effects, no patient discontinued due to discomfort, and none developed immunity over the long duration of follow-up. In another study there was good efficacy and tolerance for this treatment in the long-term. In 46% patients, there was recovery of normal writing, partial benefit was in 10%, no benefit in 21%, and in 23% patients there was loss to follow-up. Authors concluded that good effect lasted for average 6 months. Progressive writer's cramp, long duration, associated tremor, and secondary dystonia were poor prognostic markers; however, there was no prognostic value of mirror dystonia in this study.[42] Most common reason of stoppage of botulinum toxin treatment in FHD is the insufficient benefit. In comparison to cervical dystonia (80%) and blepharospasm (90%), overall response rate in FHD is low (about 50%).[43] In a 1 year follow-up; double-blind randomized, placebo-controlled trial in 40 patients who received either BoNT-A (dysport) or placebo injections in two sessions and 20 patients who received the BoNT-A injection chose to continue the treatment due to beneficial effects in comparison with 6 of 19 patients in placebo group.[36]
Musician and other FHDs
The highly demanding professional skill and ultimate goal of returning to playing musical instrument to perfection makes musician dystonia a difficult and challenging condition to treat. Medical therapies including baclofen, benzodiazepines, anticholinergics, and phenytoin [Table 2] have been used with disappointing results. Injection botulinum toxin is better tolerated and effective, but postinjection weakness in a major limiting factor leading to poor acceptability in the long term. Dosages needs to be kept at the minimum and selection of muscles should be precized. Uses of EMG and USG-guided injections are very helpful in musician dystonia patients. Outcome is best when primary dystonic muscles are injected rather than compensatory muscles similar to other FHD patients. Occupational therapy, rehabilitation, and immobilization techniques have also been used with limited success.
Golfer's “yipps” usually manifests while putting the golfstick and gets exacerbated by anxiety.[44] Injection botulinum toxin has been used in this condition, but there is no systemic study. Similarly typist and telegraphers may also complain of pain, cramp, and abnormal posturing of hand. A combination of anticholinergic drugs and injection botulinum toxin may be effective course of treatment.
Conclusion
Similar to other types of dystonias, treatment for FHD is only symptomatic rather than curative or protective. Treatment selection should be based on type and distribution of muscle involvement, age, and severity of symptoms. Injection botulinum toxin is the mainstay of treatment. Dosage should be calibrated for the individual patient depending upon the dystonic activity of muscles. Mirror dystonia is helpful in identifying the target muscles. Use of EMG and ultrasound are helpful in guided injections of deeper muscles. Addressing comorbidities and educating family members is equally important [Table 6].[46]
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Albanese A, Bhatia K, Bressman SB, Delong MR, Fahn S, Fung VS, et al. Phenomenology and classification of dystonia: A Consensus Update. Mov Disord. 2013;15(28):863–73. doi: 10.1002/mds.25475. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Jinnah HA, Berardelli A, Comella C, Defazio G, Delong MR, Factor S. Current views and challenges for future research. Mov Disord. 2013;28:926–43. doi: 10.1002/mds.25567. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Torres-Russotto D, Perlmutter JS. Task-specific dystonias: A review. Ann N Y Acad Sci. 2008;1142:179–99. doi: 10.1196/annals.1444.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Altenmuller E, Baur V, Hofmann A, Lim VK, Jabusch HC. Musician's cramp as manifestation of maladaptive brain plasticity: Arguments from instrumental differences. Ann N Y Acad Sci. 2012;1252:259–65. doi: 10.1111/j.1749-6632.2012.06456.x. [DOI] [PubMed] [Google Scholar]
- 5.Giorelli M, Zimatore GB. Hairdresser's dystonia: An unusual occupational dystonia. Tremor Other Hyperkinet Mov (N Y) 2013;4:3. doi: 10.7916/D87S7MGH. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Franco G, Fusetti L. Bernardino Ramazzini's early observations of the link between musculoskeletal disorders and ergonomic factors. Appl Ergon. 2004;35:67–70. doi: 10.1016/j.apergo.2003.08.001. [DOI] [PubMed] [Google Scholar]
- 7.Chang FC, Frucht SJ. Motor and sensory dysfunction in Musician's dystonia. Curr Neuropharmacol. 2013;11:41–7. doi: 10.2174/157015913804999531. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Bell C. London: Taylor and Francis; 1833. The Nervous System of the Human Body. [Google Scholar]
- 9.Gowers WR. Vol. 2. London: Churchill; 1888. A manual of diseases of the nervous system; pp. 656–74. [Google Scholar]
- 10.Duchenne de Boulogne GB. L’Electrisation localisee. Vol. 1. Paris: Bailliere; 1861. Spasme fonctionel et paralysies musclaires fonctionelles; pp. 928–46. [Google Scholar]
- 11.Babinski J. Spasme facial post encephalitique. Revue Neurologique. 1921;28:462–8. [Google Scholar]
- 12.Wilson SA. Vol. 2. London: Butterworth; 1940. Neurology; pp. 1675–84. [Google Scholar]
- 13.Sheehy MP, Marsden CD. Writers’ cramp-a focal dystonia. Brain. 1982;105:461–80. doi: 10.1093/brain/105.3.461. [DOI] [PubMed] [Google Scholar]
- 14.Cohen LG, Hallett M, Geller BD, Hochberg F. Treatment of focal dystonias of the hand with botulinum toxin injections. J Neurol Neurosurg Psychiatry. 1989;52:355–63. doi: 10.1136/jnnp.52.3.355. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Lin PT, Hallett M. The pathophysiology of focal hand dystonia. J Hand Ther. 2009;22:109–14. doi: 10.1016/j.jht.2008.10.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Nakashima K, Rothwell JC, Day BL, Thompson PD, Shannon K, Marsden CD. Reciprocal inhibition between forearm muscles in patients with writer's cramp and other occupational cramps, symptomatic hemidystonia and hemiparesis due to stroke. Brain. 1989;113:681–97. doi: 10.1093/brain/112.3.681. [DOI] [PubMed] [Google Scholar]
- 17.Chen R, Wassermann E, Canos M, Hallett M. Impaired inhibition in writer's cramp during voluntary muscle activation. Neurology. 1997;49:1054–9. doi: 10.1212/wnl.49.4.1054. [DOI] [PubMed] [Google Scholar]
- 18.Levy LM, Hallett M. Impaired brain GABA in focal dystonia. Ann Neurol. 2002;51:93–101. [PubMed] [Google Scholar]
- 19.Hamano T, Kaji R, Katayama M, Kubori T, Ikeda A, Shibasaki H, et al. Abnormal contingent negative variation in writer's cramp. Clin Neurophysiol. 1999;1130:508–15. doi: 10.1016/s1388-2457(98)00045-5. [DOI] [PubMed] [Google Scholar]
- 20.Toro C, Deuschl G, Hallett M. Movement-related electroencephalographic desynchronization in patients with hand cramps: Evidence for motor cortical involvement in focal dystonia. Ann Neurol. 2001;47:456–61. [PubMed] [Google Scholar]
- 21.Stinear CM, Byblow WD. Impaired modulation of intracortical inhibition in focal hand dystonia. Cerebral Cortex. 2004;14:555–61. doi: 10.1093/cercor/bhh017. [DOI] [PubMed] [Google Scholar]
- 22.Meunier S, Garnero L, Ducorps A, Mazières L, Lehéricy S, du Montcel ST, et al. Human brain mapping in dystonia reveals both endophenotypic traits and adaptive reorganization. Ann Neurol. 2001;50:521–7. doi: 10.1002/ana.1234. [DOI] [PubMed] [Google Scholar]
- 23.Bara-Jimenez W, Catalan MJ, Hallett M, Gerloff C. Abnormal somatosensory homunculus in dystonia of the hand. Ann Neurol. 1998;44:828–31. doi: 10.1002/ana.410440520. [DOI] [PubMed] [Google Scholar]
- 24.Zeuner KE, Bara-Jimenez W, Noguchi PS, Goldstein SR, Dambrosia JM, Hallett M. Sensory training for patients with focal hand dystonia. Ann Neurol. 2002;51:593–8. doi: 10.1002/ana.10174. [DOI] [PubMed] [Google Scholar]
- 25.Quartarone A, Bagnato S, Rizzo V, Siebner HR, Dattola V, Scalfari A, et al. Abnormal associative plasticity of the human motor cortex in writer's cramp. Brain. 2003;126:2586–96. doi: 10.1093/brain/awg273. [DOI] [PubMed] [Google Scholar]
- 26.Quartarone A, Rizzo V, Bagnato S, Morgante F, Sant’Angelo A, Romano M, et al. Homeostatic-like plasticity of the primary motor hand area is impaired in focal hand dystonia. Brain. 2005;128:1943–50. doi: 10.1093/brain/awh527. [DOI] [PubMed] [Google Scholar]
- 27.Dressler D. Botulinum toxin for treatment of dystonia. Eur J Neurol. 2010;17:88–96. doi: 10.1111/j.1468-1331.2010.03058.x. [DOI] [PubMed] [Google Scholar]
- 28.Lawrence GW, Ovsepian SV, Wang J, Aoki KR, Dolly JO. Extravesicular intraneuronal migration of internalized botulinum neurotoxins without detectable inhibition of distal neurotransmission. Biochem J. 2012;441:443–52. doi: 10.1042/BJ20111117. [DOI] [PubMed] [Google Scholar]
- 29.Matak I, Riederer P, Lackovic Z. Botulinum toxin's axonal transport from periphery to the spinal cord. Neurochem Int. 2012;61:236–9. doi: 10.1016/j.neuint.2012.05.001. [DOI] [PubMed] [Google Scholar]
- 30.Yoshimura DM, Aminoff MJ, Olney RK. Botulinumtoxin therapy for limb dystonias. Neurology. 1992;42:627–30. doi: 10.1212/wnl.42.3.627. [DOI] [PubMed] [Google Scholar]
- 31.Tsui JK, Bhatt M, Calne S, Calne DB. Botulinum toxinin the treatment of writer's cramp: A double-blindstudy. Neurology. 1993;43:183–5. doi: 10.1212/wnl.43.1_part_1.183. [DOI] [PubMed] [Google Scholar]
- 32.Cole R, Hallett M, Cohen LG. Double-blind trial of botulinum toxin for treatment of focal hand dystonia. Mov Disord. 1995;10:466–71. doi: 10.1002/mds.870100411. [DOI] [PubMed] [Google Scholar]
- 33.Wissel J, Kabus C, Wenzel R, Klepsch S, Schwarz U, Nebe A, et al. Botulinum toxinin writer's cramp: Objective response evaluation in 31 patients. J Neurol Neurosurg Psychiatry. 1996;61:172–5. doi: 10.1136/jnnp.61.2.172. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Behari M. Botulinum toxinin the treatment of writer's cramp. J Assoc Physicians India. 1999;47:694–8. [PubMed] [Google Scholar]
- 35.Djebbari R, du Montcel ST, Sangla S, Vidal JS, Gallouedec G, Vidailhet M, et al. Factors predicting improvement in motor disability in writer's cramp treated with botulinum toxin. J Neurol Neurosurg Psychiatry. 2004;75:1688–91. doi: 10.1136/jnnp.2003.032227. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Kruisdijk JJ, Koelman JH, Ongerboer de Visser BW, de Haan RJ, Speelman JD. Botulinum toxin for writer's cramp: A randomised, placebo-controlled trial and 1-year follow-up. J Neurol Neurosurg Psychiatry. 2007;78:264–70. doi: 10.1136/jnnp.2005.083170. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Somma-Mauvais H, Soulayrol S, Duvocelle A, Azulay JP, Gastaut JL. Treating writer's cramp: 14 years’ experience with botulinum toxin. Rev Neurol (Paris) 2010;166:630–8. doi: 10.1016/j.neurol.2009.12.008. [DOI] [PubMed] [Google Scholar]
- 38.Lungu C, Karp BI, Alter K, Zolbrod R, Hallett M. Long term follow-up of botulinum toxin therapy for focal hand dystonia: Outcome at 10 or more years. Mov Disord. 2011;26:750–3. doi: 10.1002/mds.23504. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Karp BI, Cole RA, Cohen LG, Grill S, Lou JS, Hallett M. Long-termbotulinum toxin treatment of focal hand dystonia. Neurology. 1994;44:70–6. doi: 10.1212/wnl.44.1.70. [DOI] [PubMed] [Google Scholar]
- 40.Simpson DM, Blitzer A, Brashear A, Comella C, Dubinsky R, Hallett M, et al. Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Assessment: Botulinum neurotoxin for the treatment of movement disorders (an evidence-based review): Report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Neurology. 2008;70:1699–706. doi: 10.1212/01.wnl.0000311389.26145.95. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Molloy FM, Shill HA, Kaelin-Lang A, Karp BI. Accuracy of muscle localization without EMG: Implications for treatment of limb dystonia. Neurology. 2002;58:805–7. doi: 10.1212/wnl.58.5.805. [DOI] [PubMed] [Google Scholar]
- 42.Marion MH, Afors K, Sheehy MP. Problems of treating writer's cramp with botulinum toxin injections: Results from 10 years of experience. Rev Neurol (Paris) 2003;159:923–7. [PubMed] [Google Scholar]
- 43.Hallett M, Benecke R, Blitzer A, Comella CL. Treatment of focal dystonias with botulinum neurotoxin. Toxicon. 2009;54:628–33. doi: 10.1016/j.toxicon.2008.12.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Turrong D, Dressler M, Hallett M, editors. 1st ed. Cambridge: Cambridge University Press; 2009. Treatment of focal hand dystonia. Manual of botulinum toxin therapy; pp. 61–75. [Google Scholar]
- 45.Albanese A, Asmus F, Bhatia KP, Elia AE, Elibol B, Filippini G, et al. EFNS guidelines on diagnosis and treatment of primary dystonias. Eur J Neurol. 2011;18:5–18. doi: 10.1111/j.1468-1331.2010.03042.x. [DOI] [PubMed] [Google Scholar]
- 46.Simpson DM, Gracies JM, Graham HK, Miyasaki JM, Naumann M, Russman B, et al. Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Assessment: Botulinum neurotoxin for the treatment of spasticity (an evidence-based review): Report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Neurology. 2008;70:1691–8. doi: 10.1212/01.wnl.0000311391.00944.c4. [DOI] [PubMed] [Google Scholar]