

Abstract
Positive emotional engagement develops in the context of face-to-face interactions during the first six months of life. Deficits in emotional engagement are characteristic of autism spectrum disorder (ASD) and may characterize the younger siblings of children with ASD (high-risk siblings). High-risk siblings are likely to exhibit a broad range of positive emotional engagement that may or may not be associated with ASD outcomes. We examined positive emotional engagement (i.e., smiling rate and contingent responsiveness to the partner’s smile) during the infant-parent interaction episodes of the Face-to-Face/Still Face protocol at six months of age. The sample included 43 high-risk infant siblings, 11 of whom went on to an ASD diagnosis, and 25 low-risk siblings with no family history of ASD. Low-risk siblings and high-risk siblings without ASD showed the typical “still-face effect” (i.e., decreases in smiling rate after period of parental non-responsiveness), but high-risk siblings with later ASD outcomes did not show this decrease. Although high-risk siblings without an ASD diagnosis were less likely to respond to their parents’ smiles than low-risk siblings, the children with eventual ASD did not differ from the other groups in contingent responsiveness. Findings suggest that subtle differences in positive emotional engagement are present in the early development of high-risk siblings but are not consistently associated with ASD outcomes.
Keywords: smiling, affective communication, autism risk, infancy
Day-to-day interactions between infants and their parents involve nonverbal responses to one another’s emotional expressions (McQuaid, Bibok, & Carpendale, 2009; Messinger, Ruvolo, Ekas, & Fogel, 2010; Symons & Moran, 1994). Over the first six months of life, infants and mothers may become increasingly responsive to one another’s smiles (Messinger et al., 2010). Deficits in positive emotional responsiveness in early development may be involved in atypical social-emotional outcomes, including symptoms of autism spectrum disorder (ASD). The infant siblings of children with ASD (high-risk siblings) exhibit a broad range of social-emotional outcomes, including subtle and frank disturbances associated with ASD. Here, we employed micro-analytic methods to examine the positive emotional engagement of low-risk infants and high-risk infants with and without ASD outcomes as they interacted with their parents.
Early Positive Emotional Development
Over the first half year of life, infants engage in increasingly mutual and responsive social interactions (Cohn & Tronick, 1987; Kaye & Fogel, 1980; Lin & Green, 2009). Expressions of positive affect, such as smiles, are a common focus of these interactions, and the frequency of infant smiles increases during this period (Kaye & Fogel, 1980; Messinger, Fogel, & Dickson, 1999). A longstanding literature focuses on the dynamics of dyadic exchanges that provide the foundation for social and emotional reciprocity (e.g., Feldman, 2007; Kochanska, 2002). Micro-analytic approaches have provided a particularly useful way to capture and model the complexity and richness of smiling interactions. Contingency analyses of infant-parent interaction, for example, quantify the likelihood of the parent influencing the infant, and of the infant influencing the parent (Bigelow & Power, 2014; Cohn & Tronick, 1987; McQuaid et al., 2009; Messinger et al., 2010; Symons & Moran, 1994; Messinger et al., 2014).
Although infant responsiveness to parent smiling appears to increase in the first six months (Messinger et al., 2010), it may be that initial increases in responsiveness plateau after three months. Kaye and Fogel (1980) found evidence of increasing infant responsiveness to mother smiles between one and a half and three months, but not between three and six months. Likewise, Bigelow and Power (2014) found evidence for an increase in infant smiling responsiveness from one month to two and three months, while Symons and Moran (1994) describe an increase in mother but not infant responsiveness in this period. To clarify these mixed results, we examined age effects on positive emotional engagement in the time period surrounding six months (5–7 months).
The face-to-face/still-face protocol (FFSF) provides a rich context to investigate early positive emotional development including the emergence of contingent responsiveness between infants and caregivers (Bigelow & Power, 2014; McQuaid et al., 2009). The FFSF allows for the investigation of positive emotional engagement (i.e., smiling rate and contingent responsiveness) in two conditions. The initial face-to-face play episode functions as a baseline and the reunion episode assays infant and parent recovery from the still-face, a period of parental non-responsiveness that functions as an age-appropriate stressor (Chow, Haltigan, & Messinger, 2010).
Positive Emotional Engagement in ASD
Responding to others’ emotional expressions is essential for successful social development, and disruptions in emotional responsiveness are a core deficit in children with ASD, which affects 1 in 68 children in the United States (American Psychiatric Association, 2013; Centers for Disease Control & Prevention, 2014). Although deficits in positive emotional engagement among children with ASD are frequently noted, the manifestation of those deficits may be subtle (Dawson, Hill, Spencer, Galpert, & Watson, 1990; Joseph & Tager-Flusberg, 1997; Kanner, 1943; Kasari, Sigman, & Yirmiya, 1993; Trad, Bernstein, Shapiro, & Hertzig, 1993). For example, Dawson et al. (1990) found that young children with autism (30 to 70 months) showed similar overall levels of smiling during a face-to-face interaction with their mothers as mental age-matched controls. However, children with autism were less likely to respond to their mothers’ smiles than control children. As ASD is not commonly diagnosed before three years of age, little is known about the early development of positive emotional engagement in infants at risk for the disorder. The longitudinal study of high-risk siblings allows for the prospective examination of positive emotional development in infants at elevated risk for ASD. Approximately one-fifth of high-risk siblings will go on to an ASD diagnosis, with another fifth developing subclinical difficulties with social and communicative behavior (Georgiades et al., 2013; Messinger et al., 2013; Ozonoff et al., 2011).
The development of positive emotional engagement in high-risk infants sheds light on the timing of the emergence of ASD-related differences in smiling behaviors. Filliter et al. (2014) reported that high-risk siblings with ASD outcomes exhibited lower rates of smiling during interactions with an examiner than high-risk siblings without ASD and low-risk infants at 12 months, but these differences were not apparent at 6 months. In fact, there are no reports before 12 months for differences in smiling during infant-parent interactions between high-risk and low-risk siblings (Merin et al., 2007; Yirmiya et al., 2006), or between infants with an eventual ASD diagnosis and other infants (Rozga et al., 2011; Young, Merin, Rogers, & Ozonoff, 2009). These studies did not, however, examine the rate of infant smiling onsets nor infant smiling in response to parent smiling. As suggested by Rozga et al. (2011), more detailed measures of dynamic responses to parent smiling during interactions may be necessary to understand patterns of contingent infant-parent affective behavior in the context of ASD risk.
Interaction is reciprocal such that infant and parental smiling responsiveness are frequently associated (Bigelow & Power, 2014). Interaction with a less emotionally responsive child, for example, might influence parental behavior. Dawson et al. (1990) found that mothers of children with autism smiled less frequently and were less likely to smile in response to their children’s smiles than other mothers (Dawson et al., 1990). For parents of high-risk siblings, levels of positive emotional engagement may be influenced by having an older child with ASD, increased parental concerns regarding the younger sibling’s development, or by symptoms of ASD in some high-risk siblings (Wan et al., 2012; Zwaigenbaum et al., 2007). Yirmiya et al. (2006), for example, found that parents of high-risk siblings exhibited less synchronous coordination of their engagement states when interacting with their four-month-olds than parents of low-risk infants. However, previous studies have not directly examined positive emotional engagement in parents of high-risk siblings using a micro-analytic measurement approach.
The Current Study
The purpose of this study was to extend our understanding of positive emotional development by examining infants between five and seven months of age at varying risk for deficits in positive emotional engagement during interaction with their parents. Positive emotional engagement was indexed by smiling rate and contingent responsiveness during the face-to-face and re-engagement episodes of the FFSF.
Methods
Participants
Infant-parent dyads were enrolled in a prospective, longitudinal investigation of the social and emotional development of infants at low or elevated risk for ASD. The current study focuses on data collected at the 6-month and 36-month assessments. Institutional review board approval and parental consent for participation were obtained. Infants were recruited from the metropolitan area of a large city in the southeastern United States. Recruitment strategies included referrals from a university-based autism center and mailings to parents whose addresses and names were obtained from county birth records.
Sixty-eight infant-parent dyads were included in the current study (43 high-risk, 25 low-risk). High-risk status was defined as having at least one older sibling diagnosed with ASD (Autistic Disorder, Asperger’s Disorder, or Pervasive Developmental Disorder-Not Otherwise Specified) based on DSM-IV-TR diagnostic criteria (American Psychiatric Association, 2000). Older sibling diagnoses were confirmed for the high-risk group by the Autism Diagnostic Observation Schedule (ADOS; Lord et al., 2000) and clinical diagnosis by a licensed psychologist. Low-risk infants had no older siblings with an ASD diagnosis or ASD symptomatology, as determined by a score of nine or lower on the Social Communication Questionnaire (Rutter, Bailey, & Lord, 2003). Of the 68 parents, 63 were mothers and 5 were fathers; 65 were married and no information on marital status was available for the remaining three parents. Infant age ranged from 5.05 – 6.92 months (M = 6.03 months, SD = .35). The sample was highly educated and predominantly Caucasian/Non-Hispanic and Hispanic/Latino (see Table 1).
Table 1.
Sample Characteristics
| Characteristic | Low-Risk (n = 25) |
High-Risk/No ASD (n = 32) |
High-Risk /ASD (n = 11) |
p | Effect size |
|---|---|---|---|---|---|
| Age (months), Mean (SD) | 6.01 (.39) | 6.04 (.27) | 6.06 (.46) | .90 | <.01 |
| Male, n (%) | 14 (56.0%) | 19 (59.4%) | 6 (54.4%) | .95 | .04 |
| Ethnicity, n (%) | .66 | .29 | |||
| Caucasian/Non-Hispanic | 11 (44.0%) | 13 (40.6%) | 6 (54.5%) | ||
| Hispanic/Latino | 11 (44.0%) | 13 (40.6%) | 4 (36.4%) | ||
| Black/African-American | 1 (4.0%) | 1 (3.1%) | 0 (0%) | ||
| Asian/Asian-American | 1 (4.0%) | 1 (3.1%) | 1 (9.1%) | ||
| Mixed Ethnicity/Other | 1 (4.0%) | 4 (12.5%) | 0 (0%) | ||
| Maternal Education, n (%) | .90 | .23 | |||
| High school | 0 (0%) | 1 (3.1%) | 0 (0%) | ||
| Some college | 2 (8.0%) | 4 (12.5%) | 1 (9.1%) | ||
| 2-year college | 4 (16.0%) | 6 (18.8%) | 1 (9.1%) | ||
| 4-year college | 6 (24.0%) | 9 (28.1%) | 2 (18.2%) | ||
| Advanced/Professional degree | 13 (52.0%) | 12 (37.5%) | 7 (63.6%) | ||
| # of Siblings, Mean (SD) | 1.72 (1.70) | 1.41 (.62) | 1.82 (1.72) | .55 | .02 |
| Maternal Age, Mean (SD) | 33.96 (4.31) | 35.50 (4.26) | 36.55 (5.84) | .24 | .04 |
| Paternal Age, Mean (SD) | 36.68 (5.99) | 38.69 (5.01) | 38.55 (7.05) | .40 | .03 |
Note. P-values reflect ANOVA comparisons for age, number of siblings, and parental age and chi-square tests for gender, ethnicity, and maternal education. Effect sizes reflect partial eta squared values for continuous variables and phi values for categorical variables.
Procedure and Measures
Face-to-face/still face (FFSF)
At six months, parents and infants participated in the FFSF (Adamson & Frick, 2003; Mesman, van IJzendoorn, & Bakersman-Kranenburg, 2009). Parents were seated directly in front of the child and instructed to play with the infant for three minutes (face-to-face), stop interacting and maintain a neutral expression for two minutes (still-face), and finally resume interaction with the infant for three minutes (reunion). If infants cried continuously for 20 seconds, the episode was abbreviated. The average length of the face-to-face episode was 3.00 minutes (range: 1.15–3.18 minutes) and the average length of the reunion episode was 2.92 minutes (range: .77–3.08 minutes). The mean duration of infants’ smiles was 4.35 seconds (SD = 3.08) in the face-to-face and 4.07 seconds (SD = 2.79) in the reunion. Parents smiled for a mean duration of 8.38 seconds (SD = 9.12) in the face-to-face and 7.39 seconds (SD = 7.46) in the reunion.
Coding of parent and infant smiles
Separate video recordings of the infants’ and the parents’ upper bodies and faces were synchronously acquired during the FFSF. Independent frame-by-frame coding (29.97 frames/second) of infant and parent smiling (presence or absence) was conducted by coders certified in the Facial Action Coding System (FACS; Ekman & Friesen, 1978) and trained in BabyFACS, its application to infants (Oster, 2006). Twenty percent of both the infant (κ = .84, 94.44% agreement) and parent sample were double coded for reliability (κ = .76, 91.01% agreement).
Positive emotional engagement variables
We analyzed infant and parent smiling rate and contingent responsiveness during the two interactive episodes of the FFSF (face-to-face and reunion). The face-to-face indexed baseline levels of positive emotional engagement and the reunion indexed positive emotional engagement after an age appropriate stressor.
Smiling rate and contingent responsiveness were defined in parallel fashion for infants and parents and are phrased here with respect to the infant. Infant smiling rate was defined by the number of infant smile onsets per minute as follows:
| Eq1 |
where ni,freq indicates the total frequency of infant smile onsets within the episode and nmin indicates the duration of the episode in minutes.
Infant contingent responsiveness (Bigelow & Power, 2014; McQuaid et al., 2009) reflects the proportion of parent smiles to which the infant responds; this proportion is adjusted for the total number of infant smiles, which disallows frequent infant smiling as a path to high responsiveness. Specifically, contingent responsiveness is the geometric mean of : 1) the frequency of infant smile onsets within 1 second of a parent smile onset divided by the total frequency of parent smile onsets and 2) the frequency of infant smile onsets within 1 second of a parent smile onset divided the by the total frequency of infant smile onsets. The geometric mean produces a standard, conservative assessment of contingent responsiveness as follows:
| Eq2 |
where ni,resp indicates the frequency of infant smile onsets within 1 second of a parent smile onset, np,freq indicates the total frequency of parent smile onsets within the episode, and nj,freq indicates the total frequency of infant smile onsets within the episode. Infant and parent contingent responsiveness were calculated individually for each FFSF episode.
ASD outcome
At 36 months, infants received a diagnostic evaluation from a licensed psychologist blind to risk group. Clinical best-estimate diagnosis was informed by the ADOS, Mullen Scales of Early Learning (Mullen, 1995), and Autism Diagnostic Interview-Revised (Lord et al., 1994). None of the 25 low-risk siblings were diagnosed with ASD (Low-Risk group). Of the 43 high-risk siblings, 11 were diagnosed with ASD (High-Risk/ASD group) and 32 were not (High-Risk/No ASD group). The percentage (25.6%) of high-risk siblings diagnosed with ASD is comparable to the proportion of ASD outcomes in a larger report of the Baby Siblings Research Consortium (Ozonoff et al., 2011). The outcome groups were comparable on all demographic variables (see Table 1).
Results
Preliminary Analyses
In calculating contingent responsiveness, if an infant or parent did not smile in an episode, their partner’s responsiveness could not be calculated. One High-Risk/No ASD infant, seven High-Risk/No ASD parents, two High-Risk/ASD parent, and one Low-Risk parent were missing at least one contingent responsiveness value. Contingent responsiveness values for infants and parents in the face-to-face and reunion episodes were significantly different from zero, all t > 6.16, all p < .001, all Cohen’s d > 1.60 (see Table 2). Thus, both infants and parents exhibited contingent responsiveness.
Table 2.
Descriptive Information for Smile Variables
|
|
||||
|---|---|---|---|---|
| Variable | Smiling Rate M (SD) | Contingent Responsiveness M (SD) | ||
|
| ||||
| Face-to-Face | Reunion | Face-to-Face | Reunion | |
| Infant | ||||
| Low-Risk | 4.73 (2.57) | 2.95 (1.98) | .13 (.09) | .13 (.09) |
| High-Risk/No ASD | 3.42 (2.36) | 2.66 (2.64) | .09 (.09) | .07 (.10) |
| High-Risk/ASD | 3.09 (1.45) | 3.27(1.37) | .12 (.08) | .12 (.07) |
| Parent | ||||
| Low-Risk | 8.33 (5.73) | 8.25 (5.40) | .11 (.10) | .09 (.09) |
| High-Risk/No ASD | 6.47 (4.94) | 6.29 (4.75) | .11 (.12) | .10 (.12) |
| High-Risk/ASD | 9.13 (5.55) | 9.72 (5.18) | .08 (.07) | .11 (.05) |
Note. M = Mean, SD = Standard Deviation.
Correlations among infant and parent smile variables were assessed using a Bonferroni correction (28 tests, p < .002). Infant smiling rate and infant contingent responsiveness were positively associated within and across the face-to-face and reunion episodes (see Table 3). Parent smiling rate was positively correlated between the face-to-face and reunion episodes.
Table 3.
Correlations between Infant and Parent Smile Variables
| Variable | Infant | Parent | ||||||
|---|---|---|---|---|---|---|---|---|
|
| ||||||||
| Smiling Rate | Contingent Responsiveness | Smiling Rate | Contingent Responsiveness | |||||
|
| ||||||||
| Face-to-Face | Reunion | Face-to-Face | Reunion | Face-to-Face | Reunion | Face-to-Face | Reunion | |
| Infant | ||||||||
| Smile Frequency | ||||||||
| Face-to-Face | – | |||||||
| Reunion (n) | .62* (68) | – | ||||||
| Contingent Responsiveness | ||||||||
| Face-to-Face (n) | .48* (67) | .35 (67) | – | |||||
| Reunion (n) | .38* (67) | .46* (67) | .37* (67) | – | ||||
| Parent | ||||||||
| Smiling Rate | ||||||||
| Face-to-Face (n) | .10 (68) | .13 (68) | .22 (67) | .15 (67) | – | |||
| Reunion (n) | .06 (68) | .07 (68) | .09 (67) | .14 (67) | .80* (68) | – | ||
| Contingent Responsiveness | ||||||||
| Face-to-Face (n) | .32 (64) | .06 (64) | −.01 (63) | .11 (63) | .31 (64) | .23 (64) | – | |
| Reunion (n) | .33* (60) | .29 (60) | .09 (59) | .12 (59) | .22 (60) | .17 (60) | .31 (58) | – |
Note. Significant with Bonferroni correction (p < .002).
Neither infant nor parent smiling rates (all p > .40, all partial η2 < .01), or parent (all p > .08, all partial η2 < .05) or infant (all p > .10, all partial η2 < .04) contingent responsiveness differed by infant gender. Infant gender was not included in subsequent analyses. Infant age was not associated with parent smiling rate or contingent responsiveness. However, older age was associated with higher rates of infant smiling, r(66) = .33, p < .01 and higher levels of contingent responsiveness, r(65) = .29, p = .02, in the reunion episode. Age was included as a covariate in subsequent analyses of infant smiling.
Group Differences for Smiling Rate and Responsiveness
Infant smiling rate
A 3 (Group) × 2 (Episode) repeated measures ANCOVA of infant smiling rate with age as a covariate yielded no main effect of outcome group, F(2, 64) = 1.35, p = .27, partial η2 = .04, or episode, F(1, 64) = 1.89, p = .17, partial η2 = .03. However, a significant interaction between outcome group and episode emerged, F(2, 64) = 4.18, p = .02, partial η2 = .12 (see Figure 1). To follow-up, repeated measures ANOVAs of smiling rate between episodes were conducted within each outcome group (see Table 2). Infants in the Low-Risk group exhibited a significant decrease in their rate of smiling from the face-to-face to reunion episodes, F(1, 24) = 29.95, p < .01, partial η2 = .56, and infants in the High-Risk/No ASD showed a similar but not significant reduction, F(1, 31) = 3.87, p = .06, partial η2 = .11. In contrast, infants in the High-Risk/ASD group did not reduce smiling rate between the face-to-face and reunion episodes, F(1, 10) = .12, p = .73, partial η2 = .01. The significant age covariate, F(1, 64) = 6.05, p = .02, partial η2 = .09, indicated a positive association between infant age and smiling rate.
Figure 1. Infant Smiling Rate across the Face-to-Face and Reunion Episodes by ASD Outcome Group.
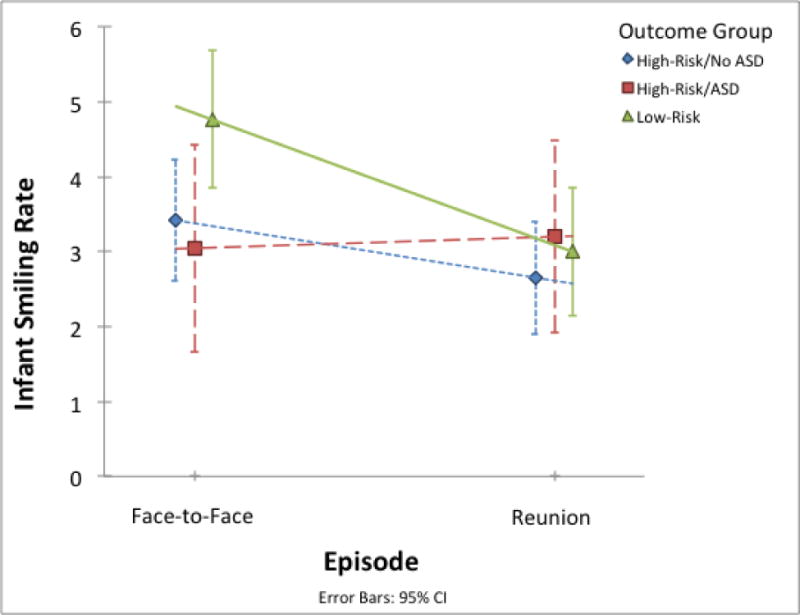
Note. Low-risk infants smiled less frequently in the reunion than the face-to-face episode, a pattern that was attenuated in high-risk infants without later ASD, and absent in high-risk infants ASD outcomes. Error bars indicate the 95% confidence intervals for the mean of each subgroup in each episode.
Infant contingent responsiveness
A 3 (Group) × 2 (Episode) repeated measures ANCOVA of infant contingent responsiveness with age as a covariate, yielded a main effect of outcome group on infant contingent responsiveness, F(2, 63) = 3.83, p = .03, partial η2 = .11 (see Figure 2 and Table 2). There was no main effect of episode, F(1, 63) = 1.14, p = .29, partial η2 = .02, or interaction between outcome group and episode, F(2, 63) = .31, p = .74, partial η2 = .01. Planned comparisons of the group effect indicated that the High-Risk/No ASD infants showed lower levels of contingent responsiveness than Low-Risk infants, t(2, 63) = 2.63, p = .01. The High-Risk/No ASD group did not differ from the High-Risk/ASD group, t(2, 63) = 1.64, p = .10. The significant age covariate, F(1, 64) = 5.21, p = .03, partial η2 = .08, indicated a positive association between infant age and contingent responsiveness.
Figure 2. Infant Contingent Responsiveness across the Face-to-Face and Reunion Episodes by Outcome Group.
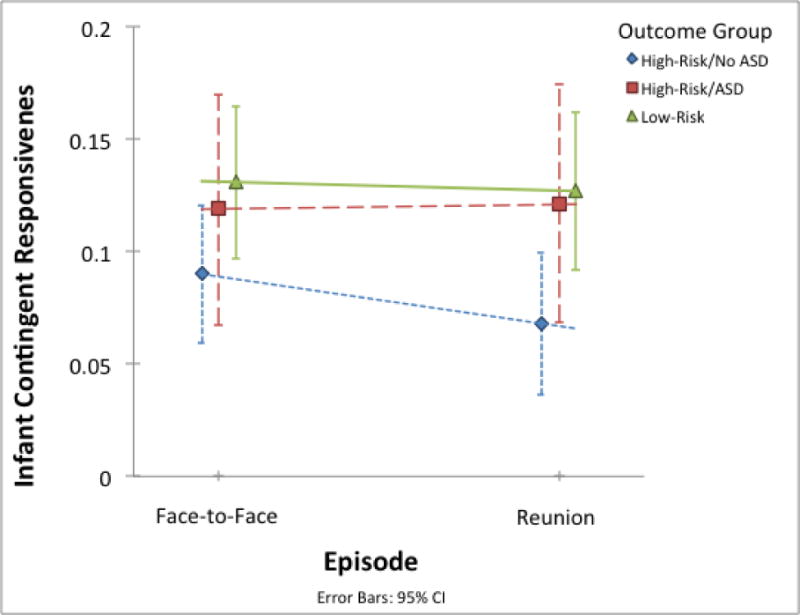
Note. Infant contingent responsiveness differed by outcome group. In repeated-measures (face-to-face and reunion) analyses, high-risk infants without ASD showed less contingent responsiveness than low-risk infants, but did not differ from high-risk infants with eventual ASD. Error bars indicate the 95% confidence intervals for the mean of each subgroup in each episode.
Parent smiling rate and contingent responsiveness
Separate 3 (Group) × 2 (Episode) repeated measures ANOVAs were conducted for smiling rate and contingent responsiveness among parents (see Table 2). For parent smiling rate, there were no main effects of outcome group, F(2, 65) = 1.97, p = .15, partial η2 = .06, or episode, F(1, 65) = .06, p = .81, partial η2 = .00, and no interaction effect, F(2, 65) = .23, p = .80, partial η2 = .01. Likewise, for parent contingent responsiveness, there were no main effects of outcome group, F(2, 55) = .17, p = .85, partial η2 = .01, or episode, F(1, 55) = .21, p = .65, partial η2 = .00, and no interaction effect, F(2, 55) = .62, p = .55, partial η2 = .02.
Discussion
We investigated positive emotional engagement during infant-parent interactions in infants between five and seven months of age who received diagnoses of ASD or no ASD at three years. Unlike low-risk infants, high-risk infants later diagnosed with ASD did not show the expected decrease in smiling between the face-to-face and reunion episodes of the FFSF, which is characteristic of the still-face effect. However, it was not infants with later ASD outcomes, but instead high-risk infants who did not have ASD outcomes, who were less likely to smile in response to their parent than low-risk infants.
Development of Positive Emotional Responsiveness
We used micro-analytic coding of infant and parent smile onsets to examine each partner’s responsiveness. Both the frequency of infant smile onsets and levels of infant contingent smile responsiveness were positively associated with age in the short interval between five and seven months. These results extend previous literature, suggesting robust increases in infant emotional contingent responsiveness beyond the first three months of life (Bigelow & Power, 2014; Symons & Moran, 1994), which may be relevant to the emergence of more coordinated communication in the second half year of life. Our findings are consistent with previous work showing comparable levels of mean contingent responsiveness among parents and infants from one to three months of age (Bigelow & Power, 2014). However, both the current levels of contingent responsiveness and those of Bigelow and Power are lower than those reported in a similar study of four- to five-month-olds and their parents (McQuaid et al., 2009). McQuaid et al. calculated contingent responsiveness only for smiles that coincided with mutual gaze and employed briefer (by one minute each) FFSF episodes, factors that may be responsible for bolstering levels of contingent responsiveness. In all, the current results suggest the utility of longitudinal examinations of contingent responsiveness for understanding interactive dynamics both among typically developing infants, and those at increased risk for neurodevelopmental disorders.
ASD Risk and Positive Emotional Engagement in Infants
Little research to date has examined the early manifestation of positive emotional engagement, particularly positive emotional responsiveness, among infants at elevated risk for ASD. We found that high-risk siblings without eventual ASD were less likely to respond to parent smiles than low-risk siblings; however, deficits in responsiveness were not associated with ASD outcome. Although unexpected, these results are similar to previous findings of decreases in social smiling in high-risk siblings that were not directly associated with later ASD diagnosis (Gangi, Ibañez, & Messinger, 2014; Nichols et al., 2014). Thus, deficits in smile responsiveness among high-risk infant siblings may be a feature of familial autism risk rather than a specific risk factor for the disorder.
Infant smiling rate did not differ by outcome group, but an intriguing interaction with episode emerged. Low-risk infants’ smiling rate declined from the face-to-face to reunion episodes. This “still-face effect,” suggests that a brief episode of parental non-responsiveness depressed the infants’ proclivity to initiate positive affect with the parent (Mesman et al., 2009). This pattern was attenuated in high-risk infants without later ASD, and absent in high-risk infants with ASD outcomes. Previous investigations employing brief face-to-face, still-face, and reunion episodes (1 minute each) reporting the results of interval coding or total durations of smiling did not yield group differences (Rozga et al., 2011; Young et al., 2009). These results raise the possibility that the absence of an expected reduction in smile initiations among six-month-olds following a period of parental non-responsiveness is associated with later ASD outcomes, which, if replicated, might foster early detection and intervention efforts.
Parent Positive Emotional Engagement
In the current study, parents of high-risk siblings did not differ from parents of low-risk siblings in frequency of smiling or in responsiveness to infant smiles. Previous ratings of free-play suggest that that the parents of high-risk siblings with and without ASD outcomes are more directive than the parents of low-risk infants at six months (Wan et al., 2012). Likewise, Yirmiya et al. (2006) found these parents to be less responsive during face-to-face interaction. However, neither investigation examined the occurrence and context of individual parent behaviors such as smiles. Despite the possibility of qualitative differences in parent interactive style, parents of children with and without ASD in the current study did not differ in level of emotional engagement despite the attenuations in the positive emotional engagement of their infants documented here.
Future Directions and Conclusion
Infant and parent affective engagement were examined within a small developmental interval, highlighting the need for longitudinal studies of emotional engagement in high-risk infants. Smiling rate measures do not reflect differences in the intensity of infant and parent smiling associated with ASD outcome groups, which is a task for future research. Replication of the subtle effects documented here with a larger sample of infants (11 infants in the current sample had ASD outcomes) is a necessity. Nevertheless, the current results suggest a general developmental relationship between early positive emotional engagement and autism risk and a specific relation to autism outcome.
Acknowledgments
The research reported in this article was supported by grants from the National Institute of Child Health and Development (R01HD057284 & R01HD047417), the National Institute of General Medical Sciences (R01GM105004), and the National Science Foundation (1052736). We thank the families who participated in this research.
Footnotes
Nicole M. McDonald is now at the Child Study Center, Yale School of Medicine.
Whitney I. Mattson is now at the Department of Psychology, University of Michigan.
Contributor Information
Brittany L. Lambert-Brown, Department of Psychology, University of Miami.
Nicole M. McDonald, Department of Psychology, University of Miami.
Whitney I. Mattson, Department of Psychology, University of Miami
Katherine B. Martin, Department of Psychology, University of Miami
Lisa V. Ibañez, Department of Psychology, University of Washington
Wendy L. Stone, Department of Psychology, University of Washington
Daniel S. Messinger, Departments of Psychology, Pediatrics, Electrical & Computer Engineering, and Music Engineering, University of Miami
References
- Adamson LB, Frick JE. The still face: A history of a shared experimental paradigm. Infancy. 2003;4:451–473. doi: 10.1207/S15327078IN0404_01. [DOI] [Google Scholar]
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 5. Arlington, VA: American Psychiatric Publishing; 2013. [Google Scholar]
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 4. Washington, DC: American Psychiatric Publishing; 2000. text revision. [Google Scholar]
- Bigelow AE, Power M. Effects of maternal responsiveness on infant responsiveness and behavior in the still-face task. Infancy. 2014;19:558–584. doi: 10.1111/infa.12059. [DOI] [Google Scholar]
- Cassel TD, Messinger DS, Ibanez LV, Haltigan JD, Acosta SI, Buchman AC. Early social and emotional communication in the infant siblings of children with autism spectrum disorders: An examination of the broad phenotype. Journal of Autism and Developmental Disorders. 2007;37(1):122–132. doi: 10.1007/s10803-006-0337-1. [DOI] [PubMed] [Google Scholar]
- Centers for Disease Control and Prevention. Prevalence of autism spectrum disorder among children aged 8 years—Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2010. MMWR. 2014;63:1–21. [PubMed] [Google Scholar]
- Chow S, Haltigan JD, Messinger DS. Dynamic Infant-Parent Affect Coupling during the Face-to-Face/Still-Face. Emotion. 2010;10:101–114. doi: 10.1037/a0017824. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cohn J, Tronick E. Mother-infant face-to-face interaction: The sequence of dyadic states at 3, 6, and 9 months. Developmental Psychology. 1987;23:68–77. doi: 10.1037/0012-1649.23.1.68. [DOI] [Google Scholar]
- Dawson G, Hill D, Spencer A, Galpert L, Watson L. Affective exchanges between young autistic children and their mothers. Journal of Abnormal Child Psychology. 1990;18:335–345. doi: 10.1007/BF00916569. [DOI] [PubMed] [Google Scholar]
- Ekman P, Friesen W. The Facial Action Coding System. Palo Alto, CA: Consulting Psychologists Press; 1978. [Google Scholar]
- Feldman R. Mother-infant synchrony and the development of moral orientation in childhood and adolescence: Direct and indirect mechanisms of developmental continuity. American Journal of Orthopsychiatry. 2007;77:582–597. doi: 10.1037/0002-9432.77.4.582. [DOI] [PubMed] [Google Scholar]
- Filliter JH, Longard J, Lawrence MA, Zwaigenbaum L, Brian J, Garon N, et al. Positive affect in infant siblings of children diagnosed with autism spectrum disorder. Journal of Abnormal Child Psychology. 2014 doi: 10.1007/s10802-014-9921-6. [DOI] [PubMed] [Google Scholar]
- Gangi DN, Ibañez LV, Messinger DS. Joint attention initiation with and without positive affect: Risk group differences and associations with ASD symptoms. Journal of Autism and Developmental Disorders. 2014;44:1414–1424. doi: 10.1007/s10803-013-2002-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Georgiades S, Szatmari P, Zwaigenbaum L, Bryson S, Brian J, Roberts W, et al. A prospective study of autistic-like traits in unaffected siblings of probands with autism spectrum disorder. JAMA Psychiatry. 2013;70(1):42–48. doi: 10.1001/2013.jamapsychiatry.1. [DOI] [PubMed] [Google Scholar]
- Gronborg TK, Schendel DE, Parner ET. Recurrence of autism spectrum disorders in full- and half-siblings and trends over time: A population-based cohort study. JAMA Pediatrics. 2013;167:947–953. doi: 10.1001/jamapediatrics.2013.2259. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Joseph RM, Tager-Flusberg H. An investigation of attention and affect in children with autism and Down syndrome. Journal of Autism and Developmental Disorders. 1997;27(4):385–396. doi: 10.1023/A:1025853321118. [DOI] [PubMed] [Google Scholar]
- Kanner L. Autistic disturbances of affective contact. Nervous Child. 1943;2:217–250. [PubMed] [Google Scholar]
- Kasari C, Sigman M, Yirmiya N. Focused and social attention of autistic children in interactions with familiar and unfamiliar adults: A comparison of autistic, mentally retarded, and normal children. Development and Psychopathology. 1993;5:403–414. doi: 10.1017/S0954579400004491. [DOI] [Google Scholar]
- Kaye K, Fogel A. The temporal structure of face.to-face communication between mothers and infants. Developmental Psychology. 1980;16:454–464. doi: 10.1017/S0954579400004491. [DOI] [Google Scholar]
- Kochanska G. Mutually responsive orientation between mothers and their young children: A context for the early development of conscience. Current Directions in Psychological Science. 2002;11:191–195. doi: 10.1111/1467-8721.00198. [DOI] [Google Scholar]
- Lin H, Green JA. Infants’ expressive behaviors to mothers and unfamiliar partners during face-to-face interactions from 4 to 10 months. Infant Behavior & Development. 2009;32(3):275–285. doi: 10.1016/j.infbeh.2009.03.002. [DOI] [PubMed] [Google Scholar]
- Lord C, Rutter M, DiLavore P, Risi S. Autism Diagnostic Observation Schedule (ADOS) manual. Los Angeles, CA: Western Psychological Services; 2000. [Google Scholar]
- Lord C, Rutter M, Le Couteur A. Autism diagnostic interview-revised: a revised version of a diagnostic interview for caregivers of individuals with possible pervasive developmental disorders. Journal of Autism and Developmental Disorders. 1994;24(5):659–685. doi: 10.1007/BF02172145. [DOI] [PubMed] [Google Scholar]
- McQuaid NE, Bibok MB, Carpendale JIM. Relation between maternal contingent responsiveness and infant social expectations. Infancy. 2009;14(3):390–401. doi: 10.1080/15250000902839955. [DOI] [PubMed] [Google Scholar]
- Merin N, Young GS, Ozonoff S, Rogers SJ. Visual fixation patterns during reciprocal social interaction distinguish a subgroup of 6-month-old infants at-risk for autism from comparison infants. Journal of Autism and Developmental Disorders. 2007;37:108–121. doi: 10.1007/s10803-006-0342-4. [DOI] [PubMed] [Google Scholar]
- Mesman J, van IJzendoorn MH, Bakermans-Kranenburg MJ. The many faces of the still-face paradigm: A review and meta-analysis. Developmental Review. 2009;29:120–162. doi: 10.1016/j.dr.2009.02.001. [DOI] [Google Scholar]
- Messinger D, Duvivier LL, Warren Z, Mahoor M, Baker J, Warlaumont AS, Ruvolo P. Affective Computing, Emotional Development, and Autism. In: Calvo R, editor. Handbook of Affective Computing. NY: Oxford University Press; 2014. [Google Scholar]
- Messinger D, Fogel A, Dickson KL. What’s in a smile? Developmental Psychology. 1999;35(3):701–708. doi: 10.1037/0012-1649.35.3.701. [DOI] [PubMed] [Google Scholar]
- Messinger DS, Ruvolo P, Ekas NV, Fogel A. Applying machine learning to infant interaction: The development is in the details. Neural Networks. 2010;23:1004–1016. doi: 10.1016/j.neunet.2010.08.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Messinger D, Young GS, Ozonoff S, Dobkins K, Carter A, Zwaigenbaum L, et al. Beyond autism: A baby sibling research consortium study of high-risk children at three years of age. Journal of the American Academy of Child and Adolescent Psychiatry. 2013;52(3):300–308. doi: 10.1016/j.jaac.2012.12.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mullen E. Mullen scales of early learning. Circle Pines, MN: American Guidance Service; 1995. [Google Scholar]
- Nichols CM, Ibañez LV, Foss-Feig JH, Stone WL. Social smiling and its components in high-risk infant siblings without later ASD symptomatology. Journal of autism and developmental disorders. 2014;44(4):894–902. doi: 10.1007/s10803-013-1944-2.. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Oster H. Unpublished monograph and coding manual, Department of Psychology. New York University; New York City: 2006. Baby FACS: Facial Action Coding System for Infants and Young Children. [Google Scholar]
- Ozonoff S, Young GS, Carter A, Messinger D, Yirmiya N, Zwaigenbaum L, et al. Recurrence risk for autism spectrum disorders: A baby siblings research consortium study. Pediatrics. 2011;128(3):e488–e495. doi: 10.1542/peds.2010-2825. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rozga A, Hutman T, Young GS, Rogers SJ, Ozonoff S, Dapretto M, et al. Behavioral profiles of affected and unaffected siblings of children with autism: Contribution of measures of mother-infant interaction and non-verbal communication. Journal of Autism and Developmental Disorders. 2011;41(3):287–301. doi: 10.1007/s10803-010-1051-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rutter M, Bailey A, Lord C. The Social Communication Questionnaire Manual. Los Angeles: Western Psychological Services; 2003. [Google Scholar]
- Symons D, Moran G. Responsiveness and dependency are different aspects of social contingencies: An example from mother and infant smiles. Infant Behavior and Development. 1994;17(2):209–214. doi: 10.1016/0163-6383(94)90057-4. [DOI] [Google Scholar]
- Trad PV, Bernstein D, Shapiro T, Hertzig M. Assessing the relationship between affective responsiveness and social interaction in children with pervasive developmental disorder. Journal of Autism and Developmental Disorders. 1993;23:361–377. doi: 10.1177/1359104508100890. [DOI] [PubMed] [Google Scholar]
- Wan MW, Green J, Elsabbagh M, Johnson M, Charman T, Plummer F, BASIS Team Quality of interaction between at-risk infants and caregiver at 12–15 months is associated with 3-year autism outcome. Journal of Child Psychology and Psychiatry. 2012;54(7) doi: 10.1111/jcpp.12032. [DOI] [PubMed] [Google Scholar]
- Yirmiya N, Gamliel I, Pilowsky T, Feldman R, Baron-Cohen S, Sigman M. The development of siblings of children with autism at 4 and 14 months: Social engagement, communication, and cognition. The Journal of Child Psychology and Psychiatry. 2006;47:511–523. doi: 10.1111/j.1469-7610.2005.01528.x. [DOI] [PubMed] [Google Scholar]
- Young GS, Merin N, Rogers SJ, Ozonoff S. Gaze behavior and affect at 6 months: Predicting clinical outcomes and language development in typically developing infants and infants at risk for autism. Developmental Science. 2009;12(5):798–814. doi: 10.1111/j.1467-7687.2009.00833.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zwaigenbaum L, Thurm A, Stone W, Baranek G, Bryson S, Iverson J, et al. Studying the emergence of autism spectrum disorders in high-risk infants: Methodological and practical issues. Journal of Autism and Developmental Disorders. 2007;3:466–480. doi: 10.1007/s10803-006-0179-x. [DOI] [PubMed] [Google Scholar]