

Highlights
-
•
We present a rare case of huge retroperitoneal cystic lymphangioma, diagnosed radiologically.
-
•
The lymphangioma was successfully resected laparoscopically after aspiration using a SAND balloon catheter.
-
•
Our case demonstrates the feasibility of minimally invasive laparoscopic resection of such lesions.
Keywords: Double balloon catheter, Laparoscopic surgery, Lymphangioma
Abstract
Introduction
Retroperitoneal cystic lymphangiomas are rare. We report a case of retroperitoneal huge cystic lymphangioma that was successfully aspirated the cyst’s contents with double balloon catheter and excised laparoscopically.
Presentation of case
A 34-year-old man was admitted to our hospital with low-grade fever and abdominal pain that had lasted for 1 week. Abdominal computed tomography and magnetic resonance imaging showed a fluid-filled multilocular mass measuring 13.5 cm in diameter around the tail of the pancreas, which was diagnosed as a retroperitoneal cystic lymphangioma. We successfully excised the tumor by laparoscopic distal pancreatosplenectomy. We punctured and aspirated the tumor with a double-balloon catheter to decrease the tumor’s size without spilling the tumor content. Cytology showed no malignant cells, and histopathological examination confirmed cystic lymphangioma. No recurrence was noted on radiographic imaging 10 months postoperatively.
Discussion and conclusion
Laparoscopic treatment for retroperitoneal huge cystic lymphangioma is feasible, and the double balloon catheter is useful for reducing the tumor volume.
1. Introduction
Cystic lymphangiomas are congenital benign tumors of the lymphatic system. More than 95% of cystic lymphangiomas occur in the head, neck, and axilla, with only 1% occurring in the retroperitoneum. Laparotomy was selected in previous cases for treating huge retroperitoneal cystic lymphangiomas [1,2]. However, this open procedure often results in greater postoperative pain and poor cosmetic appearance. With recent advances in surgical equipment and techniques, more minimally invasive procedures with laparoscopy for the treatment of large tumors are indicated [3].
In this paper, we describe a case in which laparoscopic treatment was used for a huge retroperitoneal cystic lymphangioma, and we also describe the usefulness of the double balloon catheter (SAND balloon catheter) for reducing the tumor’s volume. Written informed consent was obtained from the patient.
2. Case presentation
A 34-year-old man without any relevant medical history was admitted to our hospital with an abdominal tumor with a low-grade fever and abdominal pain that had lasted for 1 week. The tumor, located in the upper abdomen, could be palpated on physical examination. Routine laboratory and hematologic investigations showed normal parameters, except for white blood cell count, which was 9100/mm3 (normal range, 4000–8000/mm3). Abdominal computed tomography showed a fluid-filled multilocular mass measuring 13.5 cm in diameter around the tail of the pancreas without obvious infiltration (Fig. 1A). A T2-weighted magnetic resonance image showed a high signal-intensity tumor without a solid component, and the wall of the mass was thin and smooth (Fig. 1B). Thus, the radiological diagnosis of retroperitoneal lymphangioma was established and laparoscopic excision was performed.
Fig. 1.
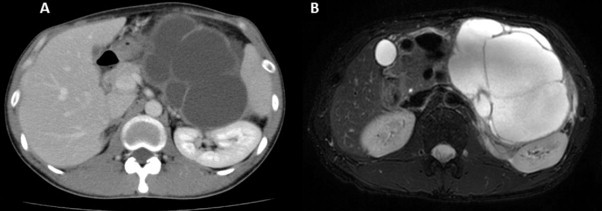
Abdominal computed tomography and magnetic resonance imaging of the present case.
(A) Abdominal computed tomography showed a fluid-filled multilocular mass measuring 13.5 cm in diameter around the tail of the pancreas. (B) A T2-weighted magnetic resonance image showed a high signal-intensity tumor without a solid component.
After the induction of general anesthesia, the patient was placed in a supine position. A camera port was inserted into an umbilical incision. A pneumoperitoneum of 12 mm Hg was created, and 4 additional ports (1 port with a diameter of 12 mm and 3 with a diameter of 5 mm) were inserted into the left upper, right lower, left lower, and right upper quadrants, under laparoscopic imaging. The tumor was located on the pancreatic tail; however, detailed laparoscopic observation of the lesion site was difficult due to the huge tumor size. A double balloon catheter (SAND balloon catheter, Hakko Medical, Tokyo, Japan) was then utilized to decrease the tumor’s volume and to obtain a good exposure of the lesion. The tumor was aspirated carefully under laparoscopy using the SAND balloon catheter without spilling any of the tumor content (Fig. 2). About 1 L of brownish serous fluid was removed from the cyst. After fluid aspiration, the entry hole was sutured with 3.0 monocryl (Ethicon, Tokyo, Japan). The tumor was tightly adherent to the pancreas, splenic artery, and splenic vein and was not able to be dissected (Fig. 3); thus, distal pancreatosplenectomy was performed. Surgical duration was 254 min and the estimated blood loss was 293 mL. Cytology of cyst’s contents showed no malignant cells and histopathological examination confirmed a cystic lymphangioma (Fig. 4). No recurrence was noted on radiographic imaging 10 months postoperatively.
Fig. 2.
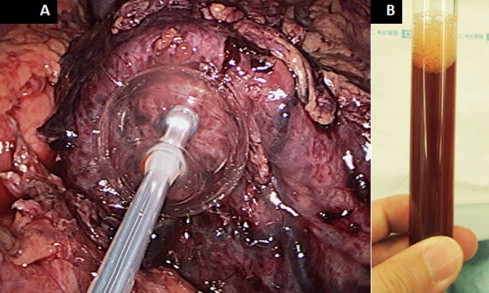
Laparoscopic view of the SAND balloon catheter and contents of the cyst.
(A) A SAND balloon catheter was utilized to decrease the tumor’s volume and to obtain a good exposure of the lesion. (B) The tumor was aspirated carefully under laparoscopy using the catheter without spilling any of the tumor contents. The cyst contained a brownish serous fluid.
Fig. 3.
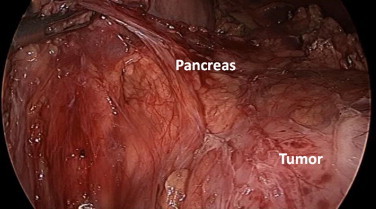
Laparoscopic view of the tumor, which was tightly adherent to the pancreas.
Because of the tight adhesions to the pancreas, splenic artery, and splenic vein, the tumor was not able to be dissected, and thus pancreatosplenectomy was performed.
Fig. 4.
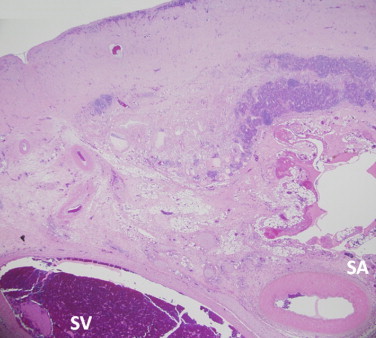
Photomicrograph of the wall of the cyst and the splenic artery and vein.
The photomicrograph shows that the wall of the cyst is tightly adherent to the splenic artery and vein through the fibrous tissue (hematoxylin and eosin staining, ×20).
3. Discussion
Cystic lymphangiomas are rare benign tumors of the lymphatic system that are more common in the pediatric population. Lymphangiomas are typically asymptomatic, but if patients have symptoms that necessitate therapeutic intervention, surgical resection is the best choice [4]. In spite of its benign nature, retroperitoneal lymphangioma can rarely recur in young patients [5]; therefore, complete resection is necessary for reducing the risk of recurrence.
Laparoscopic or retroperitoneal laparoscopic resections have sometimes been chosen to reduce postoperative pain and cosmetic issues [6–10]. However, to manage a huge tumor, decreasing the tumor volume by aspirating cystic contents without spillage is required to permit mobilization and removal of the tumor. In this case, we used a specially designed SAND balloon catheter for aspiration to minimize spilling the cyst’s contents into the retroperitoneal cavity. SAND balloon catheter has two balloons, namely a distal balloon and a proximal transparent one near its tip. After the entire distal balloon is inserted into the cyst, the distal balloon is then inflated with 10 mL of saline solution. The proximal balloon is inflated in the same way while the inflated distal balloon is retracted. The punctured cyst wall is sandwiched between the two inflated balloons, which can minimize spilling the cyst’s contents. This balloon catheter was developed primarily for laparoscopic cystectomy of benign ovarian cysts [11]. Yagihashi et al. previously successfully used a SAND balloon catheter to resect a cystic lymphangioma [3].
The laparoscopic approach for the retroperitoneal cystic lymphangioma was technically feasible through careful separation of the cyst from adjacent structures. The use of the SAND balloon catheter to decrease tumor volume prior to resection was associated with no complications. This minimally invasive technique also improves patient comfort, with less postoperative pain, rapid recovery after surgery, and minimal scar formation. Laparoscopic excision should therefore, be considered as a therapeutic option to treat retroperitoneal huge cystic lymphangiomas.
Conflicts of interest
All authors certify that they have no commercial associations that might pose a conflict of interest in connection with submitted article.
Funding
All authors certify that they have no sponsors regarding submitted article.
Ethical approval
Ethics Committee’s approval is unnecessary for this case report, and written informed consent was obtained from the patient.
Consent
A written informed consent was obtained from the patient.
Author contribution
YI, HT, HH, NI, KK and SN helped to draft the manuscript. KY, SH, SA, TN, JY and KH have revised the manuscript critically. All authors read and approved the final manuscript.
Acknowledgment
All authors certify that they have no commercial associations that might pose a conflict of interest in connection with submitted article.
References
- 1.de Perrot M., Rostan O., Morel P. Abdominal lymphangioma in adults and children. Br. J. Surg. 1998;85:395–397. doi: 10.1046/j.1365-2168.1998.00628.x. [DOI] [PubMed] [Google Scholar]
- 2.Baseskioglu B., Bilen C.Y., Erkan I. Laparoscopic management of giant hygroma renalis. Int. J. Urol. 2012;19:484–485. doi: 10.1111/j.1442-2042.2011.02948.x. [DOI] [PubMed] [Google Scholar]
- 3.Yagihashi Y., Kato K., Nagahama K., Yamamoto M., Kanamaru H. A case of laparoscopic excision of a huge retroperitoneal cystic lymphangioma. Case Rep. Urol. 2011;2011:1–3. doi: 10.1155/2011/712520. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Fattahi A.S., Maddah G., Motamedolshariati M. Chronic low back pain due to retroperitoneal cystic lymphangioma. Arch. Bone Joint Surg. 2014;2:72–74. [PMC free article] [PubMed] [Google Scholar]
- 5.Ozdemir H., Kocakoc E., Bozgeyik Z. Recurrent retroperitoneal cystic lymphangioma. Yonsei Med. J. 2005;46:715–718. doi: 10.3349/ymj.2005.46.5.715. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Celia A., Breda G. Laparoscopic excision of a retroperitoneal cystic lymphangioma: an insidious case. J. Laparoendosc. Adv. Surg. Tech. A. 2007;17:315–316. doi: 10.1089/lap.2006.0167. [DOI] [PubMed] [Google Scholar]
- 7.Singh R.R., Govindarajan K.K., Bowen C. Retroperitoneal cystic lymphangioma: a rare presentation in childhood, treated laparoscopically. J. Laparoendosc. Adv. Surg. Tech. A. 2009;19:249–250. doi: 10.1089/lap.2008.0234. [DOI] [PubMed] [Google Scholar]
- 8.Trindade E.N., Trindade M.R., Boza J.C. Laparoscopic excision of a retroperitoneal cystic lymphangioma in an elderly patient. Minerva Chir. 2007;62:145–147. [PubMed] [Google Scholar]
- 9.Tsukamoto T., Tanaka S., Yamamoto T. Laparoscopic excision of a retroperitoneal cystic lymphangioma: report of a case. Surg. Today. 2003;33:142–144. doi: 10.1007/s005950300032. [DOI] [PubMed] [Google Scholar]
- 10.Wildhaber B.E., Chardot C., Le Coultre C. Total laparoscopic excision of retroperitoneal cystic lymphangioma. J. Laparoendosc. Adv. Surg. Tech. A. 2006;16:530–533. doi: 10.1089/lap.2006.16.530. [DOI] [PubMed] [Google Scholar]
- 11.Takeda A., Imoto S., Mori M. Management of large adnexal tumors by isobaric laparoendoscopic single-site surgery with a wound retractor. Eur. J. Obstet. Gynecol. Reprod. Biol. 2013;166:185–189. doi: 10.1016/j.ejogrb.2012.10.016. [DOI] [PubMed] [Google Scholar]