

Abstract
Background
Immunoglobulin (Ig) G4-related disease (IgG4-RD) is characterized by elevated serum IgG4 and infiltration of IgG4+ plasma cells into multiple organs. It is not known whether serum IgG4 is autoreactive in IgG4-RD.
Methods
We measured anti-nuclear antibody (ANA) in 19 IgG4-RD cases, determined IgG subclasses of the ANA, and compared them with those of other systemic autoimmune diseases (systemic lupus erythematosus, Sjögren’s syndrome, systemic sclerosis, and polymyositis), using subclass-based ANA test (indirect immunofluorescence).
Results
58 % of IgG4-RD cases were ANA-positive (cut-off: 1:40). Whereas their subclass of ANA was predominantly IgG2, we observed no IgG4-type ANA. In systemic autoimmune diseases, subclasses of ANA were mostly IgG1, 2, or 3, but IgG4-type ANA was very rarely detected. We also found several patients in whose serum ANA patterns differed among IgG subclasses, probably due to the difference of corresponding autoantigens.
Conclusions
Although IgG4 is highly elevated in sera of IgG4-RD patients, their ANA do not include IgG4 subclass. These results offer new insight into the role of IgG4 and the pathogenesis of IgG4-RD, implying that each IgG subclass tends to cover its own spectrum of antigens, and IgG4 is not preferentially used to make ANA.
Keywords: IgG4-related disease, Systemic autoimmune disease, IgG subclass, Autoantibody, Anti-nuclear antibody
Background
Immunoglobulin (Ig) G4-related disease (IgG4-RD) is a multi-organ disorder characterized by elevated serum IgG4, organ infiltration by IgG4+ plasma cells, hypergammaglobulinemia, and tissue sclerosis [1–4]. Many organs, such as lacrimal gland, salivary gland, eye orbit, lymph node, thyroid gland, lung, pancreas, kidney, retroperitoneum, and prostate can be affected by IgG4-RD. The role of IgG4 in IgG4-RD is not sufficiently understood. Some view IgG4-RD as an allergic disease, because IgG4-RD is often complicated in allergic diseases and serum IgE levels are often high in IgG4-RD. Others see IgG4-RD as an autoimmune disease, because anti-lactoferrin [5] and carbonic anhydrase II [6] antibodies are detected in some of IgG4-related autoimmune pancreatitis cases, and because IgG4-RD cases usually show good responses to glucocorticoid therapies.
At this point, there is no consensus that IgG4-related disease is an autoimmune disorder. To examine whether IgG4 in IgG4-RD is autoreactive, we determined IgG subclasses of serum anti-nuclear antibody (ANA) in IgG4-RD patients and compared them with those in patients with systemic autoimmune diseases such as systemic lupus erythematosus (SLE), Sjögren’s syndrome (SS), systemic sclerosis (SSc), and polymyositis (PM). Using a subclass-based ANA test that was derived from indirect immunofluorescence (IIF), we investigated how frequently IgG4 was included in ANA in IgG4-RD. We also examined how frequently each IgG subclass was included in ANA in systemic autoimmune diseases.
Methods
Patients
Patients were recruited from Department of Rheumatology and Clinical Immunology, Kyoto University Hospital, Kyoto, Japan. The patients were definitely diagnosed by the 2011 Comprehensive Diagnostic Criteria proposed by the IgG4-RD research team of Ministry of Health, Labour and Welfare (MHLW), Japan [4]: (1) diffuse or localized swelling or mass formation of ≥ 1 organs, (2) elevated serum IgG4 levels ≥135 mg/dL, (3a) fibrosis with remarkable infiltration of lymphocytes and plasma cells, and (3b) IgG4+/IgG+ plasma cell ratio > 0.4, and > 10 IgG4+ plasma cells in a high-power field. No IgG4-RD patients were considered having SS, Castleman’s disease, sarcoidosis, granulomatosis with polyangiitis, or malignant lymphoma. As ANA-positive disease controls, we enrolled 8 SLE patients diagnosed by the 1997 American College of Rheumatology revised criteria [7], 8 SS patients diagnosed by the 1999 revised criteria of MHLW, Japan [8], 4 SSc patients diagnosed by the 1980 American College of Rheumatology criteria [9], and 7 PM patients diagnosed by Bohan and Peter’s criteria [10]. All participants provided informed consent in accordance with the Declaration of Helsinki. This study was approved by the Medical Ethics Committee of Graduate School of Medicine and Faculty of Medicine, Kyoto University.
Detection of subclass-specific ANA
We performed subclass-based ANA tests based on the Fluoro-HepANA™ test (Medical & Biological Laboratories, Nagoya, Japan). Briefly, HEp-2 cell-coated slides were incubated with sera, washed with PBS, incubated with FITC-labeled second antibodies, and observed with a fluorescence microscope. Instead of using anti-total human IgG antibody as the second antibody, we used anti-IgG1 (ab50473, Abcam), anti-IgG2 (10122, Alpha Diagnostic Intl.), anti-IgG3 (10123, Alpha Diagnostic Intl.), or anti-IgG4 antibodies (ab99821, Abcam). To detect total-IgG ANA, patients’ sera are usually diluted by the ratios starting from 1:40. To detect each IgG-subclass ANA, the sera were not diluted because of relatively low affinities of the second antibodies against subclasses.
Results
ANA positivity of IgG4-RD
Of 19 cases that definitely satisfied the 2011 Comprehensive Diagnostic Criteria for IgG4-RD by MHLW, Japan (Table 1), 14 (74 %) were older than 60 years, and 14 (74 %) were male. Lymph node swellings and retroperitoneal fibrosis were major manifestations. Eleven patients (58 %) were ANA-positive at a cut-off titer of 1:40 (range: 1:40–1:320). The ANA patterns were homogeneous + speckled or speckled in most cases. Although 7 (37 %) were positive for rheumatoid factor and 2 (11 %) were positive for anti-SS-A/Ro antibodies, we confirmed these 9 cases did not fulfill the criteria for rheumatoid arthritis (RA) or SS. No patients were positive for anti-DNA, Sm, or U1-RNP antibodies.
Table 1.
Clinical, serological, and histopathological features of IgG4-RD cases
| Case | Age | IgG4a | IgGa | ANA Specific Abs | RFb | Clinical manifestations | Biopsy source, IgG4+/IgG+ cell ratio |
|---|---|---|---|---|---|---|---|
| 1 | 73 | 2890 | 3668 | 40 (Homo + Spe) | <6 | Mikulicz’s disease, Prostatitis, LN | Prostate, 0.60 |
| 2 | 76 | 2210 | 3632 | 40 (Spe) | <6 | Mikulicz’s disease, RPF | Submandibular gl, 0.40 |
| 3c | 79 | 1460 | 3669 | 160 (Homo + Spe) Anti-SS-A+ | <6 | Küttner’s tumor, IP, IN, RPF, LN | Submandibular gl, 0.73 |
| 4 | 66 | 1090 | 2301 | 40 (Homo + Spe) | 30.3 | AIP, IN, Renal pseudotumor | Kidney, 0.70 |
| 5c | 73 | 592 | 3321 | 320 (Homo + Spe) | <6 | Sialadenitis, IP, IN, RPF, LN | Submandibular gl, 0.43 |
| 6 | 74 | 389 | 2184 | <40 | <6 | Retroorbital tumor | Retroorbital tumor, 0.48 |
| 7 | 52 | 383 | 1748 | <40 | <6 | Küttner’s tumor | Submandibular gl, 0.57 |
| 8 | 70 | 724 | 1729 | <40 | <6 | Küttner’s tumor, LN | Submandibular gl, 0.40 |
| 9 | 46 | 675 | 1617 | 80 (Homo + Spe) | 26.8 | Mikulicz’s disease | Lachrymal gl, 0.41 |
| 10 | 37 | 533 | 1741 | <40 | <6 | Mikulicz’s disease | Lachrymal gl, 0.50 |
| 11 | 76 | 458 | 1527 | <40 | <6 | AIP, RPF | Retroperitoneal tumor, 0.70 |
| 12 | 62 | 315 | 1809 | 40 (Spe) Anti-SS-A+ | <6 | AIP, RPF | Pancreas, 0.43 |
| 13 | 79 | 1960 | 2953 | 40 (Homo + Spe) | 65 | Orbital tumor, Lung nodule, LN | Orbital tumor, 0.59 |
| 14c | 62 | 1460 | 2177 | 40 (Spe) | 23.3 | Sialadenitis, Laryngeal tumor, LN | Parotid gl, 0.60 Cervical LN, 0.69 |
| 15 | 65 | 1050 | 1811 | <40 | 19.8 | Mikulicz’s disease, LN | Submandibular LN, 0.80 |
| 16 | 25 | 1210 | 2181 | <40 | <6 | Mikulicz’s disease, IP, IN, Renal pseudotumor, LN | Minor salivary gl, 0.65 |
| 17 | 55 | 1510 | 3116 | <40 | 72.2 | Orbital tumor, RPF, Lung nodule, LN | Cervical LN, 0.90 |
| 18 | 61 | 491 | 1466 | 80 (Spe + Granular) | <6 | Sialadenitis | Submandibular gl, 0.48 |
| 19 | 78 | 1470 | 3762 | 80 (Homo + Spe) | 35 | AIP, RPF | Vater’s ampulla, 0.48 |
amg/dL in serum. bIU/mL. cShown in Fig. 1
ANA: anti-nuclear antibody; gl: gland; Homo: homogeneous; IN: interstitial nephritis; IP: interstitial pneumonitis; LN: lymph node; RF: rheumatoid factor; RPF: retroperitoneal fibrosis; Spe: speckled
IgG subclasses of ANA in IgG4-RD
We selected 5 IgG4-RD patients robustly ANA-positive with a cut-off titer of 1:80, and examined the IgG subclasses of their ANA. Subclass-based ANA test showed IgG2+ ANA and scant IgG1+ ANA. However, we found no IgG4+ or IgG3+ ANA (Fig. 1, 2). We confirmed that the second antibody against IgG4 worked, using direct immunofluorescence on a lymph node specimen (IgG4+/IgG+ plasma cell ratio = 0.69) of an IgG4-RD patient (Fig. 1, lower right panel).
Fig. 1.
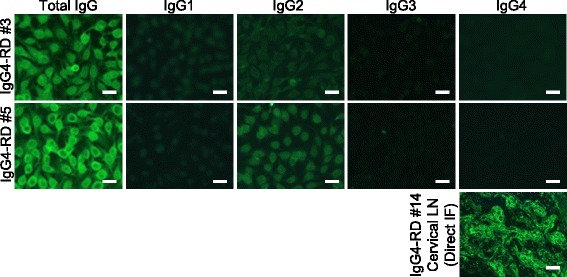
Subclass-based ANA test in IgG4-RD, showing immunofluorescence microscopy of two typical IgG4-RD cases (IgG4-RD #3 and #5). Lower right panel: We confirmed the second antibody’s function by direct immunofluorescence of a lymph node specimen (IgG4+/IgG+ plasma cell ratio = 0.69) from an IgG4-RD patient (IgG4-RD #14). Bar = 20 μm
Fig. 2.
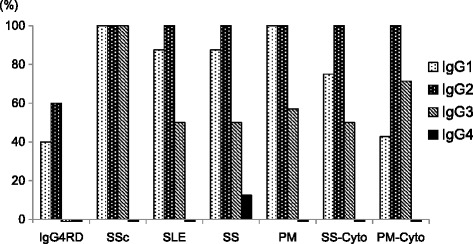
Positivity of each ANA subclass in IgG4-RD and systemic autoimmune diseases. Cyto: positivity of each subclass of anti-cytoplasmic antibody was also calculated for patients with Sjögren’s syndrome and polymyositis
IgG subclasses of ANA in systemic autoimmune diseases
We examined IgG subclasses of ANA in systemic autoimmune diseases such as SLE, SSc, SS, and PM (Table 2). The ANA titers ranged from 1:40 to 1:5120 with various patterns. The Subclass-based ANA test detected IgG1+, IgG2+, or IgG3+ ANA in the systemic autoimmune disease cases (Fig. 2, 3). Especially, all cases were IgG2+. However, IgG4 was not detected (Fig. 2, 3), except in a patient with SS who showed IgG4-type ANA with peripheral pattern (Fig. 4).
Table 2.
ANA profiles of patients with systemic autoimmune diseases
| Case | ANA | Specific autoantibodies | IgG4a | IgGa |
|---|---|---|---|---|
| SLE 1b | Spe 320 | dsDNA, ssDNA, U1-RNP, Sm | 21.3 | 1830 |
| SLE 2 | Homo + Spe 320 | dsDNA, ssDNA, SS-A | 11 | 826 |
| SLE 3 | Spe 1280 | dsDNA, ssDNA, Sm, Ribosome | 20 | 2043 |
| SLE 4 | Spe 640 | ssDNA, U1-RNP, Sm, SS-A, SS-B | 8.3 | 829 |
| SLE 5 | Homo + Spe 1280 | dsDNA, ssDNA, U1-RNP, Sm, SS-A, SS-B | 7 | 556 |
| SLE 6 | Homo + Spe 160 | ssDNA | 48.6 | 1938 |
| SLE 7 | Spe 320 | dsDNA, SS-A | 19.6 | 1186 |
| SLE 8 | Spe 5120 | dsDNA, ssDNA, U1-RNP, Sm, SS-A | 7 | 908 |
| SSc 1 | Discrete spe 1280 | Centromere | 7 | 1177 |
| SSc 2b | Discrete spe 1280, Spe 160, Cyto 80 | Centromere, SS-A | 21.2 | 1772 |
| SSc 3 | Spe 1280 | Scl-70, U1-RNP, SS-A | 25.5 | 2147 |
| SSc 4 | Discrete spe 1280 | Centromere, Scl-70, U1-RNP | 12.4 | 1108 |
| SS 1 | Spe 320 | SS-A, SS-B | 33.4 | 2974 |
| SS 2 | Spe 160 | SS-A, SS-B | 16.5 | 1765 |
| SS 3 | Spe 80 | SS-A, SS-B | 74 | 1370 |
| SS 4c | Spe 640 | SS-A | 228 | 1721 |
| SS 5 | Spe 40, Cyto 80 | SS-A | 38 | 2133 |
| SS 6 | Spe 160 | SS-A, SS-B | 14.5 | 2340 |
| SS 7 | Spe 160 | SS-A, SS-B | 9.5 | 1882 |
| SS 8b | Spe + Nucleolar 80, Cyto 40 | SS-A | 20.1 | 1678 |
| PM 1 | Spe + Nucleolar 640 | Ku | 53.5 | 1668 |
| PM 2b | Spe 320, Cyto 40 | ssDNA, U1-RNP, Sm, SS-A | 12.9 | 1132 |
| PM 3 | Spe 40, Cyto 160 | PL-7 | 15 | 717 |
| PM 4 | Spe 320 | U1-RNP, Sm | 5 | 282 |
| PM 5 | Spe 1280 | Ku, SS-A, SS-B | <3 | 823 |
| PM 6 | Spe 40, Cyto 80 | SRP | 18.4 | 1365 |
| PM 7 | Homo + Spe 160 | Not detected | 19 | 2051 |
Fig. 3.
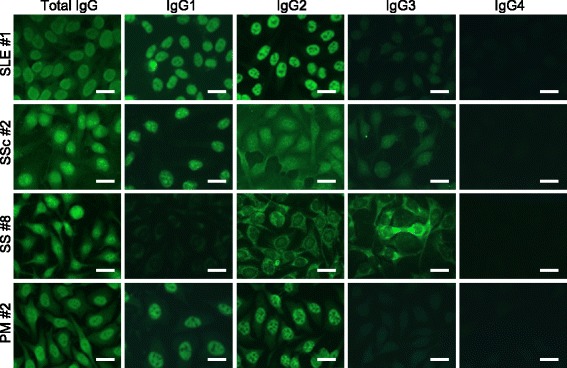
Subclass-based ANA test for systemic autoimmune diseases showing immunofluorescence microscopy for each typical case, including systemic lupus erythematosus (SLE #1), systemic sclerosis (SSc #2), Sjögren’s syndrome (SS #8) and polymyositis (PM #2) showed variation in ANA patterns among IgG subclasses. In SSc #2, total IgG showed Discrete spe + Speckled + Cyto, while IgG1 showed Discrete spe + Speckled, IgG2 showed Discrete spe + Speckled + Cyto, IgG3 showed Discrete spe + Cyto, and IgG4 showed negative. In SS #8, total IgG showed Speckled + Nucleolar + Cyto, while IgG1 and IgG2 showed Speckled + Cyto, IgG3 showed Nucleolar + Cyto, and IgG4 showed negative. Bar = 20 μm Discrete spe: discrete speckled, Cyto: cytoplasmic
Fig. 4.
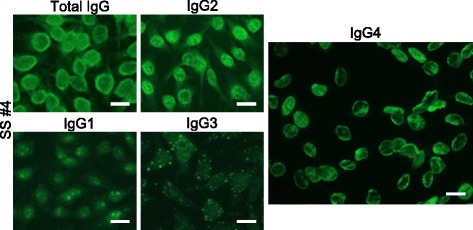
Subclass-based ANA test of a patient with Sjögren’s syndrome (SS #4) showing IgG4-type ANA. ANA patterns differed among IgG subclasses. Total IgG showed Speckled, while IgG2 showed Speckled + Cyto, IgG1 and IgG3 showed Nucleolar + Cyto (with atypical cytoplasmic spots), and IgG4 showed Peripheral. Bar = 20 μm. Cyto: cytoplasmic
An exceptional case with IgG4-type ANA
A 79-year-old male with SS showed IgG4-type ANA with peripheral pattern (Fig. 4). Lip biopsy results were compatible with SS, although anti-IgG4 staining was not performed. Anti-SS-A/Ro antibody was positive. We saw no swelling of lacrimal glands, salivary glands, or lymph nodes. This patient did not meet the criteria for IgG4-RD and was not considered to have clinical IgG4-RD.
Difference of ANA patterns among IgG subclasses
In serum from one patient, ANA patterns differed among IgG subclass. Such phenomenon was seen in Fig. 3 and 4.
Discussion
In IgG4-RD patients, we found no IgG4+ ANA, but did detect IgG1+ and IgG2+ ANA (Fig. 1 and 2). We also found IgG4+ ANA was very rare, whereas IgG1/2/3+ ANA were detected in systemic autoimmune diseases (Fig. 2 and 3). Autoantibodies with cytoplasmic patterns in the Fluoro-HepANA™ test are not exact ANA; “anti-cytoplasmic” antibodies—e.g., anti-SS-A/Ro, anti-aminoacyl-tRNA synthetase, and anti-signal recognition particle antibodies—are known in SS and PM. Subclass-based ANA tests found IgG1/2/3+ anti-cytoplasmic antibodies, but not IgG4 (Fig. 2, 3).
IgG4+ ANA is very rare in systemic autoimmune diseases, possibly because serum IgG4/IgG ratios are low, less than 5 %, in these diseases (Table 2). However, IgG4+ ANA was not detected despite high serum IgG4/IgG ratios (43 %) in IgG4-RD. This implies that IgG4 itself is not used to make ANA.
Several studies have investigated ANA subclasses in systemic autoimmune diseases. Zouali et al. reported that in SLE and mixed connective tissue disease, anti-double-stranded DNA (dsDNA) antibody was IgG1/3-dominant, and anti-RNP was IgG2-dominant [11]. Anti-Sm, anti-RNP, and anti-dsDNA in SLE [12], anti-SS-A/Ro and anti-SS-B/La in SS [13], and anti-Scl-70 in SSc [14] are reportedly IgG1-dominant. However, IgG4-type ANA was hardly detected in all the above reports. Rigopoulou et al. examined primary biliary cirrhosis cases, and found that ANA was IgG1/3-dominant but IgG4 was not detected by subclass-based IIF [15]. The reason IgG2-type ANA was remarkably frequent in our study whereas IgG1 and IgG3 were predominant in previous studies might be that second antibody affinities differed between studies. In the subclass-based ANA test, titers cannot be accurately compared between subclasses, as the second antibodies are different. In past studies, IgG2-type ANA was also detected at moderate levels, whereas IgG4-type ANA was constantly negative or at low levels. In our study, IgG4-type ANA was also hardly detected.
Autoimmune pancreatitis (AIP) is an organ-specific disorder seen in IgG4-RD. Various autoantibodies, such as anti-lactoferrin [5] and anti-carbonic anhydrase II [6] antibodies, are seen in AIP. Asada et al. found anti-pancreatic secretory trypsin inhibitor (PSTI) antibody in AIP, and showed that the titers of anti-PSTI antibody moved in parallel with serum IgG4 levels [16]. IgG4 levels change in parallel with IgG4-RD disease activity, as reported in many studies, including our previous study [17]. Asada et al. thought that anti-PSTI might be an important factor in the pathophysiology. However, immunoblotting of subclasses with anti-IgG1 or anti-IgG4 as second antibodies showed the subclass was not IgG4 but IgG1. Possibly, IgG4-type autoantibodies are difficult to produce in IgG4-RD patients.
However, some autoimmune diseases reportedly show IgG4-type autoantibodies. Rock et al. reported that IgG4 was the most common (100 %) of anti-desmoglein (Dsg)-1 antibodies detected in sera of patients with pemphigus foliaceus, and showed the pathogenicity of IgG4-type anti-Dsg-1 antibody using Balb/c mice [18]. Anti-Dsg-3 antibody in pemphigus vulgaris was also IgG4-predominant [19]. Beck et al. showed by immunoblotting that anti-phospholipase A2 receptor (PLA2R) antibody in idiopathic membranous nephropathy mainly consisted of IgG4 [20]. IgG4 is reportedly predominant in anti-neutrophil cytoplasmic antibody (ANCA). C-ANCA (IIF), proteinase-3 (PR3)-ANCA (ELISA), and myeloperoxidase (MPO)-ANCA (ELISA) in granulomatosis with polyangiitis (GPA) [21], and MPO-ANCA (ELISA) in propylthiouracil-induced vasculitis [22] were IgG1/4-dominant. Others similarly reported that IgG4 made up most C-ANCA (IIF) and PR3-ANCA (ELISA) in vasculitides [23, 24]. Engelmann et al. reported that anti-cyclic citrullinated peptide (CCP) antibody was IgG1/4-dominant in RA [25]. However, IgG4 in vasculitides and RA might not be pathophysiologically important. In functional analyses of ANCA, IgG1 and IgG3 PR3-ANCA can stimulate neutrophils [26], whereas IgG4 PR3-ANCA was only weakly stimulatory to neutrophils [27]. In RA patients who had HLA-DR4-shared epitope, Engelmann et al. found IgG3 anti-CCP antibody to be predominant, and considered that IgG3-type antibody might be more important in the pathophysiology of RA [28]. As IgG4 has poor ability to activate complements and antibody-dependent cellular cytotoxicity [29–32], IgG4 is unlikely to take part in mechanisms of tissue damage in autoimmune diseases.
Interestingly, there seem to be pathogenic and non-functional IgG4-type autoantibodies. IgG4-type ANCA is considered less pathogenic, compared to other subclass ANCA in ANCA-associated vasculitis [26, 27]. The affinities between IgG4-type and other subclass ANCA should be equal, but the abilities of complement activation are different, so that the role of IgG4-type ANCA can be less significant than that of other subclass ANCA. On the other hand, IgG4 anti-PLA2R antibody has high affinity and is considered pathogenic in idiopathic membranous nephropathy [20]. Why IgG4 anti-PLA2R antibody can exert pathogenicity without ability of complement activation may be because the pathogenicity is brought by the destruction of electrical barriers of glomerular basement membrane.
Taken together, IgG4 usage rates differ among autoantibodies and among diseases. IgG4 is associated with anti-Dsg-1/3, anti-PLA2R, anti-CCP antibodies, and ANCA, but not with anti-PTSI antibody in AIP or ANA in IgG4-RD and systemic autoimmune diseases (Table 3). This asymmetry implies that IgG4 has unknown but certain physiological or pathological functions. Further analyses are needed to know its role.
Table 3.
Summary of predominant subclasses in autoantibodies in IgG4-RD and autoimmune diseases
| Diseases | Autoantibodies | Predominant subclass | IgG4 subclass | Reports |
|---|---|---|---|---|
| IgG4-RD | ANA | IgG2 | Negative | Present study |
| IgG4-RD (AIP) | Anti-PSTI | IgG1 | Negative | Asada [16] |
| SLE, SSc, SS, PM | ANA | IgG1/2/3 | Seldom | Present study, Zouali [11], Eisenberg [12], Maran [13], Vazquez-abad [14] |
| GPA, Vasculitis | ANCA | IgG1, IgG4 | Frequent | Brouwer [21], Mellbye [23], Liu [24], Gao [22] |
| RA | ACPA | IgG1, IgG4 | Frequent | Engelmann [25] |
| PF, PV | Anti-Dsg-1/3 | IgG4 | Primary | Rock [18], Ding [19] |
| Idiopathic MN | Anti-PLA2R | IgG4 | Primary | Beck [20] |
ACPA: anti-citrullinated protein antibody; AIP: autoimmune pancreatitis; ANA: anti-nuclear antibody; ANCA: anti-neutrophil cytoplasmic antibody; Dsg-1/3: desmoglein-1 and 3; GPA: granulomatosis with polyangiitis; MN: membranous nephropathy; PF: pemphigus foliaceus; PLA2R: phospholipase A2 receptor; PSTI: pancreatic secretory trypsin inhibitor; PV: pemphigus vulgaris; RA: rheumatoid arthritis
In the present study, we observed ANA patterns differed among IgG subclasses in some cases (Fig. 3, 4). When a case has several autoantibodies, the utilized subclasses differ by autoantigens. This can be explained by the hypothesis that each IgG subclass prefers to cover its own spectrum of antigens. The reason we hardly found IgG4 in ANA might be that IgG4 does not cover antigens that can be detected by the ANA test—i.e., nuclear antigens or related microbial antigens. Selective IgG2 subclass deficiency is often associated with bacterial infection by Neisseria meningitidis and Streptococcus pneumoniae [33, 34], so that IgG2 is considered to have a role in protection from these bacteria. The role of IgG4 has not been sufficiently understood. If IgG4 is related to some microorganism type, and if the microorganism antigens and autoantigens are similar, as with Dsg-1/3, PLA2R, PR3, and citrullinated proteins, it would explain why IgG4-type antibody against those proteins was dominantly generated.
Our results imply that IgG4-RD is not an autoimmune disease, and that high levels of serum IgG4 in IgG4-RD are only nonspecific. Subclass-based ANA tests in this study covered both nuclear and cytoplasmic antigens in HEp-2 cells, and can screen a wide range of unmodified ubiquitous antigens. However, this analysis has limitations: modified antigens like citrullinated proteins and organ-specific antigens are not screened. The number of cases is limited in this study. There remains a possibility that unknown IgG4-type autoantibodies might be found in IgG4-RD. A further analysis is needed.
Conclusions
We found ANA in IgG4-RD patients are not IgG4-based despite high serum IgG4 levels. IgG4 was also hardly found in ANA in systemic autoimmune diseases. We also observed several patients in whom ANA patterns differed among IgG subclasses, probably due to difference in corresponding autoantigens. These findings imply that each IgG subclass tends to cover its own spectrum of antigens, and IgG4 is not apparently used to make ANA.
Acknowledgements
This study was supported by a grant for Research Program for Intractable Disease (the IgG4-related disease research team) from Ministry of Health, Labour and Welfare, Japan.
Abbreviations
- ANA
Anti-nuclear antibody
- ANCA
Anti-neutrophil cytoplasmic antibody
- AIP
Autoimmune pancreatitis
- CCP
Cyclic citrullinated peptides
- dsDNA
Double-stranded deoxyribonucleic acid
- Dsg
Desmoglein
- ELISA
Enzyme-linked immunosorbent assay
- GPA
Granulomatosis with polyangiitis
- HLA
Human leukocyte antigen
- IgG4-RD
Immunoglobulin G4-related disease
- IIF
Indirect immunofluorescence
- MPO
Myeloperoxidase
- PLA2R
Phospholipase A2 receptor
- PM
Polymyositis
- PR3
Proteinase-3
- PTSI
Pancreatic secretory trypsin inhibitor
- RA
Rheumatoid arthritis
- RNP
ribonucleoprotein
- SLE
Systemic lupus erythematosus
- SS
Sjögren’s syndrome
- SSc
Systemic sclerosis.
Footnotes
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
TM provided the idea of IgG4-subclass autoantibody in IgG4-RD. K. Kiyama and HY designed the study and collected the clinical data. K. Kiyama, HY, TK, and RN performed experiments and evaluations. DK gave significant suggestions and advice to the study. All the authors contributed to the composition of the manuscript.
Contributor Information
Kazuhiro Kiyama, Email: rheum@kuhp.kyoto-u.ac.jp.
Hajime Yoshifuji, Email: yossii@kuhp.kyoto-u.ac.jp.
Tsugumitsu Kandou, Email: kandou.tsugumitsu.35m@st.kyoto-u.ac.jp.
Yuji Hosono, Email: hosono25@kuhp.kyoto-u.ac.jp.
Koji Kitagori, Email: kitagori@kuhp.kyoto-u.ac.jp.
Ran Nakashima, Email: ranran@kuhp.kyoto-u.ac.jp.
Yoshitaka Imura, Email: imuray@kuhp.kyoto-u.ac.jp.
Naoichiro Yukawa, Email: naoichiy@kuhp.kyoto-u.ac.jp.
Koichiro Ohmura, Email: ohmurako@kuhp.kyoto-u.ac.jp.
Takao Fujii, Email: takfujii@kuhp.kyoto-u.ac.jp.
Daisuke Kawabata, Email: daisuke@kuhp.kyoto-u.ac.jp.
Tsuneyo Mimori, Email: mimorit@kuhp.kyoto-u.ac.jp.
References
- 1.Masaki Y, Dong L, Kurose N, Kitagawa K, Morikawa Y, Yamamoto M, et al. Proposal for a new clinical entity, IgG4-positive multiorgan lymphoproliferative syndrome: analysis of 64 cases of IgG4-related disorders. Ann Rheum Dis. 2009;68(8):1310–5. doi: 10.1136/ard.2008.089169. [DOI] [PubMed] [Google Scholar]
- 2.Okazaki K, Uchida K, Miyoshi H, Ikeura T, Takaoka M, Nishio A. Recent concepts of autoimmune pancreatitis and IgG4-related disease. Clin Rev Allergy Immunol. 2011;41(2):126–38. doi: 10.1007/s12016-010-8214-2. [DOI] [PubMed] [Google Scholar]
- 3.Umehara H, Okazaki K, Masaki Y, Kawano M, Yamamoto M, Saeki T, et al. A novel clinical entity, IgG4-related disease (IgG4RD): general concept and details. Mod Rheumatol. 2012;22(1):1–14. doi: 10.3109/s10165-011-0508-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Umehara H, Okazaki K, Masaki Y, Kawano M, Yamamoto M, Saeki T, et al. Comprehensive diagnostic criteria for IgG4-related disease (IgG4-RD), 2011. Mod Rheumatol. 2012;22(1):21–30. doi: 10.3109/s10165-011-0571-z. [DOI] [PubMed] [Google Scholar]
- 5.Okazaki K, Uchida K, Ohana M, Nakase H, Uose S, Inai M, et al. Autoimmune-related pancreatitis is associated with autoantibodies and a Th1/Th2-type cellular immune response. Gastroenterology. 2000;118(3):573–81. doi: 10.1016/S0016-5085(00)70264-2. [DOI] [PubMed] [Google Scholar]
- 6.Nishi H, Tojo A, Onozato ML, Jimbo R, Nangaku M, Uozaki H, et al. Anti-carbonic anhydrase II antibody in autoimmune pancreatitis and tubulointerstitial nephritis. Nephrol Dial Transplant. 2007;22(4):1273–5. doi: 10.1093/ndt/gfl672. [DOI] [PubMed] [Google Scholar]
- 7.Hochberg MC. Updating the American College of Rheumatology revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum. 1997;40(9):1725. doi: 10.1002/art.1780400928. [DOI] [PubMed] [Google Scholar]
- 8.Fujibayashi T, Sugai S, Miyasaka N, Hayashi Y, K T: Revised Japanese criteria for Sjögren’s syndrome (1999): availability and validity. Mod Rheumatol 2004(14):425–434. [DOI] [PubMed]
- 9.Preliminary criteria for the classification of systemic sclerosis (scleroderma). Subcommittee for scleroderma criteria of the American Rheumatism Association Diagnostic and Therapeutic Criteria Committee. Arthritis Rheum 1980, 23(5):581–590. [DOI] [PubMed]
- 10.Bohan A, Peter JB. Polymyositis and dermatomyositis (first of two parts) N Engl J Med. 1975;292(7):344–7. doi: 10.1056/NEJM197502132920706. [DOI] [PubMed] [Google Scholar]
- 11.Zouali M, Jefferis R, Eyquem A. IgG subclass distribution of autoantibodies to DNA and to nuclear ribonucleoproteins in autoimmune diseases. Immunology. 1984;51(3):595–600. [PMC free article] [PubMed] [Google Scholar]
- 12.Eisenberg RA, Dyer K, Craven SY, Fuller CR, Yount WJ. Subclass restriction and polyclonality of the systemic lupus erythematosus marker antibody anti-Sm. J Clin Invest. 1985;75(4):1270–7. doi: 10.1172/JCI111826. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Maran R, Dueymes M, Pennec YL, Casburn-Budd R, Shoenfeld Y, Youinou P. Predominance of IgG1 subclass of anti-Ro/SSA, but not anti-La/SSB antibodies in primary Sjogren's syndrome. J Autoimmun. 1993;6(3):379–87. doi: 10.1006/jaut.1993.1032. [DOI] [PubMed] [Google Scholar]
- 14.Vazquez-Abad D, Monteon V, Senecal JL, Walsh S, Rothfield N. Analysis of IgG subclasses of human antitopoisomerase I autoantibodies suggests chronic B cell stimulation. Clin Immunol Immunopathol. 1997;84(1):65–72. doi: 10.1006/clin.1997.4362. [DOI] [PubMed] [Google Scholar]
- 15.Rigopoulou EI, Davies ET, Pares A, Zachou K, Liaskos C, Bogdanos DP, et al. Prevalence and clinical significance of isotype specific antinuclear antibodies in primary biliary cirrhosis. Gut. 2005;54(4):528–32. doi: 10.1136/gut.2003.036558. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Asada M, Nishio A, Uchida K, Kido M, Ueno S, Uza N, et al. Identification of a novel autoantibody against pancreatic secretory trypsin inhibitor in patients with autoimmune pancreatitis. Pancreas. 2006;33(1):20–6. doi: 10.1097/01.mpa.0000226881.48204.fd. [DOI] [PubMed] [Google Scholar]
- 17.Kiyama K, Kawabata D, Hosono Y, Kitagori K, Yukawa N, Yoshifuji H, et al. Serum BAFF and APRIL levels in patients with IgG4-related disease and their clinical significance. Arthritis Res Ther. 2012;14(2):R86. doi: 10.1186/ar3810. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Rock B, Martins CR, Theofilopoulos AN, Balderas RS, Anhalt GJ, Labib RS, et al. The pathogenic effect of IgG4 autoantibodies in endemic pemphigus foliaceus (fogo selvagem) N Engl J Med. 1989;320(22):1463–9. doi: 10.1056/NEJM198906013202206. [DOI] [PubMed] [Google Scholar]
- 19.Ding X, Aoki V, Mascaro JM, Jr, Lopez-Swiderski A, Diaz LA, Fairley JA. Mucosal and mucocutaneous (generalized) pemphigus vulgaris show distinct autoantibody profiles. J Invest Dermatol. 1997;109(4):592–6. doi: 10.1111/1523-1747.ep12337524. [DOI] [PubMed] [Google Scholar]
- 20.Beck LH, Jr, Bonegio RG, Lambeau G, Beck DM, Powell DW, Cummins TD, et al. M-type phospholipase A2 receptor as target antigen in idiopathic membranous nephropathy. N Engl J Med. 2009;361(1):11–21. doi: 10.1056/NEJMoa0810457. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Brouwer E, Tervaert JW, Horst G, Huitema MG, van der Giessen M, Limburg PC, et al. Predominance of IgG1 and IgG4 subclasses of anti-neutrophil cytoplasmic autoantibodies (ANCA) in patients with Wegener's granulomatosis and clinically related disorders. Clin Exp Immunol. 1991;83(3):379–86. doi: 10.1111/j.1365-2249.1991.tb05647.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Gao Y, Ye H, Yu F, Guo XH, Zhao MH. Anti-myeloperoxidase IgG subclass distribution and avidity in sera from patients with propylthiouracil-induced antineutrophil cytoplasmic antibodies associated vasculitis. Clin Immunol. 2005;117(1):87–93. doi: 10.1016/j.clim.2005.06.002. [DOI] [PubMed] [Google Scholar]
- 23.Mellbye OJ, Mollnes TE, Steen LS. IgG subclass distribution and complement activation ability of autoantibodies to neutrophil cytoplasmic antigens (ANCA) Clin Immunol Immunopathol. 1994;70(1):32–9. doi: 10.1006/clin.1994.1007. [DOI] [PubMed] [Google Scholar]
- 24.Liu LJ, Chen M, Yu F, Zhao MH, Wang HY. IgG subclass distribution, affinity of anti-myeloperoxidase antibodies in sera from patients with Wegener's granulomatosis and microscopic polyangiitis. Nephrology. 2008;13(7):629–35. doi: 10.1111/j.1440-1797.2008.00976.x. [DOI] [PubMed] [Google Scholar]
- 25.Engelmann R, Brandt J, Eggert M, Karberg K, Krause A, Neeck G, et al. IgG1 and IgG4 are the predominant subclasses among auto-antibodies against two citrullinated antigens in RA. Rheumatology (Oxford) 2008;47(10):1489–92. doi: 10.1093/rheumatology/ken336. [DOI] [PubMed] [Google Scholar]
- 26.Holland M, Hewins P, Goodall M, Adu D, Jefferis R, Savage CO. Anti-neutrophil cytoplasm antibody IgG subclasses in Wegener's granulomatosis: a possible pathogenic role for the IgG4 subclass. Clin Exp Immunol. 2004;138(1):183–92. doi: 10.1111/j.1365-2249.2004.02566.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Hussain A, Pankhurst T, Goodall M, Colman R, Jefferis R, Savage CO, et al. Chimeric IgG4 PR3-ANCA induces selective inflammatory responses from neutrophils through engagement of Fcgamma receptors. Immunology. 2009;128(2):236–44. doi: 10.1111/j.1365-2567.2009.03108.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Engelmann R, Eggert M, Neeck G, Mueller-Hilke B. The impact of HLA-DRB alleles on the subclass titres of antibodies against citrullinated peptides. Rheumatology (Oxford) 2010;49(10):1862–6. doi: 10.1093/rheumatology/keq179. [DOI] [PubMed] [Google Scholar]
- 29.van der Zee JS, van Swieten P, Aalberse RC. Inhibition of complement activation by IgG4 antibodies. Clin Exp Immunol. 1986;64(2):415–22. [PMC free article] [PubMed] [Google Scholar]
- 30.Jefferis R, Reimer CB, Skvaril F, de Lange G, Ling NR, Lowe J, et al. Evaluation of monoclonal antibodies having specificity for human IgG sub-classes: results of an IUIS/WHO collaborative study. Immunol Lett. 1985;10(3–4):223–52. doi: 10.1016/0165-2478(85)90082-3. [DOI] [PubMed] [Google Scholar]
- 31.van der Neut KM, Schuurman J, Losen M, Bleeker WK, Martinez-Martinez P, Vermeulen E, et al. Anti-inflammatory activity of human IgG4 antibodies by dynamic Fab arm exchange. Science. 2007;317(5844):1554–7. doi: 10.1126/science.1144603. [DOI] [PubMed] [Google Scholar]
- 32.Aalberse RC, Schuurman J. IgG4 breaking the rules. Immunology. 2002;105(1):9–19. doi: 10.1046/j.0019-2805.2001.01341.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Hammarstrom L, Smith CI. IgG subclasses in bacterial infections. Monogr Allergy. 1986;19:122–33. [PubMed] [Google Scholar]
- 34.Escobar-Perez X, Dorta-Contreras AJ, Interian-Morales MT, Noris-Garcia E, Ferra-Valdes M. IgG2 immunodeficiency: association to pediatric patients with bacterial meningoencephalitis. Arq Neuropsiquiatr. 2000;58(1):141–5. doi: 10.1590/S0004-282X2000000100021. [DOI] [PubMed] [Google Scholar]