

Don't cringe when you hear the term “chelation (key-LAY-shun) therapy”. If you have heard about it at all, you may have heard it is alternative medicine, quackery, expensive, and even dangerous. New research funded by the National Institutes of Health is suggesting that this old treatment has some real life in it, and that it may particularly benefit patients with diabetes and prior heart attacks.
What is chelation therapy?
Chelation therapy was first used in the early 20th century to treat metal poisoning. The treatment involves administering a drug called a chelator, which has a magnetically charged pocket that can “grab” a metal and hang on to it, allowing it to be excreted in the urine- kind of like a baseball mitt with a magnet in its pocket. One chelator, calcium EDTA, is FDA approved to treat lead poisoning. Alternative medicine practitioners have been using a similar chelator, disodium EDTA, to treat heart disease, claiming to see benefits, since the 1950s.
Disodium EDTA chelation therapy is usually administered intravenously each week for 20 to 40 sessions. Each intravenous infusion may last hours. In spite of the expense and tedium, the 2008 National Health Statistics Report stated that in 2007, 111,000 people used chelation.
What does my doctor think about chelation?
Major cardiology organizations have published statements discouraging the use of chelation. These opinions were formed in the 1960s and 1970s, when the dosages and rate of administration of EDTA chelation had not been standardized, and there were safety problems, including kidney problems and even deaths. These opinions were so strong that until 2002, no large-scale clinical trial had been funded that could determine whether EDTA chelation harmed or benefitted cardiac patients.
So what is new about chelation in 2015?
There are reasons to think chelation to remove metals might treat or prevent heart disease1. Some complications of diabetes may be caused by chemical reactions that happen to the excess sugar in the blood. These reactions are catalyzed, or facilitated, by metals. The environment is polluted with metals that are toxic to our systems. Lead (gasoline, plumbing), arsenic (well water, rice, apple juice), mercury (many fish), and cadmium (from cell phone batteries) are among the top ten most toxic substances listed by the U.S. government. EDTA chelates lead and cadmium.
Concurrent with these conceptual developments, and because of the large number of Americans receiving chelation therapy, in 2002, the National Center for Complementary and Alternative Medicine and the National Heart Lung and Blood Institute funded a $30 million clinical trial of chelation therapy in patients age 50 or older with a prior heart attack and good kidney function to finally understand whether EDTA chelation for coronary disease was safe and effective. So the Trial to Assess Chelation Therapy (TACT) was born.
TACT enrolled 1,708 patients who were at least 50 years old and had a prior heart attack. The proposed treatment was intensive – 40 intravenous infusions, three hours each, all given over a little more than a year. Half of the patients received EDTA chelation. The other half received a saltwater placebo. Overall, patients received 55,222 IV infusions in 134 offices and hospitals across the US and Canada. Nearly a decade later, on August 15, 2012, we learned the results of our work. Did chelation work to reduce heart events in a vulnerable population with a prior heart attack? Turns out, it did. And it was safe.
Results of TACT
Overall, there was an 18% reduction in heart events (death, another heart attack, stroke, stenting or bypass, and hospitalization for heart pains) by EDTA infusions above and beyond that provided by our effective treatments including statins and aspirin2. When the group that took the EDTA infusions plus oral vitamins was analyzed, the reduction was by 26% compared with placebo3. The effect was even more striking in patients with diabetes, where there was a 41% reduction in clinical events (Figure 1), including a 43% reduction in deaths over 5 years4. There is nothing comparable in diabetes therapies.
Figure 1.
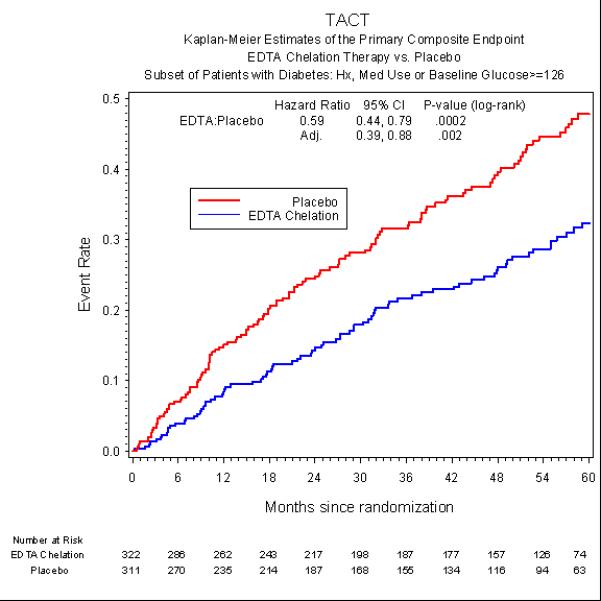
Risk of death, heart attack, stroke, stenting, bypass, or hospitalization for angina in patients with, or without chelation therapy. Reproduced with permission from Escolar et al.4
I had a heart attack and I have diabetes. Should I receive chelation?
The landscape for chelation therapy has changed, and environmental toxins may emerge as a modifiable risk factor for heart disease. The US Food and Drug Administration reviewed the TACT in a positive light, but they encouraged us to carry out another study to confirm these results (TACT2 is being planned). The American Heart Association, in its latest guidelines, has “upgraded” chelation from Class 3 (never ever do), to Class 2b (probably not effective). So the “official” answer is no.
But this is an emerging technology, and I believe our data. Clinicians sometimes race ahead of official guidelines. When asked, I recommend that patients seek their doctor's advice after their doctor has read the TACT papers referenced here. If a patient with diabetes and a prior heart attack wants chelation, I do not discourage them like I used to. And for high-risk patients in hospitals that offer chelation as a therapeutic choice, like mine, I recommend it. Finally, if your hospital is participating in the upcoming TACT2, currently in the very early planning phase, please get involved in the research. We still have a lot to learn.
Supplementary Material
Acknowledgments
Funding Sources
The National Heart, Lung, and Blood Institute and the National Center for Complementary and Alternative Medicine provided funding and oversight, grant # U01AT001156 and U01HL092607.
Footnotes
Disclosures
None
References
- 1.Solenkova NV, Newman JD, Berger JS, Thurston g, Hochman JS, Lamas GA. Metal Pollutants and Cardiovascular Disease: Mechanisms and Consequences of Exposure. Am Heart J. 2014 doi: 10.1016/j.ahj.2014.07.007. (in press) DOI: 10.1016/j.ahj.2014.07.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Lamas GA, Goertz C, Boineau R, Mark DB, Rozema T, Nahin RL, Lindblad L, Lewis EF, Drisko JA, Lee KL. Effect of disodium EDTA chelation regimen on cardiovascular events in patients with previous myocardial infarction: The TACT Randomized Trial. JAMA. 2013;309:1241–1250. doi: 10.1001/jama.2013.2107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Lamas G, Boineau R, Goertz C, Mark DB, Rosenberg Y, Stylianou M, Rozema T, Nahin RL, Chappell LT, Lindblad L, Lewis EF, Drisko J, Lee KL. EDTA Chelation Therapy Alone and in Combination with Oral High-Dose Multivitamins and Minerals for Coronary Disease: The Factorial Group Results of the Trial to Assess Chelation Therapy. Am Heart J. 2014;168:37–44. doi: 10.1016/j.ahj.2014.02.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Escolar E, Lamas G, Mark DB, Boineau R, Goertz C, Rosenberg Y, Nahin RL, Ouyang P, Rozema T, Magaziner A, Nahas R, Lewis EF, Lindblad L, Lee KL. The Effect of an EDTA-based Chelation Regimen on Patients with Diabetes and Prior Myocardial Infarction in TACT. Circ Cardiovasc Qual Outcomes. 2014;7:15–24. doi: 10.1161/CIRCOUTCOMES.113.000663. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.