

Abstract
Background
Lung cancer is the most common cancer and the leading cause of cancer death in China. Along with socioeconomic development, environmental problems have intensified and the burden of lung cancer continues to increase.
Methods
In this study, national cancer registry data was used for evaluating incidence, mortality, time trend, and prediction.
Results
In China in 2010, 605 900 patients were diagnosed and 486 600 patients died of lung cancer. Throughout the last three decades, the mortality of lung cancer has dramatically increased, as shown in national death surveys. From 2000 to 2010, age specific incidence of lung cancer increased in most age groups. It is estimated that in 2015, the total number of new cases of lung cancer will reach 733 300.
Conclusions
Lung cancer is a serious disease affecting public health and an effective control strategy is needed in China.
Keywords: Epidemiology, incidence, lung cancer, mortality
Introduction
Cancer is an emerging health issue in China and in many other countries. Lung cancer has been the leading cancer diagnosed and cause of cancer death for many years in China, with a rapidly increasing trend during the past several decades.1,2 The incidence rate of lung cancer in China is relatively high, but is increasing at a more rapid rate than in Western countries. Many risk factors, such as cigarette smoking and air pollution, have been proven as risk factors of the disease.3–6 With a large smoking population, the growth of lung cancer incidence in China will continue to rise. This article provides an up-to-date description of the epidemiology of lung cancer in China, which will provide an evidence base for future interventions to improve health in China.
Lung cancer has been the most common cancer in the world for several decades. There are estimated to be 1.8 million new cases in 2012 (12.9% of the total), 58% of which occurred in less developed regions. The disease remains the most common cancer in men worldwide (1.2 million, 16.7% of the total), with the highest estimated age-standardised incidence rates in Eastern Asia (50.4 per 100 000). Lung cancer is the most common cause of cancer death worldwide, estimated to be responsible for nearly one in five deaths (1.59 million deaths, 19.4% of the total). Because of its high fatality (the overall ratio of mortality to incidence is 0.87) and the relative lack of variability in survival in different world regions, the geographical patterns in mortality closely follow those of incidence. As the most populous country in the world, China contains 19% of the word population with 21.75% of all newly diagnosed cancer cases and 26.90% of deaths, including 35.78% of all newly diagnosed lung cancer cases and 37.56% of lung cancer deaths worldwide.7
Incidence
According to the National Central Cancer Registry (NCCR), including 145 cancer registries' data and accounting for 11.58% of the national population, in 2010, there were 605 946 new lung cancer diagnoses in China (416 333 men and 189 613 in women), accounting for 19.59% of all new cancer cases. The crude incidence rate was 46.08 per 100 000. The age-standardized rates by Chinese population 2000 (CASIR) were 35.23 per 100 000 and the age-standardized rates by world population (Segi's population, WASIR) were 35.04 per 100 000. Among the new cases, 348 107 (57.45%) came from urban areas and 257 839 (42.55%) from rural areas. Among patients aged 0–74, the cumulative incidence rate was 4.28%.
Lung cancer occurred more often in men than in women. In men, the crude incidence rate was 61.86/100 000, whereas the CASIR and WASIR were 49.27/100 000 and 49.16/100 000, respectively. In women, the crude incidence rate was 29.54/100 000, whereas the CASIR and WASIR were 21.66/ 100 000 and 21.40/100 000, respectively. The crude incidence rate in urban areas was 52.52/100 000, which was higher than in rural areas (39.54/100 000). After age standardization, the incidence rate in urban areas (36.39/100 000 for WASIR) was still higher than in rural areas (33.25/100 000 for WASIR) (Table 1).
Table 1.
Lung cancer incidence in China, 2010
| Areas | Gender | No. of cases | Crude rate | Ratio | CASIR | WASIR | Cum rate | TASR | Rank |
|---|---|---|---|---|---|---|---|---|---|
| (1/105) | (%) | (1/105) | (1/105) | 0–74 (%) | 35–64 (1/105) | ||||
| ALL | Both | 605 946 | 46.08 | 19.59 | 35.23 | 35.04 | 4.28 | 50.61 | 1 |
| Male | 416 333 | 61.86 | 23.03 | 49.27 | 49.16 | 5.98 | 69.26 | 1 | |
| Female | 189 613 | 29.54 | 14.75 | 21.66 | 21.40 | 2.56 | 31.33 | 2 | |
| Urban | Both | 348 107 | 52.52 | 20.48 | 36.62 | 36.39 | 4.42 | 50.48 | 1 |
| Male | 238 816 | 70.39 | 24.48 | 51.22 | 51.05 | 6.15 | 68.80 | 1 | |
| Female | 109 291 | 33.78 | 15.10 | 22.52 | 22.24 | 2.63 | 31.36 | 2 | |
| Rural | Both | 257 839 | 39.54 | 18.50 | 33.39 | 33.25 | 4.10 | 50.74 | 1 |
| Male | 177 517 | 53.20 | 21.33 | 46.75 | 46.73 | 5.75 | 69.85 | 1 | |
| Female | 80 322 | 25.23 | 14.31 | 20.49 | 20.25 | 2.47 | 31.25 | 2 |
CASIR, age-standardized rates by Chinese population, 2000; TASR, truncated age-standardized rate (Segi's population); WASIR, age-standardized rates by world population (Segi's population).
In China, the 10 most common cancers in men accounted for 85.01% of all new cases. Lung cancer was the most common cancer diagnosed in men in China, accounting for 23.03% of all new cases, followed by stomach, liver, esophageal and colorectal cancers. In women, lung cancer was the second most frequently diagnosed cancer, after breast cancer, accounting for 16.20% of all new cases, and followed by colorectal, stomach, and liver cancers (Table 2).
Table 2.
The top 10 cancer incidence rates in China in 2010
| Male | Female | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Rank | Site | Cases | Incidence (1/105) | (%) | CASIR (1/105) | Site | Cases | Incidence (1/105) | (%) | CASIR (1/105) |
| 1 | Lung (C33-C34) | 416333 | 61.86 | 23.03 | 49.27 | Breast (C50) | 208192 | 32.43 | 16.20 | 25.89 |
| 2 | Stomach (C16) | 287844 | 42.77 | 15.92 | 34.05 | Lung (C33-C34) | 189613 | 29.54 | 14.75 | 21.66 |
| 3 | Liver (C22) | 268757 | 39.94 | 14.87 | 32.21 | Colorectal (C18-21) | 117486 | 18.30 | 9.14 | 13.63 |
| 4 | Esophagus (C15) | 204449 | 30.38 | 11.31 | 24.05 | Stomach (C16) | 116721 | 18.18 | 9.08 | 13.55 |
| 5 | Colorectal (C18-21) | 157355 | 23.38 | 8.70 | 18.75 | Liver( C22) | 90083 | 14.03 | 7.01 | 10.41 |
| 6 | Bladder (C67) | 46102 | 6.85 | 2.55 | 5.49 | Esophagus (C15) | 83183 | 12.96 | 6.47 | 9.46 |
| 7 | Pancreas (C25) | 40394 | 6.00 | 2.23 | 4.78 | Cervix (C53) | 76884 | 11.98 | 5.98 | 9.84 |
| 8 | Brain, CNS (C70-C72) | 39782 | 5.91 | 2.20 | 5.10 | Uterus (C54-55) | 47751 | 7.44 | 3.72 | 5.84 |
| 9 | Prostate (C61) | 38373 | 5.70 | 2.12 | 4.56 | Ovary (C56) | 41516 | 6.47 | 3.23 | 5.22 |
| 10 | Leukaemia (C91-C95) | 37523 | 5.58 | 2.08 | 5.10 | Thyroid (C73) | 41213 | 6.42 | 3.21 | 5.62 |
CASIR, age –standardized incidence rate (China population 2000); CNS, central nervous system.
Age-specific incidence rates of lung cancer for both genders and areas were compared. Lung cancer age-specific incidence rates were relatively low up to 45 years of age in each area, but then increased dramatically, peaking in the age groups of 80–84 or over 85 years old. Generally, lung cancer among men had a higher age-specific incidence rate than in women, except for those in younger age groups (<30 years old). Similarly, the age-specific lung cancer rates in urban areas were generally higher than in rural areas, except for subjects in younger age groups. The age-specific incidence rates varied in different areas with a similar curve (Fig 1). Lung cancer incidence rates were higher in urban areas than in rural areas.8 A unique age-specific incidence of lung cancer can be observed in Chinese women under 30 years of age.
Figure 1.
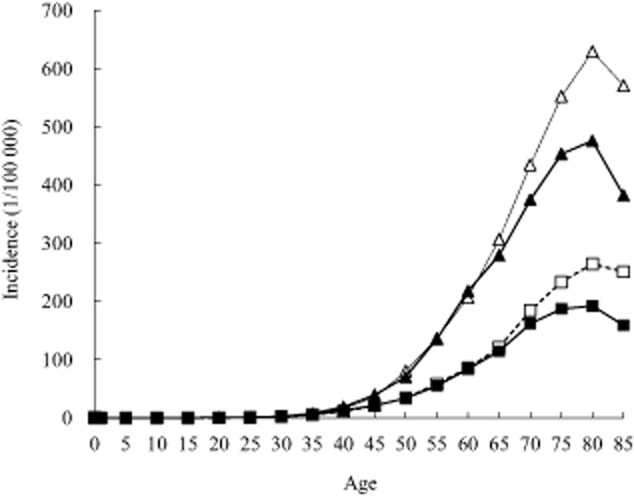
Age-specific incidence rate of lung cancer in China in 2010 (1/105).  , Urban male;
, Urban male;  , Urban female;
, Urban female;  , Rural male;
, Rural male;  , Rural female.
, Rural female.
Mortality
It is estimated that 486 555 people died of lung cancer in 2010 (336 786 men and 149 769 women), with a crude mortality rate of 37.00 per 100 000. The age-standardized rates by Chinese population (CASMR) were 27.93 per 100 000 and age-standardized rates by world population (WASMR) were 27.72 per 100 000. The cumulative rates of incidence and mortality from age 0 to 74 were 4.28% and 3.24%, respectively. Among 486 555 lung cancer deaths, 279 919 (57.53%) patients were from urban areas and 206 636 (42.47%) from rural areas.
In 2010, the mortality rates in urban areas (42.23/100 000) were higher than in rural areas (31.69/100 000), and slightly higher than ASR world rates (28.62/100 000 vs. 26.47/100 000).The mortality rate of lung cancer was much higher in men than in women. In men, the crude mortality rates, CASMR, and WASMR were 50.04/100 000, 39.79/100 000, and 39.62/100 000, respectively. In women, the crude mortality rates, CASMR, and WASMR were 23.33/100 000, 16.62/100 000, and 16.41/100 000, respectively. In urban areas, the crude mortality rates, CASMR, and WASMR were 42.23/100 000, 28.88/100 000, and 28.62/100 000, respectively. In rural areas, they were 31.69/100 000, 26.61/100 000, and 26.47/100 000, respectively, which were much lower than those in urban areas (Table 3).
Table 3.
Lung cancer mortality in China, 2010
| Crude rate | Ratio | CASIR | WASIR | Cum rate | TASR | ||||
|---|---|---|---|---|---|---|---|---|---|
| Areas | Gender | No. of cases | (1/105) | (%) | (1/105) | (1/105) | 0–74 (%) | 35–64 (1/105) | Rank |
| ALL | Both | 486 555 | 37.00 | 24.87 | 27.93 | 27.72 | 3.24 | 34.36 | 1 |
| Male | 336 786 | 50.04 | 26.85 | 39.79 | 39.62 | 4.59 | 48.49 | 1 | |
| Female | 149 769 | 23.33 | 21.32 | 16.62 | 16.41 | 1.86 | 19.75 | 1 | |
| Urban | Both | 279 919 | 42.23 | 27.05 | 28.88 | 28.62 | 3.32 | 33.10 | 1 |
| Male | 192 438 | 56.72 | 29.46 | 41.04 | 40.81 | 4.69 | 46.95 | 1 | |
| Female | 87 481 | 27.04 | 22.92 | 17.31 | 17.04 | 1.91 | 18.65 | 1 | |
| Rural | Both | 206 636 | 31.69 | 22.42 | 26.61 | 26.47 | 3.12 | 35.76 | 1 |
| Male | 144 348 | 43.26 | 24.02 | 38.09 | 38.00 | 4.45 | 50.19 | 1 | |
| Female | 62 288 | 19.56 | 19.42 | 15.64 | 15.50 | 1.81 | 21.02 | 1 |
CASIR, age-standardized rates by Chinese population, 2000; cum, cumulative; TASR, truncated age-standardized rate (Segi's population); WASIR, age-standardized rates by world population(Segi's population).
Because of the high mortality for lung cancer in each age group, the trend for lung cancer mortality in different age groups was similar to the trend of incidence. Age-specific mortality rates of lung cancer for both genders and areas were compared. The lung cancer age-specific mortality rates were relatively low up to 50 years of age in each area, but then increased dramatically, peaking in the age groups of 80–84 and over 85 years of age. Generally, lung cancer among men also had a higher age-specific mortality rate than among women, except for those in younger age groups (<40 years old) because of fluctuations of incidence in those age groups. Similarly, the age-specific mortality of lung cancer in urban areas was generally higher than in rural areas.8 The age-specific mortality rates varied in different areas with a similar curve (Fig 2).
Figure 2.
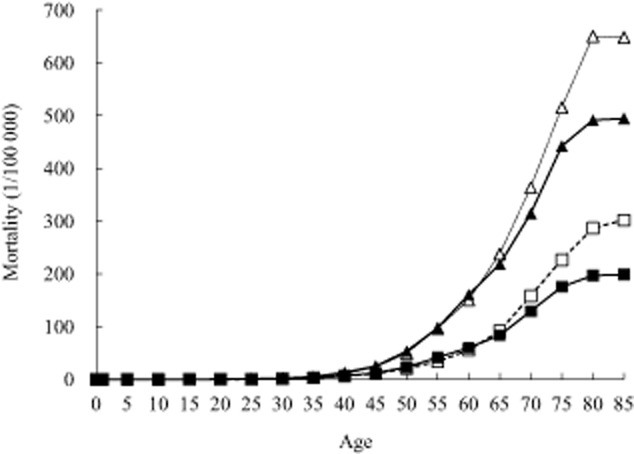
Age-specific mortality of lung cancer in China in 2010 (1/105).  , Urban male;
, Urban male;  , Urban female;
, Urban female;  , Rural male;
, Rural male;  , Rural female.
, Rural female.
In China, the 10 most common cancer deaths in men accounted for 89.35% of all deaths. Lung cancer was the most common cancer mortality in men, accounting for 23.33% of all deaths, followed by liver, stomach, esophageal, and colorectal cancers. Lung cancer was not the top cancer incidence in women in China, but the disease has become the leading cause of cancer death in women, accounting for 21.32% of all deaths with a high mortality compared with other cancers, followed by stomach, liver, esophageal and breast cancers (Table 4).
Table 4.
The top 10 cancer mortality rates in China in 2010
| Male | Male | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Rank | Site | Cases | Mortality (1/105) | (%) | ASR† (1/105) | Site | Cases | Mortality (1/105) | (%) | ASR† (1/105) |
| 1 | Lung (C33-C34) | 336786 | 50.04 | 26.85 | 39.79 | Lung (C33-C34) | 149769 | 23.33 | 21.32 | 16.62 |
| 2 | Liver (C22) | 231950 | 34.47 | 18.49 | 27.69 | Stomach (C16) | 87833 | 13.68 | 12.50 | 9.83 |
| 3 | Stomach (C16) | 200018 | 29.72 | 15.95 | 23.70 | Liver (C22) | 80482 | 12.54 | 11.46 | 9.15 |
| 4 | Esophagus (C15) | 148865 | 22.12 | 11.87 | 17.54 | Esophagus (C15) | 59608 | 9.29 | 8.49 | 6.52 |
| 5 | Colorectal (C18-21) | 76646 | 11.39 | 6.11 | 9.10 | Breast (C50) | 55500 | 8.65 | 7.90 | 6.56 |
| 6 | Pancreas (C25) | 34509 | 5.13 | 2.75 | 4.08 | Colorectal (C18-21) | 55464 | 8.64 | 7.90 | 6.12 |
| 7 | Leukaemia (C91-C95) | 26212 | 3.89 | 2.09 | 3.45 | Pancreas (C25) | 23226 | 3.62 | 3.31 | 2.58 |
| 8 | Brain, CNS (C70-C72) | 26029 | 3.87 | 2.08 | 3.27 | Cervix (C53) | 21626 | 3.37 | 3.08 | 2.60 |
| 9 | Lymphoma (C81-85,88,90,96) | 22178 | 3.30 | 1.77 | 2.70 | Brain, CNS (C70-C72) | 20711 | 3.23 | 2.95 | 2.55 |
| 10 | Bladder (C67) | 17386 | 2.58 | 1.39 | 2.05 | Leukaemia (C91-C95) | 19441 | 3.03 | 2.77 | 2.56 |
ASR, age –standardized incidence rate (China population 2000; CNS, central nervous system.
Trends over time
Lung cancer incidence and mortality has increased during the past decades in China, especially in rural areas.9,10 According to the statistics of the retrospective investigation of death by the National Office for Cancer Prevention and Control in the mid-1970s, the death rate for lung cancer in China was 5.47/100 000, accounting for 7.43% of the total cancer-related deaths and ranking fifth after gastric, esophageal, liver, and uterine cervix cancers, a lower ranking than in other countries at that time. The second sampling survey during the early 1990s revealed that the lung cancer death rate was 17.27/100 000, ranking third after gastric and esophageal cancers.
The 2006 third national retrospective investigation of mortality showed that cancer patterns in China have changed. Lung cancer has become the leading cause of cancer death with a mortality rate of 30.83/100 000, accounting for 22.69% of all cancer deaths, followed by liver, stomach and esophageal cancers(Table 5).
Table 5.
The top 10 cancer mortality rates in three National Retrospective Investigation of Death surveys
| 1973-75 | 1990-92 | 2004-05 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Mortality | CASMR | Mortality | CASMR | Mortality | CASMR | ||||
| Sites | (1/105) | (%) | (1/105) | (%) | (1/105) | (1/105) | (1/105) | (%) | (1/105) |
| ALL sites | 74.20 | 100.00 | 75.60 | 108.26 | 100.00 | 94.36 | 135.88 | 100.00 | 91.24 |
| Stomach | 17.40 | 23.45 | 17.70 | 25.16 | 23.24 | 21.76 | 24.71 | 18.19 | 17.86 |
| Esophagus | 16.70 | 22.51 | 17.10 | 17.38 | 16.05 | 15.02 | 15.21 | 11.19 | 9.97 |
| Liver | 10.75 | 14.49 | 11.00 | 20.37 | 18.82 | 17.83 | 26.26 | 19.33 | 17.86 |
| Cervix | 5.55 | 7.48 | 5.70 | 1.89 | 1.75 | 1.64 | 1.40 | 1.03 | 0.94 |
| Lung | 5.46 | 7.36 | 5.60 | 17.54 | 16.20 | 15.19 | 30.83 | 22.69 | 20.24 |
| Colorectal | 4.17 | 5.62 | 4.20 | 5.30 | 4.90 | 4.54 | 7.25 | 5.34 | 4.67 |
| Leukemia | 2.54 | 3.42 | 2.50 | 3.64 | 3.36 | 3.53 | 3.84 | 2.83 | 3.43 |
| Nasopharynx | 1.99 | 2.68 | 2.00 | 1.74 | 1.61 | 1.53 | 1.46 | 1.07 | 1.01 |
| Breast | 1.48 | 1.99 | 1.50 | 1.72 | 1.59 | 1.49 | 2.90 | 2.13 | 1.98 |
| Bladder | 0.51 | 0.69 | 0.50 | 1.01 | 0.93 | 0.85 | 1.41 | 1.04 | 0.85 |
CASMR, age-standardized rates by Chinese population.
According to data from 21 fixed cancer registries from 2000 to 2010 (NCCR), age-specific incidence of lung cancer has gradually changed. In men in urban areas, incidence increased only in the age group of 50–59 over the past decades, whereas in women in urban areas, incidence in the older age groups, such as 70 years of age, increased during the past decades. (Fig 3).
Figure 3.
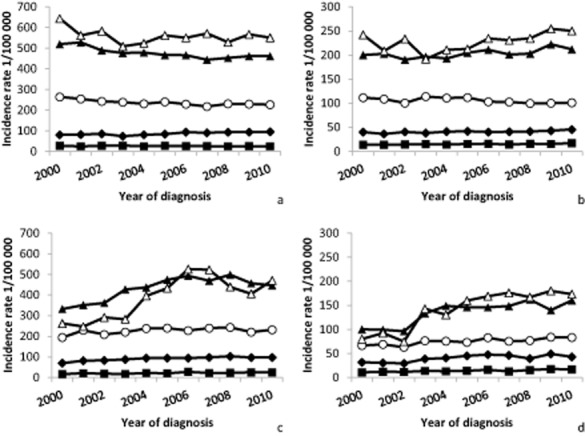
Age-specific incidence rates per 100 000 population, China, 2000–2010. (a) Urban male; (b) urban female; (c) rural male; (d) rural female.  , 40–49;
, 40–49;  , 50–59;
, 50–59;  , 60–69;
, 60–69;  , 70–79;
, 70–79;  , 80+.
, 80+.
The age-specific mortality trend of lung cancer changes similarly to the rate of incidence, with a slight decrease for each age group in urban areas, except in the female 80-year-old age group. The lung cancer mortality trend in rural areas did not obviously increase or decrease during the past decades, except in the 70-year-old age groups. (Fig 4)
Figure 4.
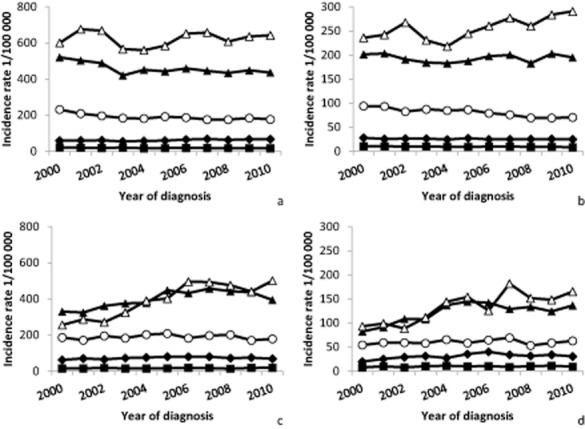
Age-specific mortality rates per 100 000 population, China, 2000–2010.  , 40–49;
, 40–49;  , 50–59;
, 50–59;  , 60–69;
, 60–69;  , 70–79;
, 70–79;  , 80+.
, 80+.
Predictions
The technical aspects of analyzing and predicting the cancer burden have been developed and refined over the past few decades. Different mathematical models, such as age, age-period, and age-period-cohort (APC) models have widely been used to describe disease trends in populations. Estimates of the future number of lung cancer patients can assist the Department of Health to plan the best possible allocation of finite resources to the core elements of cancer control: primary prevention, screening and early diagnosis, treatment, rehabilitation, and palliative care.11
The most important risk behaviour for lung cancer is tobacco smoking. The relationship between smoking and lung cancer is one of the most thoroughly investigated issues in biomedical research, and compelling evidence has built up since the middle of the 20th century to indicate that smoking is the predominant causal factor for lung cancer.12 According to GLOBOCAN 2012, 733 280 lung cancer patients in 2015 and 845 133 lung cancer patients in 2020 are predicted,7 a higher prediction of lung cancer cases than previous estimates.13 Lung cancer will increase in the future in China.
Discussion
A population-based cancer registry system plays a very important role in collecting and providing cancer statistics for cancer control and prevention. In China, the first population-based cancer registry was established in 1958 in Linzhou, Henan province.14 However, the development of cancer registration was limited at this time and little improvement was seen for several decades. The NCCR of China was established in 2002, acting as a federal bureau for systematic management of cancer surveillance nationwide. The NCCR of China is responsible for cancer data collection, evaluation, analysis, and publication from population-based cancer registries located in each province. All hospitals, community health centers, and other medical institutions with cancer diagnostic capabilities record and report new cancer cases to the cancer registry when a case is first diagnosed, including details from township medical insurance and the New Rural Cooperative Medical System. The death record database is linked to the cancer registration database for identifying vital statistics and also identifying cases not included in the registry (which can then be added to the cancer registry). The documentation of cancer cases throughout China was limited in the 20th century because of a lack of reliable cancer registries in different regions; only 11 cancer registries were established in China until 1998. Because of an increasing demand for cancer information and an emphasis on effective cancer prevention and control, the Health Ministry established the NCCR in 2002.15 By 2014, the number of cancer registries had increased to 308, distributed in each province and covering approximately 300 million or 22% of the national population. The NCCR now adequately reflects the general population of China.
Lung cancer has been the leading cause of cancer mortality in China for many years, and its incidence is growing throughout the world. The high morbidity and mortality of lung cancer largely results from the fact that most people are diagnosed at advanced disease stage. Although many risk factors have been implicated, such as tobacco exposure, air pollution has also been determined to have a significant impact in the development of lung cancer. Tobacco use is currently increasing among specific population groups. It is probable that lung cancer will continue to be a major medical and social problem for the foreseeable future. Lung cancer incidence and mortality trends closely reflect patterns in smoking prevalence from 20 to 30 years earlier. In more developed countries, incidence and mortality rates are generally declining among men and are starting to plateau for women, reflecting previous trends in smoking prevalence. In contrast, there are some populations in less developed countries where increasing lung cancer rates are predicted to continue as a result of the endemic use of tobacco.12 Tobacco use is the most preventable cause of cancer death, accounting for 20% of cancer deaths worldwide and for about 6% of cancer deaths in Africa.16 In women, the incidence rates are generally lower and the geographical pattern is a little different, mainly reflecting different historical exposure to tobacco smoking.17,18 However, in China, about 52.4% of lung cancer can be attributed to smoking in men, and about 19.4% in women.19 Risk factors, such as indoor air pollution and indoor radon9,20 also play a role in the development of lung cancer in women in China. Many differences in lung cancer have been identified in China compared with developed countries, such as later stage distribution. An improvement in the health care system in China would help to optimise care for people with lung cancer.
Conclusion
The age-specific incidence trend found in this study is contradictory to the crude incidence trend of lung cancer shown in a previous study,2 which reported that age-specific incidence rate changes were stabilizing or even slightly decreasing; however, the crude incidence rate has continuously increased over the past decade in both men and women in urban and rural areas of China. The predicted increase in lung cancer and the trend of lung cancer during the past decades can be explained by the aging population in China. Tobacco consumption, air pollution, unhealthy lifestyles, and other risk factors for exposure would be reflected in future data if we did nothing for disease control. This article has described the epidemic of lung cancer in China and because of a lack of effective treatment for advanced lung cancers, these results highlight the need for ongoing prevention and control strategies to reduce the burden of lung cancer.
Disclosure
No authors report any conflict of interest.
References
- Chen Z. The 3rd National Death Cause Survey Report. Beijing: Chinese Academy of Medical Sciences & Peking Union Medical College Press; 2008. [Google Scholar]
- Chen W, Zhang S, Zou X. Evaluation on the incidence, mortality and tendency of lung cancer in China. Thorac Cancer. 2010;1:35–40. doi: 10.1111/j.1759-7714.2010.00011.x. [DOI] [PubMed] [Google Scholar]
- Kabir Z, Bennett K, Clancy L. Lung cancer and urban air-pollution in Dublin: a temporal association? Ir Med J. 2007;100:367–369. [PubMed] [Google Scholar]
- Loomis D, Grosse Y, Lauby-Secretan B, et al. The carcinogenicity of outdoor air pollution. Lancet Oncol. 2013;14:1262–1263. doi: 10.1016/s1470-2045(13)70487-x. [DOI] [PubMed] [Google Scholar]
- Moolgavkar SH, Holford TR, Levy DT, et al. Impact of reduced tobacco smoking on lung cancer mortality in the United States during 1975–2000. J Natl Cancer Inst. 2012;104:541–548. doi: 10.1093/jnci/djs136. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pesch B, Kendzia B, Gustavsson P, et al. Cigarette smoking and lung cancer—relative risk estimates for the major histological types from a pooled analysis of case–control studies. Int J Cancer. 2012;131:1210–1219. doi: 10.1002/ijc.27339. [DOI] [PMC free article] [PubMed] [Google Scholar]
- International Agency for Research on Cancer. 2013. GLOBOCAN 2012: estimated cancer incidence, mortality and prevalence worldwide in 2012 [Cited 12 Dec 2013.] Available from URL: http://globocan.iarc.fr/Default.aspx.
- Chen W, Zheng R, Zhang S, et al. Annual report in status of cancer in China, 2010. China J Cancer Res. 2014;26(1):48–58. doi: 10.3978/j.issn.1000-9604.2014.01.08. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mumford JL, He XZ, Chapman RS, et al. Lung cancer and indoor air pollution in Xuan Wei, China. Science. 1987;235:217–220. doi: 10.1126/science.3798109. [DOI] [PubMed] [Google Scholar]
- Han R, Zheng R, Zhang S, Wu M, Chen W. [Trend analyses on the differences of lung cancer incidence between gender, area and average age in China during 1989–2008. Zhongguo Fei Ai Za Zhi. 2013;16:445–451. doi: 10.3779/j.issn.1009-3419.2013.09.02. (In Chinese.) [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bray F, Moller B. Predicting the future burden of cancer. Nat Rev Cancer. 2006;6:63–74. doi: 10.1038/nrc1781. [DOI] [PubMed] [Google Scholar]
- Youlden DR, Cramb SM, Baade PD. The International Epidemiology of Lung Cancer: geographical distribution and secular trends. J Thorac Oncol. 2008;3:819–831. doi: 10.1097/JTO.0b013e31818020eb. [DOI] [PubMed] [Google Scholar]
- Chen WQ, Zheng RS, Zeng HM. Bayesian age-period-cohort prediction of lung cancer incidence in China. Thorac Cancer. 2011;2:149–155. doi: 10.1111/j.1759-7714.2011.00062.x. [DOI] [PubMed] [Google Scholar]
- Zhang S, Cheng W, Wang L. The 30 years of cancer registration in China. China Cancer. 2009;18:256–259. (In Chinese.) [Google Scholar]
- Cancer Registry List of International Agency for Research on Cancer. [Cited 19 Sep 2014.] Available from URL: http://ci5.iarc.fr/Default.aspx.
- de Martel C, Ferlay J, Franceschi S, et al. Global burden of cancers attributable to infections in 2008: a review and synthetic analysis. Lancet Oncol. 2012;13:607–615. doi: 10.1016/S1470-2045(12)70137-7. [DOI] [PubMed] [Google Scholar]
- Parkin DM. International variation. Oncogene. 2004;23:6329–6340. doi: 10.1038/sj.onc.1207726. [DOI] [PubMed] [Google Scholar]
- Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics, 2002. CA Cancer J Clin. 2005;55:74–108. doi: 10.3322/canjclin.55.2.74. [DOI] [PubMed] [Google Scholar]
- Liu BQ, Peto R, Chen ZM, et al. Emerging tobacco hazards in China: 1. Retrospective proportional mortality study of one million deaths. BMJ. 1998;317(7170):1411–1422. doi: 10.1136/bmj.317.7170.1411. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Blot WJ, Xu ZY, Boice JD, Jr, et al. Indoor radon and lung cancer in China. J Natl Cancer Inst. 1990;82:1025–1030. doi: 10.1093/jnci/82.12.1025. [DOI] [PubMed] [Google Scholar]