

Abstract
Unfortunately, the prevalence of cesarean section has increased in recent years. Whereas awareness of the prevalence and causes is inevitable for planning and effective interventions, so aim of this study has designed and conducted for reviewing of systematic Prevalence and caesarean causes in Iran. In this meta-analysis, the required information have been collected using several keywords which are Cesarean section rate, Cesarean section prevalence, delivery, childhood, childbirth, relative causes, relative frequency, Iran and their Persian equivalents have been collected from databases such as CINAHL, Science Direct, PubMed, Magiran, SID, Iranmedex. Finally, we found 706 related articles and selected 34 articles among them for studying of cesarean Prevalence. We used CMA software with random model for Meta-Analysis. The prevalence of Cesarean was estimated48%. Using content analysis, Factors influencing the incidence of cesarean section were divided to 3 categories including social and demographic factors, obstetric-medical causes and non-obstetric-medical causes. Maternal education and grand multiparity in the field of demographic and social factors, previous cesarean in the field of obstetric-medical causes and fear of normal-vaginal delivery (NVD) and doctor’s suggestion in the field of non-obstetric-medical causes were major causes of Cesarean. According to the high prevalence of caesarean section and it upward development, it seems to be essential designing and implementing of programs and interventions effectiveness including providing of Possibility of painless childbirth and education and psychological interventions, increasing of quality of natural delivery services, proper culture and prohibiting of doctors from Personal opinions and profit.
Keywords: Incidence, Caesarean, Causes, Iran, Meta-Analysis
Introduction
Childbirth this one of the blessings of God to save the human race on Earth and it has been continued since human immersion up to now. Delivery mechanism is a spontaneous process without need for intervention(1–3) where the action takes place in both natural and caesarean (4). Vaginal delivery is known as the best but unfortunately because of development of caesar-ean section, the prevalence of vaginal delivery is declined in recent years (5).
However, based on recent studies, the rate of caesarean section is increasing in the world, so this rate is about 22%, 25%, 27% in USA, Brazil, and Chili respectively and also is about 17-40% in 19 countries in Latin America (6, 7). Based on proposing of The World Health Organization, Incidence of cesarean section should not exceed 15% of total deliveries (8). Unfortunately, based on the results of different studies, the rates of caesarean is very high in Iran (9–11) and according to the Statistics, this rate was reported 26% up to 60% in comparison with some private institute which was reported up to 87%. According to statistics published in 1355, Caesarean section incidence was19.5%in comparison with year 1385 which was 42.3% (10).
Lack of knowledge of cesarean section and misinformation about natural childbirth is important factors for cesarean section (12–14). On the other hand, maternal satisfaction from the previous childbirth experience has tremendous impact on the type of delivery which is based on maternal deciding (15). Also, the results of the studies showed that fear, anxiety and pain have important role in the choice of delivery type (16). Many studies have been conducted in the context of the prevalence and causes of cesarean in Iran. But, these studies have been done in a particular geographical area. Hence, there is need to summarize and provide a clear and complete plane of the prevalence and different causes in different regions of Iran, so that the results of these studies can be used to design and implement appropriate Planning and interventions.
The aim of this study was collecting and reporting of prevalence and effective factors in the tendency of women to cesarean based on studies which have been conducted in Iran.
Methods
In this meta-analysis, the required information have been collected using several keywords which are Cesarean section rate, Cesarean section prevalence, delivery, childhood, childbirth, relative causes, relative frequency, Iran and their Persian equivalents have been collected from databases such as CINAHL, Science Direct, PubMed, Magiran, SID, Iranmedex. Finally, we found 706 related articles and selected 34 articles among them for studying of cesarean Prevalence. We used CMA software with random model for Meta-Analysis. Published articles have been studied in Persian and English languages. A literature search was conducted from 2000 to 2012. This period of time was selected due to control and decreases the time-passing effects on the rate and causes of cesarean section prevalence. Because of time-passing effects, it is possible that rate and causes of cesarean section prevalence has been changed for different reasons including medical advances, awareness change, women’s attitudes and many other factors, so selecting this period of time, effect of these changing has been decreased and prevalence and causes Prevalence and causes would be more realistic. Articles which are mentioned to one of the objects of this study (prevalence and causes) at least and published articles in both Persian and English languages. The search strategy also included hand searching of journals, gray literature, and references of included articles. Existing criteria from study were included letters to the editor, case reports, papers presented in seminars and conferences and articles which are resulted from interventions. After articles extraction from the database using mentioned keywords to assess the quality of articles, these articles were evaluated by two assessors using the descriptive and analytical studies checklist (STROBE). Two investigators evaluated all articles to achieved agreement. When agreement was unattainable between evaluators, consensus was achieved through third party investigator. Finally, among the 706 articles, 34 related articles were entered into the study after removing some articles which were poor-related with study object including existing criteria (Fig. 1). Selected articles have been studied completely and required information in the systematic review has been summarized by extraction table using Excel software. Endnote X5 software is used for organizing and studying of subjects and also identification of repetitive cases. CMA (Comprehensive Meta-Analysis) software is used for Calculating and estimating of cesarean Incidence and performing Meta-Analysis. Forest plots are used for reporting the results as the size of each square represents the sample size and the lines drawn on each side of the square represent95% confidence interval for the incidence of cesarean in each study. I2 test was used to measure heterogeneity and funnel plot to measure publication biases.
Fig. 1:

Literature review and retrieval flow diagram
Results
After eliminating irrelevant and repeated articles, finally 34 completely related articles related to the objectives of research were investigated (Appendix 1). Thirty items of these articles were analytical-descriptive, 3 items were qualitative from results of which we use just in determining influencing factors section. One of these studies had been carried out in case-subjective method. Among 31 descriptive-analytical and case-subjective articles, totally, we studied 74809 deliveries. Among this number, 35908 cases (48%) were carried out in caesarean method and 38901 cases (52%) were carried out in Normal Vaginal Delivery (NVD) method. The main tools and sources of data gathering were hospital profiles and questioners which were filled through interview. In this investigation, researchers investigated the prevalence in three groups of pregnant mothers with heavy, natural and lower weight. Prevalence was different in each three groups which are related to each three group’s average
Appendix 1:
Summary of results of investigating on conducted researches
| references | Sample size | Prevalence (%) | Causes |
|---|---|---|---|
| (3) | 100 | 34 | High education, cesarean background, increasing the age of mother, doctor’s recommendation (11.76%), low pain (55.89%), friends’ recommendation (8.82%), the less side effect for mother (8.82%), the less side effect for infant (5.88%), tendency to tube ligation (8.82%) |
| (18) | 1473 | 45.6 | Private hospital, high education, high educational and social class, employee, living in city, having surgery background |
| (20) | 500 | 43 | Fearing vaginal delivery pain (37.2%), doctor’s recommendation (35.8%), concerning about infant health (11.5%), concerning about mother’s fitness (6.5%), associated disease (5%), high education, having job |
| (24) | 824 | 66.5 | Mother requesting (22%), doctor’s recommendation (22%), repeated cesarean (73.5%), twinning (7%), fetal displacement (6%), other (13.5%) |
| (25) | 824 | 66.5 | The repeated midwife-medical-cesarean factors (73.5%), multiple twines (7%), fetal displacement (6%), other (13.5%) (fearing of vaginal delivery pain, doctor’s recommendation, high education, previous cesarean, caring at the private hospital) |
| (27) | 342 | - | The lower pain (60%), infant’s health (27.1%), mother’s health (10%), friends’ opinion (2.3%), the low expenditure (0.6%) |
| (28) | 396 | 58.6 | Undeveloped delivery (18.1%), doctor’s recommendation (15.1%), fearing vaginal delivery pain (11.2%), mother requesting (11.2%) |
| (33) | 7649 | 32.92 | Previous cesarean (25.1%), fetal distress (22.16%), optional or selected cesarean (11.6%), non-cephalicpresentation (11.44%), mother’s disease (10.52%), cephalopelvic disproportion (8.26%), undeveloped delivery (8.07%), twinning (2.86%) |
| (33) | 3596 | 26.06 | Repeated cesarean (23.69%), optional or selected cesarean (13.67%), cephalopelvic disproportion (13.56%), fetal distress (13.45%), non-cephalic presentation (11.63%), undeveloped delivery (10.03%), twinning (3.63%) |
| (35) | 1737 | 45.4 | Undeveloped delivery (8.7%), delivery distress (22.3%), CPD and Macrosomia (22.2%), previous cesarean (22.7%), presentation (8.4%), other (15.7%) |
| (36) | 5238 | 44 | Previous cesarean (43.4%), pelvic stricture (20%), hazardous childbirth (7.7%), presentation (6%), tendency to tube ligation (5%), other (26.9%) |
| (38) | 473 | 25.4 | Having better job, high education, living in city, lowering family members, high birth weight (more than 3900 gram), enlargement of Head circumference, high weight and age of mother |
| (39) | 250 | 28.4 | Doctor’s recommendation, fearing vaginal delivery pain, previous cesarean, the care given by private doctor |
| (40) | 210 | - | Infant health, fearing vaginal delivery pain (51.55%), mother’s health (57.15%), fetal’s health (82.9%), friends’ recommendation (27.94%), tube ligation (16.2%), other (30.5%) |
| (41) | 256 | 31.25 | Fearing vaginal delivery pain (52.5%), tube ligation (17.5%), fearing the infant’s harm (6.2%), fearing the female reproductive system harm (8.8%), mother’s health (3.8%), tendency of wife and families (3.8%), living in city (5%)/* The rate of awareness (56%) |
| (42) | 11 | - | Fearing vaginal delivery pain, the bad experience from previous cesarean |
| (43) | 400 | - | Fear of vaginal delivery (NVD) pain |
| (44) | 1221 | 42.1 | Previous cesarean (25.7%), tendency to tube ligation (9.1%), cephaloofpelvic disproportion (8%), decreasing of amniotic fluid (7.6%), abnormal appearance (6.8%), other (42.8%) |
| (45) | 294 | 16.2 | Obesity |
| (46) | 500 | 37.6 | The rate of previous cesarean, the rate of visits before delivery, fetal displacement, meeting midwife, pelvic stricture, tube ligation after delivery, mother suggestion for cesarean, the age of marriage |
| (47) | 3210 | 32.2 | Previous cesarean (34.9%), fetal distress (20.2%), undeveloped delivery steps (11.1%), fetal displacement (10.7%), other (23.1%) |
| (48) | 26 | - | Fearing unknown things, low pain, unsuccessful experience, other’s encouraging, concerning about side effects, inappropriate relationship of treatment team, feeling the death and being solitude, infant’s health |
| (49) | 16170 | 27 | Undeveloped delivery (25.3%), cesarean background (25%), fetal distress (20.9%), inappropriate presentation (8.86%), twinning (1.2%), mother’s systematic disease (1.8%), cesarean for tube ligation (0.88%) |
| (50) | 609 | 47.25 | Previous cesarean (29.7%), optional or selected cesarean (10.2%), fetal distress (8.3%), undeveloped delivery (7.1%), cephalopelvic disproportion (6.8%), abnormal appearance (6%), other (31.9%) |
| (51) | 195 | 63.4 | Medical-midwifery: previous cesarean (32.3%), pelvic stricture (11.3%), undeveloped delivery (8.9%), other (47.5%) Non-medical factors: doctor’s persistence (50%), previous cesarean (25%), personal belief (4.9%), mother’s persistence (4.9%), other (15.2%) |
| (52) | 459 | 43.9 | High educational and social class |
| (53) | 24241 | 45.2 | Previous cesarean (43%), fetal distress (12.8%), undeveloped delivery (11.6%), midwifery factors (9.1%), fetal displacement (6.3%), other (17.2%) |
| (54) | 346 | 50.2 | Doctor’s opinion (49.4%), low pain (36%), infant’s health (27.6%), awareness of delivery time (23%), husband suggestion (11.5%), other (24.1%) |
| (55) | 187 | 49.8 | Low pain (55%), fearing the female reproductive system’s harm (23%), concerning about infant’s health (17%), medical conditions (3%), the bad experience from previous cesarean (2%) |
| (56) | 210 | 51.7 | High education, recommendation of husband and his family, recommendation of mother and wife’s family |
| (57) | 1500 | 40.3 | High age and education, higher rate of Gestations, previous delivery background, live infant, increasing rate of abortion |
| (58) | 300 | 58 | Cesarean experience, age and type of the hospital, fearing vaginal delivery pain |
| (59) | 703 | - | Fetal distress (30.8%), repeated cesarean (19.4%), cephalopelvic disproportion (15.9%), delivery stop (14.9%), other (19%) |
The minimum amount of prevalence of caesarean equaling 16.2% was observed in Bam and maximum amount (66.5%) observed in Tehran. Finally, caesarean prevalence was estimated 48%.
Putting aside qualitative studies and studies having weaknesses of methodological and administration point of view, from 34 entered articles to this study, 25 articles entered into Meta-analysis. In this study, considering Cochran’s Q test result which indicates heterogeneity among different studies results, we used a model with random effect in meta-analysis. Figure 2 indicates caesarean prevalence with 95% confidence interval of total studies in different parts of country.
Fig. 2:
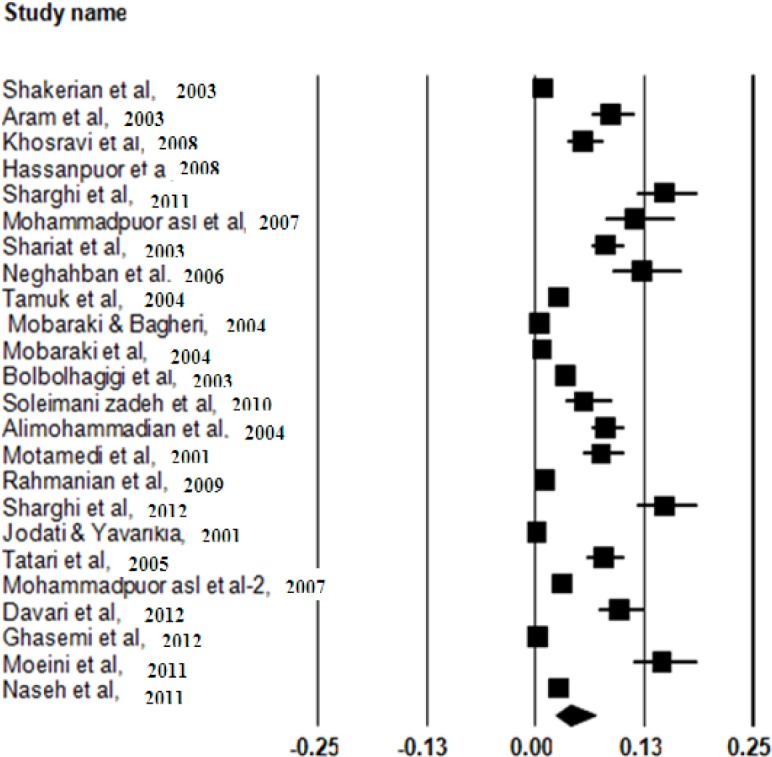
Caesarean section prevalence in Iran with confidence interval of 95% (Based on random model)
The prevalence of Caesarean section based on the random effect was determined to be 48% (95% CI, lowest = 26%, highest = 88%).
95% CI for the prevalence was drawn for each study in the horizontal line format (Q value= 2303.43, df=24 I2=98.9 P-value<0.001).
Funnel plot of caesarean section show that there are not symmetry in data. That indicates some study which has lower prevalence and high standard error not be published (Fig. 3).
Fig. 3:
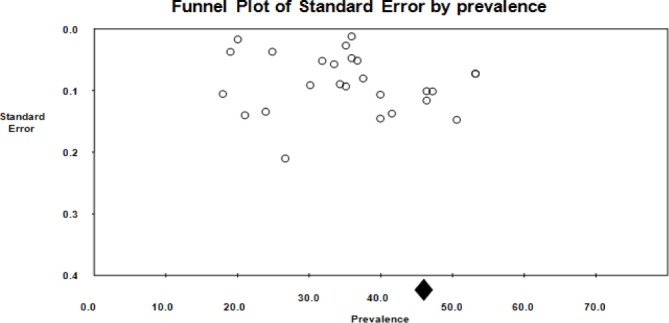
Funnel plot of caesarean section in Iran
Using content analysis, the influencing reasons of caesarean section were divided into three categories of 1-demographical and social elements, 2-midwifery and clinical elements and 3-non-clinical non-midwifery elements. Among these factors individual and her behavior are most important. Using repetition frequency in studies or mentioned mean of all percentages in studies, the effect of each element was provided in Fig. 4-7 respectively. As it can be seen in Fig. 4, the higher education and higher pregnancy age with 7 times of repetition was considered as the main influencing social and demographical factors of caesarean section prevalence in investigated articles, significantly. Delivery or receiving clinical cares in pregnancy period from hospital or private doctor were other influencing factors of caesarean prevalence among articles. Another grouping model of reasons in this study was clinical-midwifery group which was mainly related embryo and mother clinical condition. These have been mentioned in Fig. 5. As it can be observed in Fig. 5, previous caesarean section experience (with 36.29% average) and fetal distress (with 18.86% average) are the major reasons of clinical-midwifery caesarean section. Among studied reasons of this research, mother background disease and multiple breeding with 7.7% and 4.22% are the least influencing factors of caesarean section. The third and the last grouping of influencing factors of caesarean prevalence is related to the factors other than factors mentioned to the previous groups which is known as “non-clinical and non-midwifery” reasons. This is mostly related to individual behaviors and comprehensions. The average of each item has been provided in Fig. 6. As it can be seen in Fig. 6, fearing from NVD pain (with average of 39.33%) and doctor advice (with average of 28.45) are the main non-behavioral or non-midwifery-clinical reasons of cesarean section prevalence.
Fig. 4:
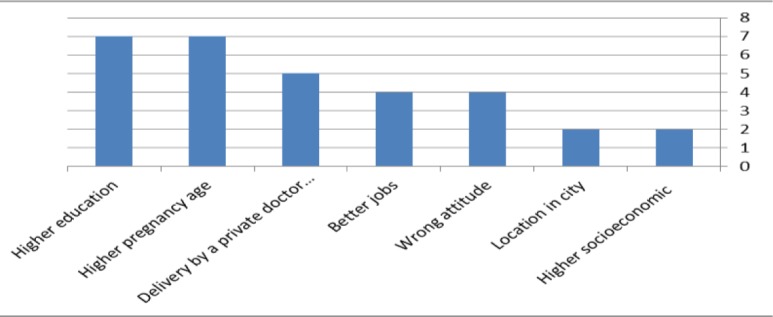
influencing social and demographic reasons frequency on caesarean operation prevalence based on significant items in investigated articles.
Fig. 7:
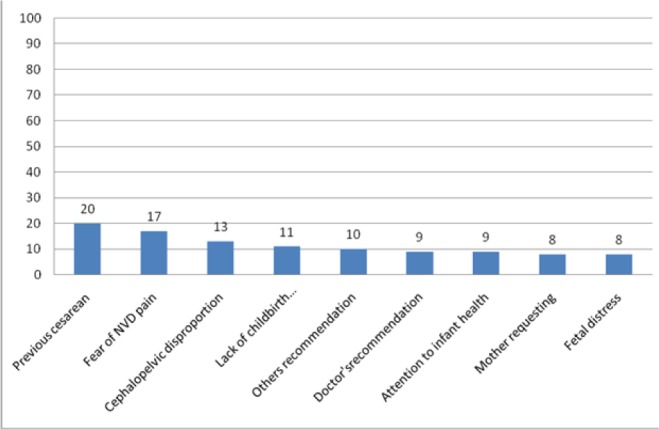
Frequency of medical and nonmedical factors affecting the incidence of repeat caesarean section according to the repeated studies
Fig. 5:
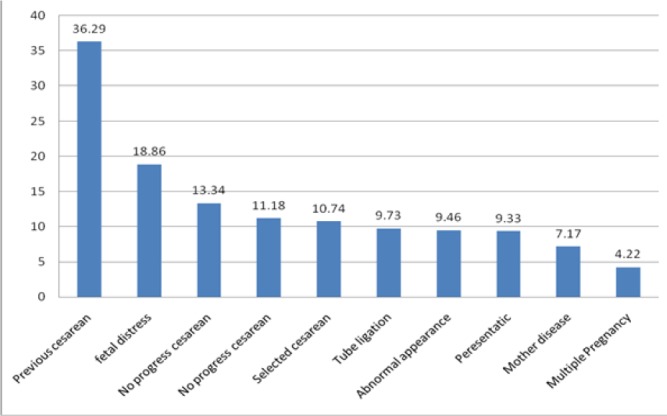
Frequency of Midwifery-Medicine causes impact on Incidence of cesarean
Fig. 6:
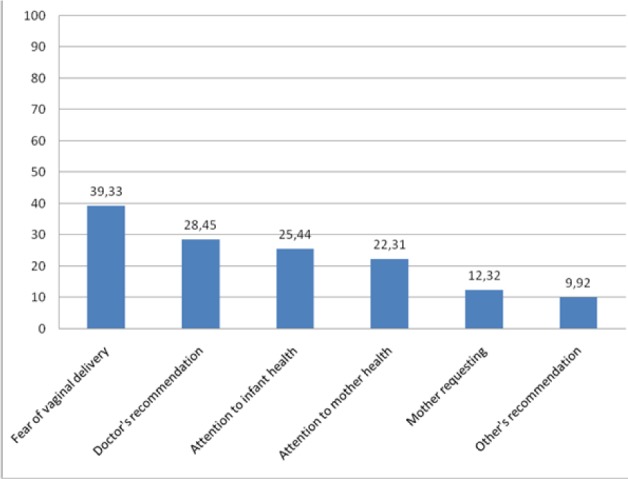
Frequency of non-Midwifery-Medicine causes impact on Incidence of cesarean
Relatives’ recommendation (with 9.92%) has the least effect among elements studied in this research.
The clinical-midwifery and non-clinical-midwifery frequency based on repetition frequency in studied articles of this research can be seen in figure 7 indicating the most repetition of previous caesar-ean section experience and fearing from NVD pain among studied influencing factors.
As it can be seen in Fig. 7, history of caesarean section (20 times) is the main clinical and non-clinical reason for deciding to caesarean section.
Discussion
Results obtained from this study indicated that general prevalence of caesarean section in carried out studies was 48%. Higher education and grand multiparity and doing caesarean section or receiving clinical cares in pregnancy period from hospital or private doctors were the main influencing social and demographical factors of caesarean section prevalence. Previous caesarean section experience and fetal distress are the major reasons of clinical-midwifery caesarean section. Fearing from NVD pain and doctor advice are the main non-behavioral or non-midwifery-clinical reasons of caesarean section prevalence. Change procedure investigation of caesarean prevalence among studied years, indicated a significant increase of caesarean amount in carried out studies.
General prevalence of cesarean, in carried out studies increased during recent years (17). Accordingly, an investigation carried out in England, indicated that caesarean section prevalence had an increasing procedure in recent years. Caesarean section prevalence was reported 26% to 60% and even 90% in some Iranian private centers (18, 19). Other studies have reported different prevalence of caesarean section in Iran (20–23). The main reason for different caesarean section prevalence in different areas of Iran can be resulted from different cultures in different areas. Since culture can affect caesarean selection through attitudes and ideas. Unequal distribution and scattering of hospitals, private clinics, and other centers and facilities in different cities and areas of country can influence this issue greatly.
Results of studied articles in this research showed that caesarean section among higher education women is more than women having lower education. Results from other studies (7) (24), indicated that with an increase in mother education level, there is more tendencies to do caesarean section. The reason for this issue can result from something more than increasing knowledge, as a preferred item, that the degree of pain is lower in caesarean section socially is more luxurious than NVD. Moreover obtained results indicated that caesarean amount in private and non-governmental clinics and taking clinical cares during pregnancy period by private personal doctor. Eighty four percent of items cared by personal doctors resulted in caesarean section, while this amount equals 47% in non-governmental centers indicating higher amount of caesarean section in items cared by hospital and personal doctors (25). In this study, mother employment has less effect on choosing caesarean section compared to other demographical variables. These findings are similar to other studies (26–28). This might be due to Iranian culture in which proving family expenses is less up to mothers and women. Moreover, tendency toward caesarean section among women whit high income and wealthy families is higher than those poor families and women. This finding is in accordance with other studies (8, 29).
According to results obtained from this study, doctor recommendation is one of the main reasons for caesarean section. This was applying in carried out studies indicating the key role of doctors and health care personnel on caesarean section. In 70% of cases, the doctor plays the main role in Caesarean section (30). Moreover in Italy, therapeutic doctor of pregnant mother plays the main role in selecting delivery system type (31). Other researchers accepted that doctor decision about delivery type is more influence than delivery conditions. The reason of increase in caesarean section, percent among mothers having no indication for this operation was doctor’s decision and tendency (32). This might be due to higher costs of caesarean section compared to NVD in hospi tals and private clinics, leading doctor unintentionally toward this kind of delivery.
In these studies previous caesarean section was mentioned as the main clinical-midwifery reason in choosing caesarean section delivery which applies to the results of most other studies carried out in this field (33–37). Taking this into consideration that, recently, number of children has been reduced in families it can be expected that the majority of previous caesareans can be in nulliparous. This can be natural, considering having no previous experience of delivery, fear, individual personalities and other reasons near nulliparous. Hence planning and effective interference with nulliparous should be carried out with higher sensitivity and severity and providing needed trainings and knowledge should start from initial periods of pregnancy.
The study was also limited by the fact that it only included articles in English and Farsi (Persian) and limited access to some of databases was another limitation of this study.
Conclusion
Considering drastic prevalence of caesarean in our country and its upward procedure on one hand, and its side effects on mothers, infants, treatment-health system and generally social health, health system managers, planners and other qualified members of this field, should design and administrate effective interferes and plans in reducing caesarean amount and promoting NVD. Considering the key reasons for caesarean prevalence including: previous caesarean, fear of pain in NVD and doctors recommendation, Providing psychological interventions and education, Increase the quality of vaginal delivery services, appropriate culture, providing solutions and legislation which are preventing doctors from personal opinions can be an effective strategy.
Ethical considerations
Ethical issues (Including plagiarism, Informed Consent, misconduct, data fabrication and/or falsification, double publication and/or submission, redundancy, etc) have been completely observed by the authors.
Acknowledgements
The authors declare that there is no conflict of interests.
References
- Sharifirad GH, Fathi Z, Tirani M, Mehaki B (2007). Assessing of pregnant women toward vaginal delivery and cesarean section based on behavioral intention model. Ilam Uni of Med Sci J, 15(1): 19–23 [in Persian]. [Google Scholar]
- Tabrizi JS, Gholipoor K, Asghari jafarabadi M, Farahbakhsh M, Mohammadzedeh M (2012). Customer quality and maternity care in Tabriz urban health centers and health posts. J Clin Res Gov, 1(2): 12–15. [Google Scholar]
- Hoshmandi S, Dolatian M, Kamalifard M, Ghojazadeh M (2012). Comparison of Labor Pain and Factors Affecting the Pain Perception among Primiparous and Multiparous Women Referring to Women's Private and state Hospitals in Tabriz in 2010. Tabriz Uni of Med Sci J, 34(3): 117–121 [in Persian]. [Google Scholar]
- Cunningham F, Leveno K, Bloom S, Fauser J, Zwirner M (2005). Williams Obstetrics. New York: Graw-Hill [Google Scholar]
- Clark SC, Taffeles S (1997). Cesarean rate decreasing. Obstet Gynecol New, 31: 10. [Google Scholar]
- Hopkins K (2000). Are Brazilian women really choosing to deliver by Cesarean? So Sci and Med, 51(5): 725–740. [DOI] [PubMed] [Google Scholar]
- Murray S (2000). Relation between private health insurance and high rates of caesarean section in Chile: qualitative and quantitative study. BMJ, 321(7275): 1501–1505. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mohammaditabar S, Kiani A, Heydari M (2009). The survey on tendencies of Primiparous women for selecting the mode of delivery. Babol Uni of Med Sci J, 11(50): 54–59 [in Persian]. [Google Scholar]
- Torkzahrani S (2008). Commentary: childbirth education in Iran. J Perinat Educ, 17(3): 51–54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- shareferad G, fathean Z, Terane M, Mahake B (2007). The Survey of pregnant women views about delivery and cesarian According Behavioral intention model. Elam Uni Med Sci J, 15(1): 19–23 [in Persian]. [Google Scholar]
- Bani S, Seyed Rasouli A, Shams Ghorashi T, Ghojazadeh M, Hassan pour S (2010). Delivery Agents Preferences Regarding Mode of Delivery for Themselves and Pregnant Women (Obstetrics, Gynecologists, Midwives). J of Nurs and Midwi, 18(5): 40–48 [in Persian]. [Google Scholar]
- Cunningham F (2005). Williams Obstetrics: Golban Publications. [Google Scholar]
- Arjmandi B, Farzin M (2007). Assessment of the Level of the Pregnant Women's Knowledge towards the Advantages and Disadvantages of Normal Vaginal Delivery and Cesarean Section, Tehran (2005). Iran Uni Med Sci J, 14(55): 13–22 [in Persian]. [Google Scholar]
- Sehhati Shafai F, Kazemi S, Ghojazadeh M (2013). Comparing Maternal Outcomes in Nulliparous Women in Labor in Physiological and Conventional Labor: A Randomized Clinical Trial. Mazandaran Uni Med Sci J, 23(97): 122–131 [in Persian]. [Google Scholar]
- Monar F, Mario S, Facchinetti F, Basevi V (2008). Obstetricians’ and midwives’ attitudes toward cesarean section. BIRTH, 35(2): 129–135. [DOI] [PubMed] [Google Scholar]
- Bahrie M, Latifnejad R, Abdollahian E, Esmaili H (2004). Effect of midwife's psycologiy & physical & Educational supportive in duration of labor stages and lobor pain force. Sabzevar Uni Medl SciJ, 11(1): 23–24 [in Persian]. [Google Scholar]
- Black C, Kaye J, Jick H (2005). Cesarean delivery in the United Kingdom: Time trends in the general practice research database. J Obstet Gy, 106(1): 151–155. [DOI] [PubMed] [Google Scholar]
- Mohammad Pour Asl A, Rostami F, Torabi S (2006). Prevalence of cesarean section and its demographic correlates in Tabriz. Tabriz Uni of Med Sci J, 28(3): 101–105 [in Persian]. [Google Scholar]
- Vaziran A (2000). Cesarean Culture. Dard, 254–55 [in Persian]. [Google Scholar]
- Aram S, Allame Z, Zamani M, Yadegar N (2002). The relative frequency of the delivery method in the pregnant women referring to medical centers of Isfahan in 2002. IJOGI, 8(4): 74–79 [in Persian]. [Google Scholar]
- Dastjerdi M (1998). A Survey of Indications, Outcome and Complications of Cesarean Section. Tehran Uni of Med Sci J, 56(1): 42–45 [in Persian]. [Google Scholar]
- Moradan S (2004). Evaluation of selection of route of delivery and its causes in patients referring to medical centers of Semnan from April till September 2004. IJOGI, 7(2): 44–49 [in Persian]. [Google Scholar]
- Piri S, Kiani A (2001). A survey on the prevalence and reasons of different types of delivery and the effect of demographic factors on it. Daneshvar, 8(35): 7–14 [in Persian]. [Google Scholar]
- Alimohamadian M, Shariat M, Mahmoodi M, Ramezanzadeh F (2003). The survey of impact of pregnant women's request in selected cesarean. Payesh, 2(2): 133–139 [in Persian]. [Google Scholar]
- Shareat M, Majlasei F, Azarei S, Mahmodei M (2002). Cesarean section rate and its determinants in maternity hospitals in Tehran. Payesh, 1(3): 5–10 [in Persian]. [Google Scholar]
- Asghar M, Parivash A, Fatemeh R, Arezoo A, Hossein A (2009). Investigating the Choice of Delivery Method Type and Its Related Factors in Pregnant Womenin Maragheh. Knowledge & Health, 4(1): 36–39 [in Persian]. [Google Scholar]
- Alavije Z, Shahry P, Kalhory M, Haghighizadeh M, Sharifirad G, Khorsandi M (2012). Identification of factors related to elective cesarean labor: a theory-based study. Daneshvar, 19(96): 1–11 [in Persian]. [Google Scholar]
- Sharghi A, Kamran A, Sharifirad G. R (2011). Assessing the factors influencing delivery method selection in primiparous pregnant women referred to health centers in Ardabil, 2010. Hormozghan Uni of Med Sci J, 15(3): 234–242 [In Persian]. [Google Scholar]
- Behague D, Victora C, Barros F (2002). Consumer demand for caesarean sections in Brazil: informed decision making, patient choice, or social inequality? A population based birth cohort study linking ethnographic and epidemiological methods. BMJ, 324(7343): 942–945. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Faraji Dor Khaneh R, Zahiri S, Farjad B (2003). Knowledge and Attitudes of pregnant women to normal delivery methods. Guilan Uni of Med Sci J, 12(46): 69–75 [in Persian]. [Google Scholar]
- Signorelli C, Cattaruzza M, Osborn J (1995). Risk factors for caesarean section in Italy: results of a multicenter study. J Public Health, 109(3): 191–199. [DOI] [PubMed] [Google Scholar]
- Menacker F, Declercq E, Mac M (2006). Cesarean delivery: background, trends, and epidemiology. Semin Perinatol, 30(5): 235–241. [DOI] [PubMed] [Google Scholar]
- Mobaraki A, Zadeh bagheri G, Zandi ghashghaie K (2005). Prevalence of cesarean section and the related causes in yasuj city in 2003. Yasuj Uni of Med Sci J, 39(10): 65–72. [Google Scholar]
- Shariat M, Majlesi F, Azari S, Mahmoodi M (2002). Cesarean section in maternity hospitals in Tehran, Iran. Payesh, 3(1): 5–10 [in Persian]. [Google Scholar]
- Tamook A, Aminisani N, Mogadam yeganeh G (2003). Cesarean section rate and its indications in social-security hospital of Ardabil, 2003. Ardabil Uni of Med Sci J, 8(2): 28–32 [in Persian]. [Google Scholar]
- Shakerian B (2004). Prevalence and causes of cesarean section in chaharmahal & bakhtiary, 2002. Shahrekord Uni of Med Sci J, 1(6): 63–69 [in Persian]. [Google Scholar]
- Kashanizadeh N (2002). Rate and indication of cesarean section delivery in Baghiyatollah hospital. KMJ, 3(7): 239–243 [in Persian]. [Google Scholar]
- Khosrovi M, Arnat M, Khadem N (2006). The Assessment of Prevalence of Cesarean and Related Factors. J of Nurs and Midwif, 58(16): 21–27 [in Persian]. [Google Scholar]
- Mohammad Pour Asl A, Asgharian P, Rostami F, Azizi A, Akbari H (2009). Investigating the choice of delivery method type and its related factors in pregnant women in Maragheh knowledge & health. Knowledge & Health J, 4(1): 36–39 [in Persian]. [Google Scholar]
- Seyed Noori T, Jamshidi Aranaki F (2006). Survey the Relationship Between Knowledge and Attitude Of Pregnant Women Requesting Cesarean Section Referred to Rasht Health Centers and Their choice Reasons. Guilan Uni of Med Sci J, 15(59): 75–84 [in Persian]. [Google Scholar]
- Negahban T, Ansari Jaberei A, Kazemi M (2006). The preferred delivery method and influenced factors from view of pregnant women referred to Rafsanjan city health and treatment units and clinics. Rafsanjan Uni Med Sci J, 5(3): 161–168 [in Persian]. [Google Scholar]
- Bagheri A, Masoodi-Alavi N, Abbaszade F (2012). Effective factors for choosing the delivery method among the pregnant women in Kashan. FEYZ, 16(2): 146–153. [Google Scholar]
- Atghaei M, Nouhi A (2010). Imagine the pain of labor and cesarean and vaginal delivery in pregnant women tends to be referred to clinics in Kerman University of Medical Sciences. IJOGI, 14(7): 44–50 [in Persian]. [Google Scholar]
- Bolbol Haghighi N, Ebrahimi H, Ajami M (2002). Comparison of frequency of vaginal delivery with cesarean section and its causes in Shahroud, 2000. Med J Reproduction & Infertility, 10(3): 50–58 [In Persian]. [Google Scholar]
- Solimanizadeh L, Solimanizadeh F, Asghari Zadeh Mahani M, Zafarnia N, Javadi M (2009). A Survey of Mother BMI Relationship with Cesarean Prevalence Rate in Bam Maternity Hospital, Bam, Iran Mahdyeh. Qom Uni Med Sci J, 3(4): 49–54 [In Persian]. [Google Scholar]
- Motamedi B, Janghorbani M, Eftekhar N (2000). Prevalence of Cesarean Section and Some Determinant Factors in Kerman. Guilan Uni Med Sci J, 33–34(9): 88–95 [in Persian]. [Google Scholar]
- Rahmanian K, Fasori M, Rahmanian V (2011). Cesarean, ever to need attention: Prevalence and causes of cesarean section in Jahrom, 2008. Jahrom Uni Med Sci J, 9(1): 1–13 [in Persian]. [Google Scholar]
- Jamshidi Manesh F, Oskouie S, Jouybary L, Sanagoo A (2009). The Process of Women's Decision Making for Selection of Cesarean Delivery. Iran J Nursing, 56(21): 55–67 [in Persian] [Google Scholar]
- Jodati A, Yavari Kia P (2000). Incidence and indication of cesarean in the eastern Azerbaijan of Iran. Tabriz Uni Med Sci J, 46(34): 19–24 [in Persian]. [Google Scholar]
- Taatari F, Abdi P, Afshari P, Hagigi zadeh MH (2004). A comparative study of the frequency of cesarean section in pregnant women attending selected private hospitals and educational Mashhad. Ilam Uni Med Sci J, 12(42–43); 25–31 [In Persian]. [Google Scholar]
- Fathian Z, sharifirad G, Fathian Z, Pezeshkihebi F (2010). Frequency of cesarean section and its related factors in Khomeinyshahr-Isfahan province 2005. HSRJ, 6(4): 786–793 [in Persian]. [Google Scholar]
- Davari M, Maracy M, Ghorashi Z, Mokhtari M (2012). The Relationship between Socioeconomic Status and the Prevalence of Elective Cesarean Section in Nulliparous Women in Niknafs Teaching Center, Rafsanjan, Iran. Health Information Management, 8(7): 965 [in Persian]. [Google Scholar]
- Ghasemi F (2012). Investigating the abundance of caesarean section and its reason in Yazd in 2009. Shahid Sadoughi Uni Med Sci J, 20(2): 229–236 [in Persian]. [Google Scholar]
- Moeini B, Allahverdipour H, Mahjoub H, Bashirian S (2011). Assessing pregnant women's beliefs, behavioral intention and predictive factors for cesarean section in Hamadan. Iranian J Obstetrics Gyne Infe, 14(3): 37–44 [in Persian]. [Google Scholar]
- Tabande A, Kashani E (2007). Prevalence of cesarean in educated woman of medical sciences group in Gorgan (2004). Gorgan Uni Med Sci J, 9(2): 67–70 [in Persian]. [Google Scholar]
- Bahonar A, Shaebani A, Aghajani M (2010). Case-control study of factors affecting the cesarean section of ten years in the city of Damghan, 1998–2009. Iranian J Epidemiol, 6(1): 33–38 [in Persian]. [Google Scholar]
- Naseh N, Khazaie T, Kianfar S, Dehghan R, Yoosefi S (2010). Prevalence of Cesarean and its complications in women referring to Vali-e-Asr hospital. Modern Care, 7(1–2): 12–18 [in Persian]. [Google Scholar]
- Ghooshchian S, Dehghani M, Khorsandi M, Farzad V (2011). The role of fear of pain and related psychological variables in prediction of cesarean labor. Arak Uni Med Sci J, 14(56): 45–54[in Persian]. [Google Scholar]
- Asnafi N, Hajian K, Hesari H (2002). Causes and complications of emergency Cesarean-section in Yahyanejad Hospital, Babol, 1999. Babol Uni Med Sci J, 13(4): 16–19 [in Persian]. [Google Scholar]