

Abstract
Aim:
To systematically review the anesthetic success rates of inferior alveolar nerve block (IANB) injection technique alone with that of combination of IANB and supplemental infiltration (SI) technique when used for pulpal anesthesia of mandibular posterior teeth with irreversible pulpitis during endodontic treatment.
Settings and Design:
The study follows a longitudinal study design involving original research.
Materials and Methods:
Electronic databases were systematically searched for randomized controlled clinical studies. Studies were selected by predefined inclusion and exclusion criteria.
Statistical Analysis Used and Result:
The statistical analysis used was based on the results of the original research. All the included studies showed that there is the difference in the values comparing the two techniques, but the data are not statistically significantly different.
Conclusion:
Based on this review, the better anesthetic efficacy of the SI was observed.
Keywords: Anesthetic success, inferior alveolar nerve block, irreversible pulpitis, pulpal anesthesia, supplemental infiltration technique
INTRODUCTION
Successful local anesthesia is important for pain control. Fear and anxiety associated with endodontic treatment is reduced with effective pain management.[1] It was found that the anesthesia of mandibular molars with irreversible pulpitis was more difficult than the healthy pulps.[2,3,4] The reason for difficulty in pulpal anesthesia of teeth with irreversible pulpitis were described in previous studies.[5,6,7,8,9,10]
Maxillary teeth requiring dental procedures can be successfully anesthetize by infiltration of buccal mucosa. However in mandibular teeth due to the thickness of buccal cortical bone buccal infiltration technique is not as effective as nerve block techniques.[11] Pulpal anesthesia of posterior mandibular teeth with irreversible pulpitis is most frequently achieved by the inferior alveolar nerve block (IANB) injection technique. However, sometimes it does not produce desired anesthesia.[12] The failure rate is between 44% and 81% as was described in various clinical studies.[3,13,14,15] Due to the failure rate of IANB, problems are commonly encountered while treating mandibular teeth with irreversible pulpitis.[16]
When the conventional IANB fails, supplemental injections (with different techniques and/or types of anesthetic) are frequently required in patients with irreversible pulpitis to achieve complete anesthesia.[17] Supplemental techniques such as the intraosseous,[3,13] intraligamentary,[14,18] and infiltration[19,20] injections technique have been studied to raise the anesthetic success. The intraosseous injection requires special equipment for drilling the cortical bone and injecting the anesthetic solution thus is not a preferred technique.[4] The intraligamentary injections are short lasting and may increase pain postoperatively.[21] It would be useful to have results produced by these techniques be achieved with simpler options such as infiltration technique.
Infiltration injection increases the success of IANB injection and is used very often as the supplemental injection technique.[20,22,23] The present systematic review compared and evaluated the anesthetic success rates of IANB injection technique alone or along with supplemental infiltration (SI) technique when used for pulpal anesthesia of mandibular posterior teeth with irreversible pulpitis.
MATERIALS AND METHODS
Electronic databases were systematically searched. The search was done in PubMed and MEDLINE (Twease) and Google search engine. The search was performed using following search terms alone and in combination “pulpal anesthesia in mandibular teeth and irreversible pulpitis,” “IANB and irreversible pulpitis,” “Infiltration in mandibular teeth and irreversible pulpitis.” The search was done till March 2014.
The inclusion and exclusion criteria for selecting the studies for the systematic review were listed in Table 1. The 284 studies titles found were scrutinized for duplicacy and 159 studies were included. The abstract of 159 studies were then assessed depending on the predetermined criteria, to identify 14 relevant studies and 145 studies were excluded. The full texts of the 14 relevant studies were further analyzed and found only 6 studies were eligible, which were meeting the defined specific criteria.
Table 1.
Predefined criteria

The Structured question was “Is there any difference in the anesthetic success rates of IANB injection technique used alone compared with the combination of IANB and SI injection technique when used for pulpal anesthesia of mandibular teeth with irreversible pulpitis.”
The Pico analysis was performed where the population was represented by patients with irreversible pulpitis in posterior mandibular teeth. The intervention done was access preparation and instrumentation to assess pulpal anesthesia. The comparison was between IANB alone or along with SI technique. The primary outcome was a percentage of successful pulpal anesthesia in the block alone or along with the SI technique with the help of Heft Parker visual analog scale (HP-VAS) method while performing the endodontic procedure. HP-VAS with a 170-mm line marked with various terms describing the levels of pain was used for this purpose. The millimeter marks were removed from the scale, and the scale was divided into four categories: “no pain” corresponded to 0 mm; “faint, weak, or mild” pain corresponded to 0-54 mm; “moderate” pain 55-114 mm; and “strong, intense, and maximum possible” pain corresponded above 114 mm. The success was defined as no or mild pain during access preparation and instrumentation.
RESULT
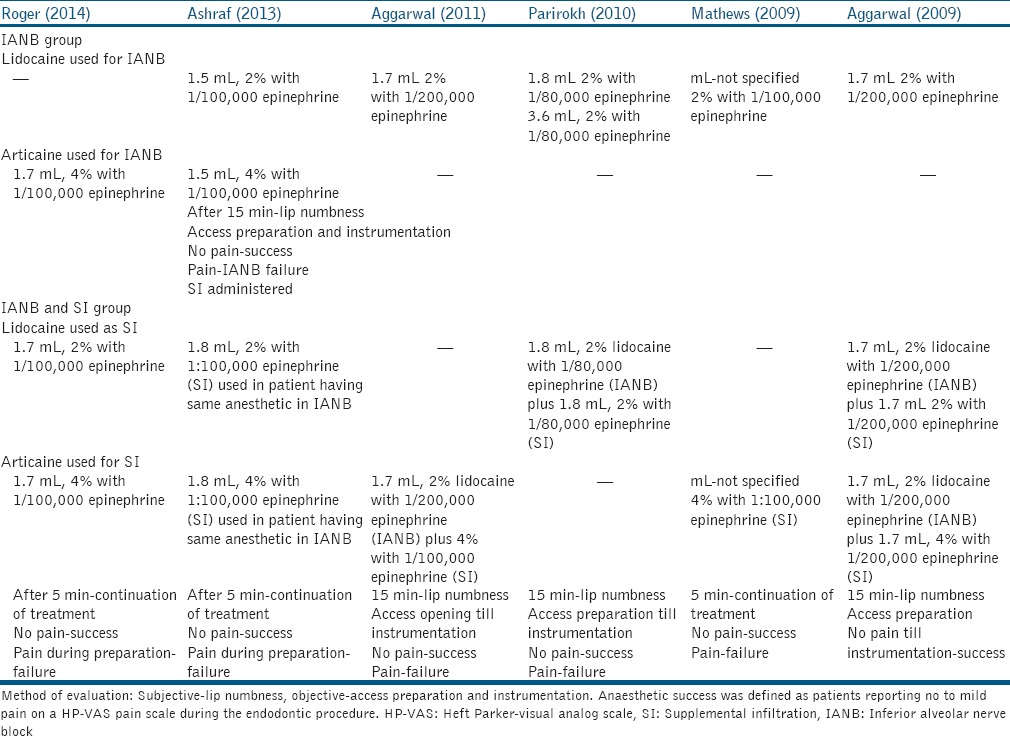
The study design of the included studies[43,44,45,46,47,48] was shown in Table 2.
Table 2.
Study design of the included studies
The list of excluded studies with reason for exclusion was shown in Table 3.
Table 3.
Studies with reason for exclusion

The comparison of percentage of patients with successful anesthesia with IANB alone and SI technique (“no pain” or “weak/mild” pain during endodontic access preparation and instrumentation) was presented in Table 4.
Table 4.
The comparison of percentage of patients with successful anesthesia with IANB (block) and IANB and SI

Inferior alveolar nerve block alone gave 14-39% success rate. With SI the local anesthetic significantly increased the success rate 50-65%. None of the technique gave 100% success rate.
DISCUSSION
The difficulty regarding adequate pain control in the posterior region of the mandible during dental procedures has been reported. The most frequently used injection technique in such region has been IANB. The reduced efficacy of IANB has been associated with various factors such as the thickness of cortical bone, overlying soft tissue and accessory innervations.[25,26,27]
Success rate of IANB in an uninflamed pulp was reported to be 70% compared with 30% in patients with irreversible pulpitis.[2,12,14,29,30,31,32,33] It was also reported that the failure of local anesthesia in patients with irreversible pulpitis was found to be 8 times more with respect to normal patients.[4] Thus, the present study was undertaken to compare the success rates of IANB alone or along with the SI technique in irreversible pulpitis.
Achieving pulpal anesthesia is difficult in irreversible pulpitis. Various reasons have been described. First, the inflamed tissue has a lowered pH as a result of which the amount of the base form of the anesthetic required to go through the nerve sheath and membrane has reduced. This leads to decreased ionized form of the anesthetic within the nerve with resultant decreased anesthesia. Second, altered resting potentials and lowered thresholds of excitability of the nerves in the inflamed tissue.[34,35] As a result of lowered threshold of excitability of these nerves, the prevention of transmission of nerve impulses by the anesthetic agents were not attained.[34,36] Third, there were anesthetic resistant sodium channels[37] and upregulation of sodium channels in pulp[38] with irreversible pulpitis.
The patients in the included studies of the review were actively experiencing pain in mandibular posterior teeth and were diagnosed with irreversible pulpitis. The subject was asked to rate the pain before the treatment and during the treatment using a HP-VAS. All received the standard IANB injection. After 15 min of injection, patients were evaluated for lip numbness. Profound lip numbness was the subjective criteria selected for the inclusion of the subjects in all the studies. Subjects, where lip numbness was not evident, were excluded from the study.
Lip numbness was used as subjective criteria for the inclusion of the subjects in the study. It should be noted that all the patients included in the study had subjective symptoms of lip numbness, but the anesthesia was not successful in all cases. Patient experienced pain during endodontic procedures despite lip numbness.
Patient's age, gender, posterior tooth type, initial pain in the included studies were not significantly different between the two groups. Furthermore, patients included were not premedicated, had no systemic conditions such as diabetes, heart disease, high blood pressure. Therefore, it can be assumed that the results of this study are not affected by these factors as a result of which the two groups can be compared on their respective anesthetic success.
In all the selected studies, anesthetic response of the patient was taken 15 min after IANB and 5 min after the SI as this time period was previously reported to obtain complete anesthesia.[32,33]
The HP-VAS was used in the included studies to rate the pain to measure the degree of pulpal anesthesia. However, two methods have been used to assess the efficacy of local anesthetic injections in previous studies. Some investigators have used pulp sensibility tests such as electric pulp tester (EPT) or the cold test, whereas others have used the HP-VAS. HP-VAS was selected in the inclusion criteria of the review for measuring pain level. EPT was not considered for pain measurement as Nusstein et al. found in their study that 42% of the patient who received anesthesia despite giving a negative response to EPT experienced pain during treatment.[13]
Various methods have been used for assessing pulpal anesthesia Bjorn[40] was the first to correlate a negative response to the maximum output of electrical pulp stimulation to painless dental treatment. However, negative response to EPT does not produce profound anesthesia. Also, lip numbness is not the indication of pulpal anesthesia. Therefore, the preparation of access cavity and extirpation of pulp was used to measure effectively the success of pulpal anesthesia using HP-VAS.
The studies reviewed were randomized control trial and clinical trials. The method used in the studies followed CONSORT guidelines. The inclusion and exclusion criteria were well defined. Sample size calculation was done in all studies and dropouts were noted. Randomization of patients in the two groups and blinding of the anesthetic agent was performed to eliminate any bias. The statistical analyses were well-defined.
CONCLUSION
The anesthetic success was clinically evident with SI injection technique as compared to IANB injection technique, but was not statistically significant in the studies. None of the technique gave 100% success.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Saberi EA, Farhadmollashahi N, Aliabadi T. A Comparison of the anesthesia efficacy of articaine and articaine plus morphine for buccal infiltration in mandibular posterior teeth with irriversible pulpitis. ZJRMS. 2014;16:26–30. [Google Scholar]
- 2.Tortamano IP, Siviero M, Costa CG, Buscariolo IA, Armonia PL. A comparison of the anesthetic efficacy of articaine and lidocaine in patients with irreversible pulpitis. J Endod. 2009;35:165–8. doi: 10.1016/j.joen.2008.10.020. [DOI] [PubMed] [Google Scholar]
- 3.Reisman D, Reader A, Nist R, Beck M, Weaver J. Anesthetic efficacy of the supplemental intraosseous injection of 3% mepivacaine in irreversible pulpitis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1997;84:676–82. doi: 10.1016/s1079-2104(97)90372-3. [DOI] [PubMed] [Google Scholar]
- 4.Hargreaves KM, Keiser K. Local anesthetic failure in endodontics: Mechanisms and management (a review) Endod Topics. 2002;1:26–39. [Google Scholar]
- 5.Walton RE, Torabinejad M. Managing local anesthesia problems in the endodontic patient. J Am Dent Assoc. 1992;123:97–102. doi: 10.14219/jada.archive.1992.0133. [DOI] [PubMed] [Google Scholar]
- 6.Hargreaves KM. Managing local anesthesia problems in the endodontic patient. J Am Dent Assoc. 1992;123:97–102. doi: 10.14219/jada.archive.1992.0133. [DOI] [PubMed] [Google Scholar]
- 7.Hannan L, Reader A, Nist R, Beck M, Meyers WJ. The use of ultrasound for guiding needle placement for inferior alveolar nerve blocks. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1999;87:658–65. doi: 10.1016/s1079-2104(99)70156-3. [DOI] [PubMed] [Google Scholar]
- 8.Rood JP, Pateromichelakis S. Inflammation and peripheral nerve sensitisation. Br J Oral Surg. 1981;19:67–72. doi: 10.1016/0007-117x(81)90023-8. [DOI] [PubMed] [Google Scholar]
- 9.Wallace JA, Michanowicz AE, Mundell RD, Wilson EG. A pilot study of the clinical problem of regionally anesthetizing the pulp of an acutely inflamed mandibular molar. Oral Surg Oral Med Oral Pathol. 1985;59:517–21. doi: 10.1016/0030-4220(85)90095-7. [DOI] [PubMed] [Google Scholar]
- 10.Dworkin SF. Anxiety and performance in the dental environment: An experimental investigation. J Am Soc Psychosom Dent Med. 1967;14:88–103. [PubMed] [Google Scholar]
- 11.Haas DA, Harper DG, Saso MA, Young ER. Comparison of articaine and prilocaine anesthesia by infiltration in maxillary and mandibular arches. Anesth Prog. 1990;37:230–7. [PMC free article] [PubMed] [Google Scholar]
- 12.Claffey E, Reader A, Nusstein J, Beck M, Weaver J. Anesthetic efficacy of articaine for inferior alveolar nerve blocks in patients with irreversible pulpitis. J Endod. 2004;30:568–71. doi: 10.1097/01.don.0000125317.21892.8f. [DOI] [PubMed] [Google Scholar]
- 13.Nusstein J, Reader A, Nist R, Beck M, Meyers WJ. Anesthetic efficacy of the supplemental intraosseous injection of 2% lidocaine with 1:100,000 epinephrine in irreversible pulpitis. J Endod. 1998;24:487–91. doi: 10.1016/S0099-2399(98)80053-8. [DOI] [PubMed] [Google Scholar]
- 14.Cohen HP, Cha BY, Spångberg LS. Endodontic anesthesia in mandibular molars: A clinical study. J Endod. 1993;19:370–3. doi: 10.1016/S0099-2399(06)81366-X. [DOI] [PubMed] [Google Scholar]
- 15.Kennedy S, Reader A, Nusstein J, Beck M, Weaver J. The significance of needle deflection in success of the inferior alveolar nerve block in patients with irreversible pulpitis. J Endod. 2003;29:630–3. doi: 10.1097/00004770-200310000-00004. [DOI] [PubMed] [Google Scholar]
- 16.Raj JD, Ramesh S. Evaluation of the anesthetic efficacy of inferior alveolar nerve blocks in dental patients — A systematic review. IOSR J Dent Med Sci. 2013;8:10–7. [Google Scholar]
- 17.Fan S, Chen WL, Pan CB, Huang ZQ, Xian MQ, Yang ZH, et al. Anesthetic efficacy of inferior alveolar nerve block plus buccal infiltration or periodontal ligament injections with articaine in patients with irreversible pulpitis in the mandibular first molar. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;108:e89–93. doi: 10.1016/j.tripleo.2009.06.012. [DOI] [PubMed] [Google Scholar]
- 18.Nusstein J, Claffey E, Reader A, Beck M, Weaver J. Anesthetic effectiveness of the supplemental intraligamentary injection, administered with a computer-controlled local anesthetic delivery system, in patients with irreversible pulpitis. J Endod. 2005;31:354–8. doi: 10.1097/01.don.0000140565.88940.60. [DOI] [PubMed] [Google Scholar]
- 19.Meechan JG, Kanaa MD, Corbett IP, Steen IN, Whitworth JM. Pulpal anaesthesia for mandibular permanent first molar teeth: A double-blind randomized cross-over trial comparing buccal and buccal plus lingual infiltration injections in volunteers. Int Endod J. 2006;39:764–9. doi: 10.1111/j.1365-2591.2006.01144.x. [DOI] [PubMed] [Google Scholar]
- 20.Kanaa MD, Whitworth JM, Corbett IP, Meechan JG. Articaine and lidocaine mandibular buccal infiltration anesthesia: A prospective randomized double-blind cross-over study. J Endod. 2006;32:296–8. doi: 10.1016/j.joen.2005.09.016. [DOI] [PubMed] [Google Scholar]
- 21.McLean ME, Wayman BE, Mayhew RB. Duration of anesthesia using the periodontal ligament injection: A comparison of bupivacaine to lidocaine. Anesth Pain Control Dent. 1992;1:207–13. [PubMed] [Google Scholar]
- 22.Aggarwal V, Jain A, Kabi D. Anesthetic efficacy of supplemental buccal and lingual infiltrations of articaine and lidocaine after an inferior alveolar nerve block in patients with irreversible pulpitis. J Endod. 2009;35:925–9. doi: 10.1016/j.joen.2009.04.012. [DOI] [PubMed] [Google Scholar]
- 23.Parirokh M, Satvati SA, Sharifi R, Rekabi AR, Gorjestani H, Nakhaee N, et al. Efficacy of combining a buccal infiltration with an inferior alveolar nerve block for mandibular molars with irreversible pulpitis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010;109:468–73. doi: 10.1016/j.tripleo.2009.11.016. [DOI] [PubMed] [Google Scholar]
- 24.Poorni S, Veniashok B, Senthilkumar AD, Indira R, Ramachandran S. Anesthetic efficacy of four percent articaine for pulpal anesthesia by using inferior alveolar nerve block and buccal infiltration techniques in patients with irreversible pulpitis: A prospective randomized double-blind clinical trial. J Endod. 2011;37:1603–7. doi: 10.1016/j.joen.2011.09.009. [DOI] [PubMed] [Google Scholar]
- 25.Ogle OE, Mahjoubi G. Local anesthesia: Agents, techniques, and complications. Dent Clin North Am. 2012;56:133–48, ix. doi: 10.1016/j.cden.2011.08.003. [DOI] [PubMed] [Google Scholar]
- 26.Kanaa MD, Whitworth JM, Meechan JG. A prospective randomized trial of different supplementary local anesthetic techniques after failure of inferior alveolar nerve block in patients with irreversible pulpitis in mandibular teeth. J Endod. 2012;38:421–5. doi: 10.1016/j.joen.2011.12.006. [DOI] [PubMed] [Google Scholar]
- 27.Malamed SF. Is the mandibular nerve block passé? J Am Dent Assoc. 2011;142(Suppl 3):3S–7. doi: 10.14219/jada.archive.2011.0340. [DOI] [PubMed] [Google Scholar]
- 28.Laskin DM. Diagnosis and treatment of complications associated with local anaesthesia. Int Dent J. 1984;34:232–7. [PubMed] [Google Scholar]
- 29.Goldberg S, Reader A, Drum M, Nusstein J, Beck M. Comparison of the anesthetic efficacy of the conventional inferior alveolar, Gow-Gates, and Vazirani-Akinosi techniques. J Endod. 2008;34:1306–11. doi: 10.1016/j.joen.2008.07.025. [DOI] [PubMed] [Google Scholar]
- 30.Childers M, Reader A, Nist R, Beck M, Meyers WJ. Anesthetic efficacy of the periodontal ligament injection after an inferior alveolar nerve block. J Endod. 1996;22:317–20. doi: 10.1016/S0099-2399(96)80267-6. [DOI] [PubMed] [Google Scholar]
- 31.Dagher BF, Yared GM, Machtou P. The anesthetic efficacy of volumes of lidocaine in inferior alveolar nerve blocks. J Endod. 1997;23:178–80. doi: 10.1016/S0099-2399(97)80271-3. [DOI] [PubMed] [Google Scholar]
- 32.Vreeland DL, Reader A, Beck M, Meyers W, Weaver J. An evaluation of volumes and concentrations of lidocaine in human inferior alveolar nerve block. J Endod. 1989;15:6–12. doi: 10.1016/S0099-2399(89)80091-3. [DOI] [PubMed] [Google Scholar]
- 33.Mikesell P, Nusstein J, Reader A, Beck M, Weaver J. A comparison of articaine and lidocaine for inferior alveolar nerve blocks. J Endod. 2005;31:265–70. doi: 10.1097/01.don.0000140576.36513.cb. [DOI] [PubMed] [Google Scholar]
- 34.Wallace J, Michanowicz A, Mundell R, et al. A pilot study of the clinical problem of regionally anesthetizing the pulp of an acutely inflamed mandibular molar. Oral Surg Oral Med Oral Pathol. 1985;59:517–21. doi: 10.1016/0030-4220(85)90095-7. [DOI] [PubMed] [Google Scholar]
- 35.Byers M, Taylor P, Khayat B, et al. Effects of injury and inflammation on pulpal and periapical nerves. J Endod. 1990;16:78–84. doi: 10.1016/S0099-2399(06)81568-2. [DOI] [PubMed] [Google Scholar]
- 36.Modaresi J, Dianat O, Soluti A. Effect of pulp inflammation on nerve impulse quality with or without anesthesia. J Endod. 2008;34:438–41. doi: 10.1016/j.joen.2008.01.014. [DOI] [PubMed] [Google Scholar]
- 37.Roy M, Narahashi T. Differential properties of tetrodotoxin sensitive and tetrodoxin resistant sodium channels in rat dorsal root ganglion neurons. J Neurosci. 1992;12:2104–11. doi: 10.1523/JNEUROSCI.12-06-02104.1992. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Sorensen H, Skidmore L, Rzasa D, et al. Comparison of pulpal sodium channel density in normal teeth to diseased teeth with severe spontaneous pain. J Endod. 2004;30:287. [Google Scholar]
- 39.Robertson D, Nusstein J, Reader A, et al. The anesthetic efficacy of articaine in buccal infiltration of mandibular posterior teeth. J Am Dent Assoc. 2007;138:1104–12. doi: 10.14219/jada.archive.2007.0324. [DOI] [PubMed] [Google Scholar]
- 40.Bjorn H. Electrical excitation of teeth and its application to dentistry. Swed Dent J. 1946;39:87–96. [Google Scholar]
- 41.Dreven LJ, Reader A, Beck M, Meyers WJ, Weaver J. An evaluation of an electric pulp tester as a measure of analgesia in human vital teeth. J Endod. 1987;13:233–8. doi: 10.1016/s0099-2399(87)80097-3. [DOI] [PubMed] [Google Scholar]
- 42.Hsiao-Wu GW, Susarla SM, White RR. Use of the cold test as a measure of pulpal anesthesia during endodontic therapy: A randomized, blinded, placebo controlled trial. J Endod. 2007;33:406–10. doi: 10.1016/j.joen.2006.12.009. [DOI] [PubMed] [Google Scholar]
- 43.Aggarwal V, Jain A, Kabi D. Anesthetic efficacy of supplemental buccal and lingual infiltrations of articaine and lidocaine after an inferior alveolar nerve block in patients with irreversible pulpitis. J Endod. 2009;35:925–9. doi: 10.1016/j.joen.2009.04.012. [DOI] [PubMed] [Google Scholar]
- 44.Aggarwal V, Singla M, Rizvi A, Miglani S. Comparative evaluation of local infiltration of articaine, articaine plus ketorolac, and dexamethasone on anesthetic efficacy of inferior alveolar nerve block with lidocaine in patients with irreversible pulpitis. J Endod. 2011;37:445–9. doi: 10.1016/j.joen.2011.01.016. [DOI] [PubMed] [Google Scholar]
- 45.Ashraf H, Kazem M, Dianat O, Noghrehkar F. Efficacy of articaine versus lidocaine in block and infiltration anesthesia administered in teeth with irreversible pulpitis: A prospective, randomized, double-blind study. J Endod. 2013;39:6–10. doi: 10.1016/j.joen.2012.10.012. [DOI] [PubMed] [Google Scholar]
- 46.Parirokh M, Satvati SA, Sharifi R, Rekabi AR, Gorjestani H, Nakhaee N, Abbott PV. Efficacy of combining a buccal infiltration with an inferior alveolar nerve block for mandibular molars with irreversible pulpitis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010;109:468–73. doi: 10.1016/j.tripleo.2009.11.016. [DOI] [PubMed] [Google Scholar]
- 47.Rogers BS, Botero TM, McDonald NJ, BDS, Gardner RJ, Mathilde C, Peters MC. Efficacy of Articaine versus Lidocaine as a Supplemental Buccal Infiltration in Mandibular Molars with Irreversible Pulpitis: A prospective, randomized, double-blind study. J Endod. 2014;40:753–8. doi: 10.1016/j.joen.2013.12.022. [DOI] [PubMed] [Google Scholar]
- 48.Matthews R, Drum M, Reader A, Nusstein J, Beck M. Articaine for supplemental buccal mandibular infiltration anesthesia in patients with irreversible pulpitis when the inferior alveolar nerve block fails. J Endod. 2009;35:343–6. doi: 10.1016/j.joen.2008.11.025. [DOI] [PubMed] [Google Scholar]