

Abstract
Objective:
The aim of the study is to evaluate temperature change in fiber-reinforced composite (FRC) resin photopolymerized with a light-emitting diode (LED) light-curing unit (LCU).
Materials and Methods:
Forty dentine disks (1 mm thick and 8 mm diameter) were prepared from human molars. The FRC specimens (2 mm thickness and 8 mm diameter) consisted of polyethylene fiber (Construct (CT)) products or glass fiber (ever Stick (ES)) and one hybrid composite bonded to the dentin disks and polymerized with an LED LCU. Control groups were prepared using the hybrid composite. Temperature rise in dentine samples under the FRC bonded disks was measured using a K-type thermocouple, and data were recorded. Temperature change data were subjected to analysis of variance (ANOVA) and Duncan's test.
Results:
The results show that addition of fiber (one or two layers) did not change temperature rise values at any of the exposure times (P > 0.05). The CT fiber/two layer/40 s group exhibited the greatest temperature rise (5.49 ± 0.62) and the ES/one layer/10 s group the lowest rise (1.75 ± 0.32). A significant difference was observed in temperature rise measured during 10 and 20 s exposures (P < 0.05).
Conclusion:
Maximal temperature rise determined in all groups was not critical for pulpal health, although clinicians need to note temperature rises during polymerization.
Keywords: Dentin, fiber-reinforced composite, polymerization, temperature rise
INTRODUCTION
Dental composite resins polymerize with free-radical polymerization under irradiation with visible light, using a wavelength of 400-500 nm.[1] Polymerization of the composite resin restorative materials and the heat of irradiation of dental light-curing units (LCUs) are sources of temperature rise (rise) in the tooth cavity, and this may damage the pulp.[2] Polymerization of the composite resins produces a temperature increase, caused by exothermic reaction and the energy absorbed during polymerization.[3] It has been suggested that external heating may enhance the conversion kinetics of resin composites and the mobility of reactive species during polymerization.[4]
Pulp is a highly vascularized tissue, and pulpal temperature is critical. Protection of the dentin-pulp complex by avoiding thermal stimuli is therefore an important factor in pulp vitality during operative procedures.[5] The total duration of harmful temperature rise is significant for pulpal health.
Temperature rise during polymerization is influenced by factors such as intensity of light, composition of composite resins, transmission properties of the composite resins, depth of the cavity or restoration, duration of light exposure and type of light source.[6,7] When a deep cavity is prepared for restoration, restorative materials with low thermal conductivity should be used to maintain pulp health.[8] In methacrylate-based composite, the filler content is increased in order to reduce temperature rise during polymerization, as fillers are chemically inert and ineffective for thermal conductivity.[9]
Fiber-reinforced composites (FRCs) were introduced for dental restorations and possess highly favorable mechanical properties; their strength-to-weight ratios are superior to those of most alloys. They also have many other advantages over metal, including ease of repair, non-corrosiveness, translucency and good bonding properties.[10] Different practical solutions are possible for creating the composite and the fiber; the clinician may adapt the restorative technique to accommodate specific indications and obtain improved results with ease and reliability.[10] Their applications in diverse areas of dentistry includes chair-side periodontal splinting, orthodontic applications, the manufacture of laboratory-made single crowns, partial- or full-coverage fixed partial dentures, post-core systems, adhesive fixed partial dentures and trauma stabilization.[11,12,13,14] Temperature rise in FRC materials must be considered because fibers have a different structure to that of composite materials.
Studies of temperature rise during polymerization of FRC restorations are limited. The purpose of this study was to evaluate the effect of different fibers placed between dentin and composite resin on temperature rise during polymerization. The null hypothesis was that temperature rise would not be affected by fiber under the composite resin.
MATERIALS AND METHODS
The materials used in study are listed in Table 1. Forty dentin disks were prepared from extracted sound human third molars. Teeth were embedded in cylindrical acrylic blocks. The occlusal surfaces were first cut horizontally, exposing the dentin. Dentin disks, 1 mm thick and 8 mm in diameter, were produced using a universal slow speed saw (Isomet, Buehler, Evanston, IL, USA) under water cooling [Figure 1]. Specimens were divided into five groups (n = 8). Polyethylene fiber (Construct (CT), Kerr Corp, Calif) and glass fiber (everStick C&B (ES), Stick Tech, Turku, Finland) glass fiber were applied to the dentin disks according to the manufacturers’ instructions. Glass fiber was applied in Groups 1 and 2, and polyethylene fiber in Groups 3 and 4. These were applied as a single layer in Groups 1 and 3 and as two layers in Groups 2 and 4. In the control group (Group 5), a hybrid composite resin (Valux Plus, 3M ESPE Dental Products, St Paul, MN, USA) was applied 2 mm on samples.
Table 1.
Brand, type, manufacturer, and lot numbers of materials used in this study

Figure 1.
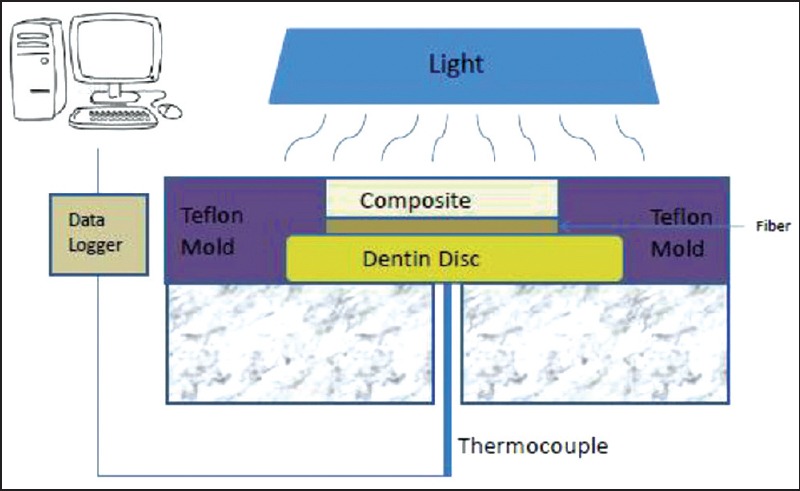
Schematic illustration of test procedure
A Teflon mold was prepared as a supporting structure for specimens [Figure 1]. The control group was prepared with hybrid composite in the same way, but without the fiber. The specimens were cured at room temperature (24°C). All specimens were polymerized with Elipar Freelight 2 LCU (3M ESPE Dental Products, St Paul, MN, USA). Based on the manufacturer's recommendations, composite resin was cured for 40 s. Temperature rises during polymerization were measured using a K-type thermocouple (E-680, Elimko Co, Ankara, Turkey). The thermocouple tip was placed under the dentin disks, and a thermocouple wire was connected to a data logger. In all groups, composite resins were polymerized for approximately 40 s. Temperature rise over time was recorded on a computer. Differences (ΔT) between baseline and each time interval were recorded, and data were analyzed using one-way ANOVA and Duncan's test at a 5% significance level with Statistical Package for Social Sciences (SPSS) 20 software.
RESULTS
Table 2 shows temperature rises during polymerization in all groups. According to the results from each curing period, addition of fiber (single or two layers) did not produce a significant change in ΔT values (P > 0.05). The highest temperature rise was observed in the CT/two layers/40 s group (5.49 ± 0.62) and the lowest temperature was recorded in the ES/one layer/10 s group (1.75 ± 0.32). Temperature rises during 0-10 s and 0-20 s curing were different from those during 0-30 s and 0-40 s curing (P < 0.05) in both the one- and two-layer fiber groups. In the control group, the temperature rise at 0-10 s was different to those obtained at other times. No significant temperature rise was observed in any group between 30 and 40 s exposures (P > 0.05).
Table 2.
ΔT values of each test group (mean ± standard deviation)

DISCUSSION
This study evaluated temperature changes in FRC resinphotopolymerized with an LCU. The tested null hypothesis was rejected because no differences were found in the temperature increase between the FRC and control groups. Temperature rise did not vary significantly depending on fiber layer.
External heat can increase the temperature in the pulp chamber. It causes inflammatory reactions and resulting damage to the pulp tissue. Clinical research has shown irreversible damage to pulp tissues of 15% at 5.5°C and 100% at 11°C.[15] Some research showed that an 11.2°C rise in temperature at the dentinopulpal junction was acceptable and that pain was felt at temperatures approaching 45°C.[16] Other studies have concluded that a safety limit of 6.1°C above normal pulpal temperature was applicable.[17] Temperature rises throughout curing are measurable using a thermocouple under dentin disks. In the literature, the K-type thermocouple is described as effective for measuring temperature rises under dentin disks during polymerization.[18] In our study we used a K-type thermocouple, and the maximum temperature rise did not exceed critical values for pulpal health. This may be related to the light source. The light-emitting diode (LED) unit has high power; it caused polymerization of composite resin in a short curing time. Temperature does not therefore rise too much during polymerization. Temperature rises may be harmful to pulp over long curing times. Zach and Cohen[19] reported that pulp showed considerable damage, resulting in complete loss of vitality in 15% for a temperature rise of 5.5°C. In this study, a temperature rise of that size was achieved over a 40 s polymerization time temperature. A significant part of the polymerization takes place between 10 and 20 s, so the highest temperature rise was observed at 10-20 s.
Curing of composite resins increases dentin temperature through the exothermic resin polymerization process and the energy absorbed during light curing. The rate of exothermic polymerization reaction and maximum temperature rise during the process is proportional to the irradiance of the LED unit, the chemical structure of the composite resin, and the light conduction properties of the composite resin.[20] Strang et al.,[21] reported that light source is more important than exothermic reaction, while Masutani et al.,[22] maintained the opposite. Although dentin has relatively low thermal conductivity, there is a greater risk for pulp injury in deep cavities in which there is a thin layer of residual dentin, with increased number and permeability of dentin tubules. As a result, irritation of the pulp due to heat depends on the extent and duration of the temperature rise.[17] Knezevic et al.,[23] reported that the temperature rise increases as the material thickness decreases. Shortall and Harrington[24] and da Silva et al.,[25] concluded that the light attenuating ability of the material exceeds the effect of exothermic polymerization reaction at the base of the cavity floor.
When the glass and polyethylene fibers we installed in single and double layers on the cavity floor were compared with the control group, although there was some change in temperature rise values, no statistically significant difference was observed. Further studies are needed on the subject of the use of fibers as thermal insulation material.
CONCLUSION
The addition of polyethylene and glass fiber to resin composite does not affect temperature rise significantly. Temperature rise in all groups determined was not critical for pulpal health, although clinicians need to note temperature rises during polymerization.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Baldissara P, Catapano S, Scotti R. Clinical and histological evaluation of thermal injury thresholds in human teeth: A preliminary study. J Oral Rehabil. 1997;24:791–801. doi: 10.1046/j.1365-2842.1997.00566.x. [DOI] [PubMed] [Google Scholar]
- 2.Ayub KV, Santos GC, Jr, Rizkalla AS, Bohay R, Pegoraro LF, Rubo JH, et al. Effect of preheating on microhardness and viscosity of 4 resin composites. J Can Dent Assoc. 2014;80:e12. [PubMed] [Google Scholar]
- 3.Nammour S, Zeinoun T, Bogaerts I, Lamy M, Geerts SO, Bou Saba S, et al. Evaluation of dental pulp temperature rise during photo-activated decontamination (PAD) of caries: An in vitro study. Lasers Med Sci. 2010;25:651–4. doi: 10.1007/s10103-009-0683-2. [DOI] [PubMed] [Google Scholar]
- 4.Peutzfeldt A. Resin composites in dentistry: The monomer systems. Eur J Oral Sci. 1997;105:97–116. doi: 10.1111/j.1600-0722.1997.tb00188.x. [DOI] [PubMed] [Google Scholar]
- 5.Hussey DL, Biagioni PA, Lamey PJ. Thermographic measurement of temperature change during resin composite polymerization in vivo . J Dent. 1995;23:267–71. doi: 10.1016/0300-5712(95)91149-h. [DOI] [PubMed] [Google Scholar]
- 6.Belli R, Petschelt A, Lohbauer U. Thermal-induced residual stresses affect the fractographic patterns of zirconia-veneer dental prostheses. J Mech Behav Biomed Mater. 2013;21:167–77. doi: 10.1016/j.jmbbm.2012.10.022. [DOI] [PubMed] [Google Scholar]
- 7.Atai M, Motevasselian F. Temperature rise and degree of photopolymerization conversion of nanocomposites and conventional dental composites. Clin Oral Investig. 2009;13:309–16. doi: 10.1007/s00784-008-0236-2. [DOI] [PubMed] [Google Scholar]
- 8.Civjan S, Barone JJ, Reinke PE, Selting WJ. Thermal properties of nonmetallic restorative materials. J Dent Res. 1972;51:1030–7. doi: 10.1177/00220345720510040701. [DOI] [PubMed] [Google Scholar]
- 9.Guiraldo RD, Consani S, Consani RL, Berger SB, Mendes WB, Sinhoreti MA, et al. Comparison of silorane and methacrylate-based composite resins on the curing light transmission. Braz Dent J. 2010;21:538–42. doi: 10.1590/s0103-64402010000600010. [DOI] [PubMed] [Google Scholar]
- 10.Ilday N, Seven N. The influence of different fiber-reinforced composites on shear bond strengths when bonded to enamel and dentin structures. J Dent Sci. 2011;6:107–15. [Google Scholar]
- 11.Rappelli G, Putignano A. Tooth splinting with fiber-reinforced composite materials: Achieving predictable aesthetics. Pract Proced Aesthet Dent. 2002;14:495–500. [PubMed] [Google Scholar]
- 12.Kumbuloglu O, Aksoy G, User A. Rehabilitation of advanced periodontal problems by using a combination of a glass fiber-reinforced composite resin bridge and splint. J Adhes Dent. 2008;10:67–70. [PubMed] [Google Scholar]
- 13.Freudenthaler JW, Tischler GK, Burstone CJ. Bond strength of fiber-reinforced composite bars for orthodontic attachment. Am J Orthod Dentofacial Orthop. 2001;120:648–53. doi: 10.1067/mod.2001.118779. [DOI] [PubMed] [Google Scholar]
- 14.Seefeld F, Wenz HJ, Ludwig K, Kern M. Resistance to fracture and structural characteristics of different fiber reinforced post systems. Dent Mater. 2007;23:265–71. doi: 10.1016/j.dental.2006.01.018. [DOI] [PubMed] [Google Scholar]
- 15.Fanibunda KB. Thermal conductivity of normal and abnormal human dentine. Arch Oral Biol. 1975;20:457–9. doi: 10.1016/0003-9969(75)90233-2. [DOI] [PubMed] [Google Scholar]
- 16.Guiraldo RD, Consani S, Lympius T, Schneider LF, Sinhoreti MA, Correr-Sobrinho L. Influence of the light curing unit and thickness of residual dentin on generation of heat during composite photoactivation. J Oral Sci. 2008;50:137–42. doi: 10.2334/josnusd.50.137. [DOI] [PubMed] [Google Scholar]
- 17.Pereira Da Silva A, Alves Da Cunha L, Pagani C, De Mello Rode S. Temperature rise during adhesive and composite polymerization with different light-curing sources. Minerva Stomatol. 2010;59:253–8. [PubMed] [Google Scholar]
- 18.Kuo WC, Chang YH, Lin CL, Kuo JS. Effects of different ceramic and dentin thicknesses on the temperature rise during photocuring. J Dent Sci. 2011;6:210–5. [Google Scholar]
- 19.Zach L, Cohen G. Pulp response to externally applied heat. Oral Surg Oral Med Oral Pathol. 1965;19:515–30. doi: 10.1016/0030-4220(65)90015-0. [DOI] [PubMed] [Google Scholar]
- 20.El-Mowafy O, El-Badrawy W, Wasef M, Omar H, Kermanshahi S. Efficacy of new LED light-curing units in hardening of Class II composite restorations. J Can Dent Assoc. 2007;73:253. [PubMed] [Google Scholar]
- 21.Strang R, Patterson CJ, McLundie AC, Cummings A, Smail SR. In vitro temperature rises produced by five polymerising light sources. Restorat Dent. 1988;4:33–5. [PubMed] [Google Scholar]
- 22.Masutani S, Setcos JC, Schnell RJ, Phillips RW. Temperature rise during polymerization of visible light-activated composite resins. Dent Mater. 1988;4:174–8. doi: 10.1016/s0109-5641(88)80059-9. [DOI] [PubMed] [Google Scholar]
- 23.Knezevic A, Sariri K, Sovic I, Demoli N, Tarle Z. Shrinkage evaluation of composite polymerized with LED units using laser interferometry. Quintessence Int. 2010;41:417–25. [PubMed] [Google Scholar]
- 24.Shortall AC, Harrington E. Temperature rise during polymerization of light-activated resin composites. J Oral Rehabil. 1998;25:908–13. doi: 10.1046/j.1365-2842.1998.00336.x. [DOI] [PubMed] [Google Scholar]
- 25.da Silva EM, Penelas AG, Simao MS, Filho JD, Poskus LT, Guimaraes JG. Influence of the degree of dentine mineralization on pulp chamber temperature increase during resin-based composite (RBC) light-activation. J Dent. 2010;38:336–42. doi: 10.1016/j.jdent.2009.12.007. [DOI] [PubMed] [Google Scholar]