

Abstract
Aim:
The purpose of this study was to determine the root form and canal configuration in maxillary first premolars.
Materials and Methods:
A total of 250 extracted human adult maxillary first premolar teeth from North Indian population were collected. Access cavities were prepared and the coronal pulp tissue was extirpated. The samples were stored in 5% nitric acid solution for 5 days. They were then rinsed, dried, and dehydrated using increasing concentrations of ethanol (70, 80, and 95%) successively for 1 day. Teeth were rendered transparent by immersing in methyl salicylate. India ink was then injected. The root canal morphology was examined under stereomicroscope.
Result:
53.6% were single rooted followed by fused root form followed by two root form. 0.4% had three rooted maxillary first premolar. Variable root canal configurations were also found. Type IV configuration was most prevalent (33.2%). Two teeth showed an additional configuration. Lateral canals were present in 34.8% of the samples and intercanal communications in 16%.
Conclusion:
Within the limitations of this study, it was concluded that in North Indian population, there was an increased propensity for types IV, I, II, and III canal morphologies in maxillary first premolars. Single root form was most common.
Keywords: Canal morphology, clearing technique, dehydration, demineralization, demineralization and maxillary first premolars, methyl Salicylate, nitric acid
INTRODUCTION
A root with a graceful tapering canal and single foramina is the exception rather than the rule. Any attempt to perform endodontic therapy must be preceded with a thorough understanding of the anatomy of both the pulp chamber and the root canal system.[1] The risk of missing anatomy during root canal treatment is high because of the complexity of the root canal system[2] and may lead to endodontic failure.
A thorough knowledge of root canal morphology is essential for successful endodontic therapy.[3,4] Numerous factors contribute to the variations found in root canal studies including ethnicity,[5] age,[6] gender,[7] and study design.[8]
The maxillary first premolars are among the most difficult teeth to be treated endodontically due to their variation in number of roots, canal configuration, the direction and longitudinal depressions of the roots, and various pulp cavity configurations.[9]
In previous studies,[9,10] the prevalence of one root in these teeth varied from 15.5 to 60%; two roots, 40-80.9%; and three roots, 0-9.2%.[11] The canal morphology of the maxillary first premolar teeth has been reported with varying prevalence rates: One canal, 0-26.2%; two canals, 73.3-97%; and three canals, 0.5-9.2%.[9,12] Thus, it is evident that the anatomy of these teeth tends to have racial variations.
Different methods have been used to investigate tooth morphology like tooth decalcification and dye injection, sectioning of the teeth and radiographic studies in vitro,[12] alternative radiographic techniques,[13] and radiographic assessment enhanced with contrast media.[14] Current literature shows that where atypical anatomy is suspected, modern radiographic techniques like spiral computed tomography and micro-computed tomography are highly helpful in making a proper diagnosis as they offer noninvasive reproducible techniques for three-dimensional assessment of root canal system.[15,16] Despite their accuracy, these modern radiographic techniques involve expensive equipment. In the present study, clearing technique was used.[17] It enabled viewing of a three-dimensional morphology of roots and canals without altering the internal shape of pulp cavity or direction of the canals. This procedure was chosen for our study as it is relatively simple, inexpensive, and acceptable. It also has a low incidence of error.[9]
Information on the root and canal morphology of maxillary first premolar teeth from populations of indigenous Indians is scarce and till date there is no published data on root canal morphology of North Indian maxillary first premolars; therefore, the aim and purpose of this study is to assess root form and canal morphology of maxillary first premolars in a North Indian population using clearing technique.
MATERIALS AND METHODS
A total of 250 extracted human adult maxillary first premolar teeth from various parts of North India were collected. Teeth with fracture, metallic restorations, deep caries, and incompletely formed roots were excluded. The maxillary first premolars were distinguished from maxillary second premolars as the buccal cusp, almost the same size as palatal cusp in maxillary second premolar; whereas in first it is longer, mesial surface of the root of first premolar has a developmental depression. Calculus and stains were removed using an ultrasonic scaler. The samples were then stored in 5.25% sodium hypochlorite (Fisher Scientific Qualigens Fine Chemicals, Navi Mumbai, India) for 30 min for the removal of organic debris and then in 10% formalin (Formoa Cresol Pharmadent Remedies Pvt Ltd, Vadodara, Gujarat, India) until use and then the teeth were cleaned under running water. Access cavities were prepared using a no. 2 round bur and the coronal pulp tissue was extirpated in the canal orifices. The samples were stored in 5% nitric acid solution (Nitric Acid, Fisher Scientific, Thermo Fisher Scientific India Pvt Ltd, Godrej Coliseum,101A-101B, Mumbai, India) for 5 days.[16] The solution was changed each day. Demineralization was assessed by insertion of needle in the crown and by periodic radiographs. The samples were then rinsed under running water to remove traces of nitric acid, dried, and dehydrated using increasing concentrations of ethanol (70, 80, and 95%; Absolute Alcohol A R Quality Eastways Park, William, Essesx, CM83YE, England) successively for 1 day. Finally, the teeth were rendered transparent by immersing in methyl salicylate (methyl salicylate (for synthesis), Loba Chemie Pvt Ltd, 107 Wodahouse Road, Mumbai, India). At the end of the 3rd day, complete transparency was achieved. India ink (Indian Ink, Loba Chemie Laboratory Reagents and Fine Chemicals, Mumbai, India) was injected into the root canals of transparent teeth using syringes with 27 gauge needle (DispoVan Hindustan Syringes and Medical Devices Ltd, Ballabgarh, Faridabad, India).
After the ink had dried, root canal morphology was examined under stereomicrosope (Olympus; zoom type).
The following observations were made:
-
Number of roots,
Group I: One root form.
Group II: Two root form.
Group III: Fused root form.
Group IV: Three root form.
Type of root canals,
Presence and location of lateral canals and intercanal communications,
Location of apical foramina
The canal configuration will be categorized into the eight types of Vertucci's classification (1984) as follows:
Type 1: A single canal present from the pulp chamber to the apex;
Type 2: Two separate canals leave the pulp chamber and join short of the apex to form one canal;
Type 3: One canal leaves the pulp chamber, divides into two within the root, and then merges to exit in one canal;
Type 4: Two separate and distinct canals are present from the pulp chamber to the apex;
Type 5: Single canal leaves the pulp chamber, but divides into two separate canals with two separate apical foramina;
Type 6: Two separate canals leave the pulp chamber, but join at the midpoint and divides again into two separate apical foramina;
Type 7: One canal leaves the pulp chamber, divides and rejoins within the canal, and finally redivides into two distinct canals short of the apex; and
Type 8: Three separate distinct canals extent from the pulp chamber to the apex.
OBSERVATIONS AND RESULTS
[Figures 1, 2 and Tables 1, 2]
Figure 1.
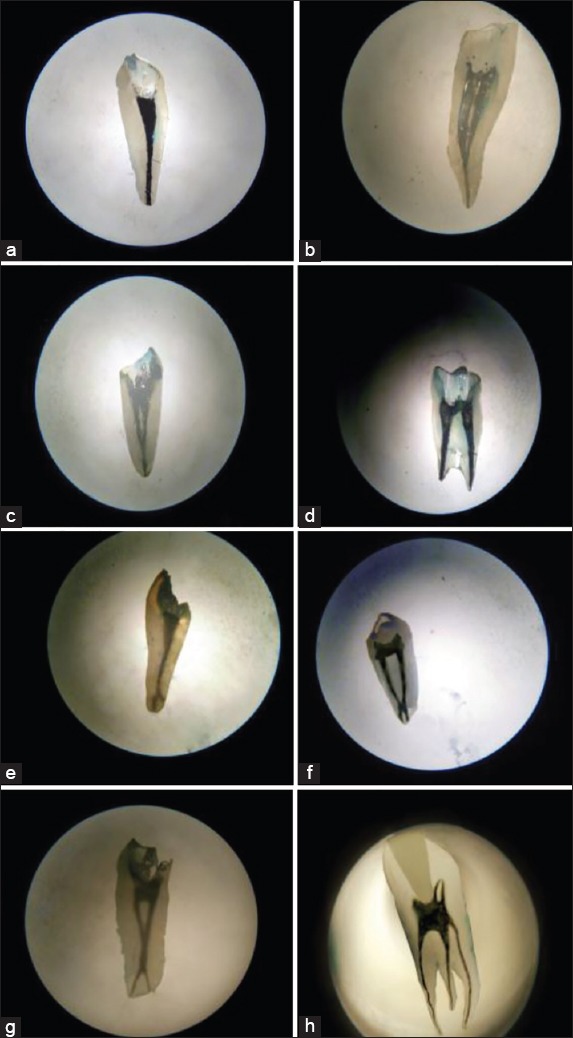
(a) Vertucci's canal classification type I (1), (b) Vertucci's canal classification type II (2-1), (c) Vertucci's canal classification type III (1-2-1), (d) Vertucci's canal classification type IV (2), (e) Vertucci's canal classification type V (1-2), (f) Vertucci's canal classification type VI (2-1-2), (g) Vertucci's canal classification type VII (1-2-1-2), and (h) Vertucci's canal classification type VIII (3)
Figure 2.
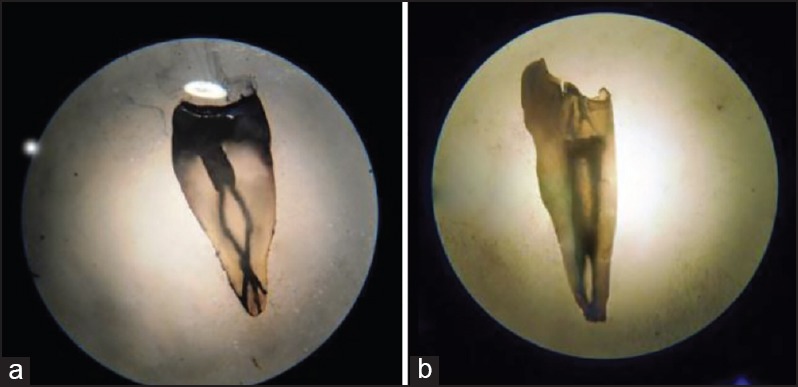
(a) Sert and Bayirli's canal classification type XIII (1-2-1-3) and (b) Sert and Bayirli's canal classification type XIX (2-1-2-1)
Table 1.
Canal morphology, root form, and lateral canals and intercanal communications
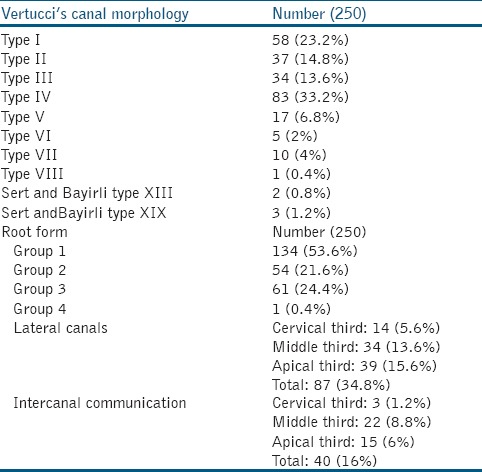
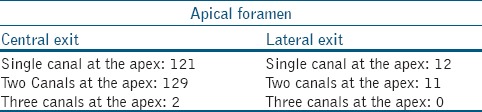
Table 2.
Location of apical foramen
Theory of results
Of the 250 studied maxillary first premolars, 53.6% were single rooted followed by fused root form (24.4%); followed by two root form in 21.6% samples. Only 0.4% had three rooted maxillary first premolar.
Type IV configuration was most prevalent (33.2%), followed by type I (23.2%), type II (14.8%), type III (13.6%), type V (6.8%), type VII (4%), type VI (2%), and type VIII (0.4%). Two teeth showed an additional configuration; Sert and Bayirli's type XIX (2-1-2-1) and another exhibited Sert and Bayirli's type XIII (1-2-1-3).
Lateral canals were present in 34.8% of the samples; apical third (15.6%)> middle third (13.6%)> cervical third (5.6%). Intercanal communications were present in 16% of the samples; middle third (8.8%)> apical third (6%)> cervical third (1.2%).
Out of all the canals; canals exiting in single foramina were 48.4%; whereas, 50.8% exited in two separate foramen. Only in 0.8%, three apical foramen were present.
DISCUSSION
In the past, various methods have been employed to study root canal morphologies.[17,18,19,20,21,22,23,24] It has been reported in the literature that ex vivo demineralization and staining provides the most detailed information, while maintaining the original form and relations of canals.[25] It also provides a three-dimensional view of the canal. The inorganic constituents of the tooth are first dissolved by decalcification; water, air, and lipid components are removed by dehydration; and by subsequent immersion in the clearing agents.[24] Five percent nitric acid used as a decalcifying agent is rapid in its action, causing little damage to the tissue if the time of decalcification is controlled rapidly. After fixation in aqueous solutions, tooth tissue needs to be dehydrated slowly in order to prevent high degree of shrinkage due to the rapid removal of water. Then the dehydrating agent is replaced by methyl salicylate, which renders the tooth transparent as the clearing agent increases the refractive index of the tooth.[24,26] In this study, the use of stereomicroscope for viewing the root canal pattern resulted in higher magnification.
The maxillary first premolars are among the most difficult teeth to be treated endodontically due to their variation in number of roots, canal configuration, the direction and longitudinal depressions of the roots, and various pulp cavity configurations;[9] therefore, maxillary first premolars were chosen for the study. Also till date only one Indian study on maxillary first premolars with limited data is reported in the literature.
Single roots, two roots, and three roots have been identified in maxillary first premolars, with the number of canals ranging from one to three per root.[12] The number and morphology of roots of Indian first premolars differ from those of Mongoloid first premolars, in which three roots are reported to be rare.[10] Though only a small percentage of the number of teeth studied were three rooted, it is important to consider this variation in the clinical scenario.
The literature suggests that the occurrence of three canals in these teeth may vary from 0.5 to 7.5%.[12] Vertucci[27] reported that maxillary first premolar was the only tooth which had all the eight types of canal configurations. This was in accordance with our study in which all eight types of canal configurations as well as two rare Sert and Bayirli's canal configurations (types XIII and XIX) were also found.
In the present study, 53.6% of the first maxillary premolars had one root; similar to Brazilian population where the reported incidence was 55.8%.[9] Prevalence of 21.6% of two rooted samples was recorded in the present study, which is lower than values observed in other populations.[10] The differences between the results of these morphology studies may be related to variations of examination methods, classification systems, sample sizes, and ethnic background of tooth sources.[16]
We found 33.2% of all the samples had Vertucci's type IV canal configuration followed by Vertucci's type I canal configuration (23.2%). This was in accordance with Vertucci's study, where type IV canal configuration was most common in maxillary first premolars.[27]
The occurrence of lateral canals was observed in the study and was found to be34.8% with maximum number noted in the apical third. (15.6%) This was in accordance with text book of endodontics, where maximum incidence of lateral canals was in the apical third of the root.[28] This variance rarely, if ever, causes an endodontic failure. When they harbor inflamed and/or infected material, they may cause pain during endodontic treatment. They may simulate periodontal disease and may cause problems with treatment if present when a tooth is left open for drainage. Periodontal disease may cause pulp exposure via lateral canals located coronally.[29]
Intercanal communication or transverse anastomoses/isthmus was present in 16% of the samples with maximum being in the middle third. (8.8%) This was in accordance with textbook of endodontics, where maximum incidence intercanal communication was in the middle third of the root.[28] An isthmus is a narrow, ribbon-shaped communication between two root canals that contains pulp or pulpally derived tissue. It functions as a bacterial reservoir.[29] Literature has reported a high percentage of intercanal communications in teeth with two canals. This communication is of clinical significance as it may be difficult to debride and fill it adequately.[29]
The location of apical foramen is of clinical significance during working length determination, which often depends on the average position of the apical constriction relative to the root apex.[29]
Our study showed that the root and canal morphology of North Indian maxillary first premolars is highly variable.
CONCLUSION
Under the limitations of this study, it was concluded that in North Indian population, there was an increased propensity for types IV, I, II, and III canal morphologies in maxillary first premolars. The finding of additional canal configurations, type XIX (2-1-2-1) and type XIII (1-2-1-3), are rare but should be kept in mind when performing endodontic therapy for these teeth.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Deepak S, Meetu M. A computed tomographic study of canal variation in maxillary and mandibular first premolar teeth in Jaipur population: An in vitro study. People's J Scientific Res. 2011;4:1–5. [Google Scholar]
- 2.Mittal S, Kumar T, Mittal S, Sharma J. Mandibular premolars with aberrant canal morphology: An endodontic challenge. J Conserv Dent. 2014;17:491–4. doi: 10.4103/0972-0707.139851. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Reuben J, Velmurugan N, Kandaswamy D. The evaluation of root canal morphology of the mandibular first molar in an Indian population using spiral computed tomography scan: An in vitro study. Int Endod J. 2011;44:990–9. doi: 10.1016/j.joen.2007.11.018. [DOI] [PubMed] [Google Scholar]
- 4.Cleghorn B, Christie W, Dong C. Root and canal morphology of the human mandibular first premolar: A literature review. J Endod. 2007;33:509–16. doi: 10.1016/j.joen.2006.12.004. [DOI] [PubMed] [Google Scholar]
- 5.Gulabivala K, Aung TH, Alavi A, Ng YL. Root and canal morphology of Burmese mandibular molars. Int Endod J. 2001;34:359–70. doi: 10.1046/j.1365-2591.2001.00399.x. [DOI] [PubMed] [Google Scholar]
- 6.Neaverth EJ, Kotler LM, Kaltenbaoh RF. Clinical investigation (in vivo) of endodontically treated maxillary first molars. J Endod. 1987;13:506–12. doi: 10.1016/S0099-2399(87)80018-3. [DOI] [PubMed] [Google Scholar]
- 7.Sert S, Bayirli GS. Evaluation of the root canal configuration of the mandibular and maxillary permanent teeth by gender in the Turkish population. J Endod. 2004;30:391–8. doi: 10.1097/00004770-200406000-00004. [DOI] [PubMed] [Google Scholar]
- 8.Awawdeh L, Abdullah H, Al-Qudah A. Root form and canal morphology of Jordanian maxillary first premolars. J Endod. 2008;34:391–8. doi: 10.1016/j.joen.2008.04.013. [DOI] [PubMed] [Google Scholar]
- 9.Pecora JD, Saquy PC, Sousa Neto ND, Woelfel JB. Root form and canal anatomy of maxillary first premolars. Braz Dent J. 1991;2:87–94. [PubMed] [Google Scholar]
- 10.Loh HS. Root morphology of maxillary first premolar in Singaporeans. Aust Dent J. 1998;43:399–402. doi: 10.1111/j.1834-7819.1998.tb00199.x. [DOI] [PubMed] [Google Scholar]
- 11.Lipski M, Woźniak K, Łagocka R, Tomasik M. Root and canal morphology of the first human maxillary premolar. Durham Anthropol J. 2003;12:2–3. [Google Scholar]
- 12.Pineda F, Kuttler Y. Mesiodistal and buccolingual roentogenic investigations of 7,275 root canals. Oral Surg. 1972;33:101–10. doi: 10.1016/0030-4220(72)90214-9. [DOI] [PubMed] [Google Scholar]
- 13.Patel S, Dawood A, Whaites E, Pitt Ford T. New dimensions in endodontic imaging: Part 1. Conventional and alternative radiographic systems. Int Endod J. 2009;42:447–62. doi: 10.1111/j.1365-2591.2008.01530.x. [DOI] [PubMed] [Google Scholar]
- 14.Scarfe WC, Fana CR, Farman AG. Radiographic detection of accessory/lateral canals: Use of radiovisiography and hypaque. J Endod. 1995;21:185–90. doi: 10.1016/S0099-2399(06)80563-7. [DOI] [PubMed] [Google Scholar]
- 15.Plotino G, Grande NM, Pecci R, Bedini R, Pameijer CH, Somma F. Three dimensional imaging using microcomputed tomography for studying tooth macro-morphology. J Am Dent Assoc. 2006;137:1555–61. doi: 10.14219/jada.archive.2006.0091. [DOI] [PubMed] [Google Scholar]
- 16.Sberna MT, Rizzo G, Zachhi E, Capparè P, Rubinacci A. A preliminary study of the use of peripheral quantitative computed tomography for investigating of the root canal anatomy. Int Endod J. 2009;42:66–75. doi: 10.1111/j.1365-2591.2008.01452.x. [DOI] [PubMed] [Google Scholar]
- 17.Boruah LC, Bhuyan AC. Morphologic characteristics of root canal of mandibular incisors in North-East Indian population: An in-vitro study. J Conserv Dent. 2011;14:346–50. doi: 10.4103/0972-0707.87195. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Kaffe I, Kaufman A, Littner MM, Lazarson A. Radiographic study of root canal system of mandibular anterior teeth. Int Endod J. 1985;18:253–9. doi: 10.1111/j.1365-2591.1985.tb00452.x. [DOI] [PubMed] [Google Scholar]
- 19.Robertson D, Leeb J, McKee M, Brewer E. A clearing technique for the study of root canal systems. J Endod. 1980;6:421–4. doi: 10.1016/S0099-2399(80)80218-4. [DOI] [PubMed] [Google Scholar]
- 20.Sampire HN, Hartwell GR. Frequency of second mesiobuccal canals in maxillary molars as determined by use of an operating microscope: A clinical study. J Endod. 2000;26:673–4. doi: 10.1097/00004770-200011000-00010. [DOI] [PubMed] [Google Scholar]
- 21.Reuben J, Velmurugan N, Kandaswamy D. The evaluation of root canal morphology of the mandibular first molar in an Indian population using spiral computed tomography scan: An in vitro study. J Endod. 2008;34:121–249. doi: 10.1016/j.joen.2007.11.018. [DOI] [PubMed] [Google Scholar]
- 22.Neelakantan P, Subbaro C, Ahuja R, Subbaro CV, Guttman JL. Cone-beam computed tomography study of root and canal morphology of maxillary first and second molars in an Indian population. J Endod. 2010;36:1622–7. doi: 10.1016/j.joen.2010.07.006. [DOI] [PubMed] [Google Scholar]
- 23.Zheng QH, Wang Y, Zhou XD, Wang Q, Zheng GN, Huang DM. A cone-beam computed tomography study of maxillary first permanent molar root and canal morphology in a Chinese population. J Endod. 2010;36:1480–4. doi: 10.1016/j.joen.2010.06.018. [DOI] [PubMed] [Google Scholar]
- 24.Shivapathasundharam B, Berti AE. Transparent tooth model system. An aid in the study of root canal anatomy. Indian J Dent Res. 2000;11:89–94. [PubMed] [Google Scholar]
- 25.Vertucci FJ. Root canal morphology and its relationship in endodontic procedures. Endod Top. 2005;10:3–29. [Google Scholar]
- 26.Culling CF. 3rd ed. Great Britain: Butterworth and Co Ltd; 1974. Handbook of histopathological and histochemical techniques; pp. 63–77. [Google Scholar]
- 27.Vertucci FJ, Gegauff A. Root canal morphology of the maxillary first premolar. J Am Dent Assoc. 1979;99:194–8. doi: 10.14219/jada.archive.1979.0255. [DOI] [PubMed] [Google Scholar]
- 28.Hargreaves KM, Cohen S. 10th ed. Louis Missouri: Mosby Elsevier St; 2011. Pathways of the pulp. Chapter 7 Tooth morphology and access cavity preparation; p. 139. [Google Scholar]
- 29.Weine FS. The enigma of the lateral canal. DCNA. 1984;28:833–52. [PubMed] [Google Scholar]