

Abstract
Background
Radiation treatment with simultaneous integrated boost against suspected lymph node metastases may be a curative therapeutic option in patients with high-risk prostate cancer (>15% estimated risk of pelvic lymph node metastases according to the Cagiannos nomogram). 11C-acetate positron emission tomography/computed tomography (PET/CT) can be used for primary staging as well as for detection of suspected relapse of prostate cancer. The aims of this study were to evaluate the association between positive 11C-acetate PET/CT findings and the estimated risk of pelvic lymph node metastases and to assess the impact of 11C-acetate PET/CT on patient management in high-risk prostate cancer patients.
Methods
Fifty consecutive prostate cancer patients referred for primary staging with 11C-acetate PET/CT prior to radiotherapy with curative intention were enrolled in this retrospective study.
Results
All patients showed increased 11C-acetate uptake in the prostate. Pelvic lymph node uptake was seen in 42% (21/50) of the patients, with positive external iliac lymph nodes in 71% (15/21) of these. The overall observed proportion of PET/CT-positive pelvic lymph nodes at patient level was higher than the average estimated risk, especially in low-risk groups (<15%). There was a significant association between observed proportion and estimated risk of pelvic lymph node metastases in groups with ≤45 and >45% estimated risk. Treatment strategy was altered due to 11C-acetate PET/CT findings in 43% (20/47) of the patients.
Conclusions
The observed proportion of 11C-acetate PET/CT findings suggestive of locoregional metastases was higher than the estimated risk, suggesting that the Cagiannos nomogram underestimates the risk for metastases. The imaging results with 11C-acetate PET/CT have a considerable impact on patient management.
Keywords: Prostatic neoplasms, PET/CT, 11C-acetate, Neoplasm staging, Lymphatic metastasis
Background
During a lifetime, approximately 15% of men will be diagnosed with prostate cancer, making it the second most common cancer form in males worldwide [1]. According to the Swedish National Prostate Cancer Registry, it is the most common cancer in males in Sweden, with an incidence of approximately 10,000 and a mortality of 2,500 annually [2]. Prostate cancer is a complex heterogeneous disease with highly variable morphological and physiological characteristics [3]. Staging and risk categorisation is decided from clinical features including T stage, prostate-specific antigen (PSA) and Gleason score. Risk estimation can be facilitated with the use of nomograms such as the Cagiannos nomogram, which is a widely used clinical tool to determine the extent of disease as well as the risk of pelvic lymph node involvement [4]. Prostate cancer with >15% estimated risk of pelvic lymph node metastases is considered as high-risk prostate cancer but still stands a chance to get cured with standard radiotherapy including the prostate and the seminal vesicles (78 Gy) [5]. However, a more aggressive treatment approach including the pelvic lymph nodes is under development [5] and is used in the treatment of high-risk prostate cancer in the University Hospital of Umeå. Nomograms will only provide an estimated risk of pelvic lymph node metastasis, and it is necessary to establish a more reliable non-invasive method for staging. Hybrid imaging with positron emission tomography/computed tomography (PET/CT) renders various molecular and morphological information, depending on the radiotracer and the design of the CT protocol. PET/CT is widely used in oncologic imaging for cancer staging and restaging as well as for evaluation of treatment response. The most used radiotracer 18F-FDG (2-deoxy-2-[18F]-d-glucose) is an indicator of glucose metabolism, which has proved useful in several malignant tumours due to their increased glycolysis, the Warburg effect [6], but it has limitations in relatively slow-growing malignancies such as prostate cancer. For PET/CT imaging in prostate cancer, 11C-acetate, 11C-choline, and 18F-choline appear to be more suitable tracers [7]. Multiple other promising new tracers are under development for imaging in prostate cancer but still need further investigation [8,9]. Currently, 11C-/18F-choline and 11C-acetate are the most commonly used tracers, with comparable results [7,10]. A recent study by Buchegger et al. showed excellent concordance between 18F-choline and 11C-acetate in the detection and localization of positive lymph nodes and skeletal metastases in patients with prostate cancer [10]. 11C-choline-PET/CT has proved valuable mainly for radiotherapy planning in prostate cancer patients with biochemical recurrence after radical treatment [11]. 11C-acetate is a radiotracer that is believed to reflect lipid metabolism, but its exact pharmacodynamic mechanism is still debated [12]. Several studies indicate that 11C-acetate is of value for primary staging of prostate cancer [8,13–15]. Oyama et al. have shown 11C-acetate to be superior to 18F-FDG with higher sensitivity for prostate cancer and its metastases [13]. In 2012, Castellucci and Jadvar suggested in a review of PET/CT in prostate cancer that the main application for 11C-acetate might be to rule out distant metastases in early prostate cancer relapse prior to salvage radiotherapy [8].
The aims of this retrospective study were to evaluate the correlation between 11C-acetate PET/CT findings and the estimated risk of locoregional lymph node metastases as indicated by the Cagiannos nomogram and to assess the impact of 11C-acetate PET/CT examination results on the clinical management of previously untreated high-risk prostate cancer patients.
Methods
Patients and clinical data
Fifty consecutive patients referred for 11C-acetate PET/CT at Nuclear Medicine, Department of Radiology, University Hospital of Umeå, Sweden, from 2011 July 6 to 2013 March 26 were included. The cause for referral was primary staging of biopsy-verified prostate cancer prior to radiotherapy with curative intention. Patients were referred for 11C-acetate PET/CT if they reached 15% risk in the nomogram or if they exhibited other risk factors such as rapidly increasing PSA. The time interval between biopsy and 11C-acetate PET/CT was at an average of 8 weeks, range 3 to 18 weeks. All patients had a baseline 11C-acetate PET/CT scan, of which 90% (45/50) had a contrast-enhanced CT (CECT) scan in the same session. The remaining five patients had a diagnostic CT scan without intravenous (i.v.) contrast due to either impaired renal function or a previous examination with i.v. iodine contrast media within 4 weeks.
Clinical information regarding pre-treatment status was retrieved from the referral text. Follow-up data were collected from the patients' medical records. Clinical data concerning changes in treatment strategy were missing in three patients referred from regional hospitals, and these patients were excluded from the evaluation of impact of 11C-acetate PET/CT findings on treatment strategy. The study was approved by the regional ethics review board.
The Cagiannos pre-treatment nomogram was used to estimate the risk of pelvic lymph node involvement. Factors taken into account in the nomogram are age, pre-treatment PSA, clinical tumour stage, primary and secondary Gleason grade, and the number of positive and negative biopsy cores [16]. Estimated risk data could be calculated for all patients except one, where clinical data were missing. This patient was excluded from the evaluation of the correlation between 11C-acetate PET/CT findings and the estimated risk of locoregional lymph node metastases. Patient characteristics are shown in detail in Table 1.
Table 1.
Patient characteristics
| n | Mean | Range | |
|---|---|---|---|
| Patients (n) | 50 | ||
| Age (years) | 67 | 41 to 77 | |
| PSA (ng/ml) | 37 | 2.7 to 168 | |
| Gleason score | 8 | 6 to 10 | |
| Estimated risk of locoregional lymph node metastases (%)a | 32 | 3.3 to 80.3 |
aAccording to the Cagiannos pre-treatment nomogram, where age, pre-treatment PSA, clinical tumour stage, primary and secondary Gleason grade, and the number of positive and negative biopsy cores influence the estimated risk.
PET/CT imaging
All image acquisition was done with a GE Discovery 690 PET/CT scanner (General Electric, Pewaukee, WI, USA). Software and algorithms were supplied with the scanner. The patients were injected with 1-[11C]-acetate (5.0 MBq/kg body weight, mean dose 436 MBq, range 304 to 577 MBq) i.v., and a CT scan with low dose for PET attenuation was acquired, followed by a PET scan 10 min post-injection and finally a diagnostic CT with or without i.v. contrast media. The attenuation CT was a helical 0.5-s rotation time scan, employing 120 kV and 30 mA. The PET scan was performed in time-of-flight mode with an acquisition time of 2 min/bed position, including the abdomen, thorax and neck. The PET images were reconstructed with the OSEM-based VuePoint HD (GE Healthcare, Pewaukee, WI, USA) (2 iterations, 24 subsets, 6.4 mm Gaussian filter), to a 128 × 128 pixel matrix with 50-cm field-of-view, giving a voxel size of 5.5 × 5.5 × 3.27 mm3. The diagnostic CT included the neck, thorax and abdomen, using 120 kV, with beam current controlled by the Auto-mA algorithm (noise index 35, current limited to the range 150 to 750 mA). The CECT was done after i.v. injection of iodine contrast (Omnipaque 350 mgI/ml 0.5 g I/kg, rendering a patient mean volume of 137 ml, range 108 to 167 ml).
Evaluation of image data
Two physicians double licensed in radiology and nuclear medicine (one with >10 years' experience from reading PET/CT and one with 2 years' experience) visually evaluated all PET/CT studies. Any exceptional cases of inter-observer disagreement were solved with consensus. The radiologists had access to basic clinical data available in the referral text, typically length of disease, Gleason score and PSA levels. Lesions with acetate uptake visually exceeding the background activity were considered positive. The uptakes were quantified by measurements of the highest standardised uptake value - maximum pixel activity in correlation to body weight and the injected dose, grams per millilitre (standardised uptake value (SUVmax)). All visually positive uptakes were measured in box regions of interest (ROIs) with PET VCAR software (AW 4.5, General Electric, Pewaukee, WI, USA) to determine SUVmax. The mediastinal background was measured in reference ROIs. The ROIs were delineated with a threshold of 42% of maximum signal intensity [17,18].
The morphological criteria for suspected lymph node metastases were round shape, short-axis diameter exceeding 10 mm, lack of fat-containing hilus and visually increased contrast enhancement compared to normal lymph nodes.
Other suspected metastatic sites were skeletal and hepatic lesions. The morphological criteria for suspected bone metastasis on CT were sclerotic, lytic or mixed lesions with destruction of cortical bone. Characteristics consistent with suspected hepatic metastases on CT were hypo- or hyperattenuating hepatic masses with irregular delineation and/or pathologic pattern of contrast enhancement.
The distinction between low, intermediate and high grade of suspicion of lymph node metastasis was based on the combination of the level of SUVmax, morphological changes in size and structure and pathological contrast enhancement, according to generally defined and accepted criteria for evaluation of lymph node involvement in CT as well as in 18F-FDG PET studies. Low-grade suspicious lesions have been considered non-metastatic. Intermediate- and high-grade suspicious lesions have been evaluated as metastatic. The systematic interpretation of lymph nodes is described in detail in Tables 2 and 3. Depending on the level of SUVmax, also normal-appearing lymph nodes can be categorised as intermediate grade, and vice versa, morphologically aberrant lymph nodes with just a slight increase in SUVmax are categorised as high grade according to Tables 2 and 3. The high grade of suspicion requires both PET and CT changes, whereas in the intermediate group, the level of the SUVmax is the critical parameter. Pelvic locoregional lymph nodes and distant paraaortal lymph nodes were evaluated with slightly different criteria than other distant lymph nodes regarding the impact of the level of SUVmax, in order to reduce the number of false-positive reactive lymph nodes in the thorax and the inguinal regions, where prostate cancer metastases are less likely to occur (Tables 2 and 3). Paraaortal lymph node metastases per definition are considered distant metastases. Our division of lymph nodes into pelvic and paraaortal versus other distant lymph node metastases was due to anatomical reasons - the lymphatic drainage from the prostate makes it more likely to find metastases in the pelvic and paraaortal lymph nodes. Also, low-grade uptake in small mediastinal lymph nodes is a relatively common finding of unclear clinical significance, making these lymph nodes more difficult to interpret. The paraaortal lymph nodes were thus treated with higher degree of suspicion than other distant sites, with regard to likelihood of metastasis.
Table 2.
Criteria for low, intermediate, and high grade of suspicion of pelvic/paraaortal lymph node metastasis in PET/CT
| SUV max < mediastinal background | SUV max > mediastinal background | Any visually positive uptake on PET | Pathological appearance on CT | |
|---|---|---|---|---|
| Low grade | + | - | ||
| Intermediate grade | + | - | ||
| High grade | + | + |
Table 3.
Criteria for low, intermediate, and high grade of suspicion of distant (except for paraaortal) lymph node metastasis in PET/CT
| SUV max <50% higher than mediastinal background | SUV max >50% higher than mediastinal background | Any visually positive uptake on PET | Pathological appearance on CT | |
|---|---|---|---|---|
| Low grade | + | - | ||
| Intermediate grade | + | - | ||
| High grade | + | + |
Statistical analysis
Different risk groups regarding the estimated risk of locoregional lymph node metastases versus the observed risk were compared with Pearson's chi-square test. The association between prostate SUVmax, PSA and Gleason score, respectively, and the presence of metastatic disease was evaluated with binary logistic regression analysis. Correlations between prostate SUVmax, PSA and Gleason score were evaluated using linear regression analysis. For more reliable sample sizes, patients were merged into three Gleason score groups: Gleason score 6 to 7, 8 and 9 to 10. The chosen significance level was p <0.05. All statistical analyses were executed in IBM SPSS Statistics 21 (SPSS Inc., Chicago, IL, USA).
Results
Distribution of positive 11C-acetate PET/CT findings
All patients showed increased heterogeneous acetate uptake of the prostate (mean SUVmax 7.3 g/ml, range 3.3 to 13.8 g/ml); typical appearance is shown in Figure 1. Suspected lymph node metastases were seen in 105 lymph nodes in 42% (21/50) of the patients, most frequently along the external iliac vessels, which was the case in 71% (15/21) of the patients (typical uptake shown in Figure 2). In 45% (47/105) of the positive lymph nodes, only PET was positive, and in the other 55% (58/105), both PET and CT were pathologic. Distribution and characteristics of suspected locoregional lymph node metastases are shown in detail in Table 4.
Figure 1.
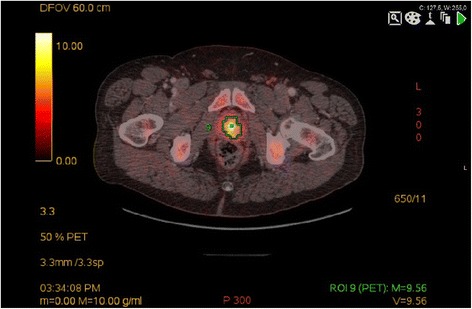
Increased acetate uptake (SUV max 9.6) of the prostate in patient with prostate cancer.
Figure 2.
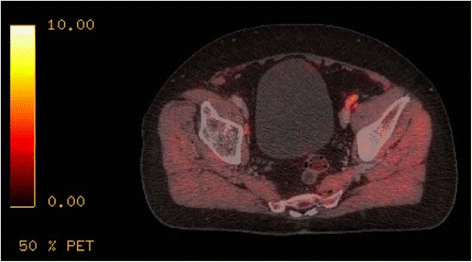
Increased acetate uptake in suspected iliac lymph node metastasis in a prostate cancer patient.
Table 4.
Distribution of total number of intermediate and high-grade suspicious locoregional lymph node uptakes, interpreted as metastatic
| Locoregional LN localisation | High-grade suspicious LN metastases (mean SUV max g/ml and mean short axis mm) | Intermediate suspicious LN metastases (mean SUV max g/ml) | Number of patients ( n =21) | ∑ suspicious LN metastases |
|---|---|---|---|---|
| Pararectal | 6 (5.4 g/ml, 20 mm) | 0 | 4 | 6 |
| Obturator | 6 (5.2 g/ml, 9.7 mm) | 2 (2.9 g/ml) | 6 | 8 |
| External iliac | 28 (6.6 g/ml, 14 mm) | 36 (3.9 g/ml) | 15 | 64 |
| Internal iliac | 11 (6.5 g/ml, 14 mm) | 4 (4.7 g/ml) | 9 | 15 |
| Common iliac | 7 (4.8 g/ml, 13 mm) | 5 (4.3 g/ml) | 6 | 12 |
| ∑ | 58 | 47 | 21a | 105 |
a21 patients with acetate uptakes in multiple locations.
Previously unknown distant metastases were found in 28% (14/50) of patients: located in paraaortal lymph nodes in six patients, mediastinal lymph nodes in eight and cervical lymph nodes in one patient (example shown in Figure 3). Among the 14 patients with suspected distant metastases were four with skeletal metastases. Unexpected incidental findings in two patients were biopsy-verified synchronous renal cell carcinoma and hepatocellular carcinoma. Distribution of suspected distant metastases and incidental findings are shown in detail in Table 5.
Figure 3.
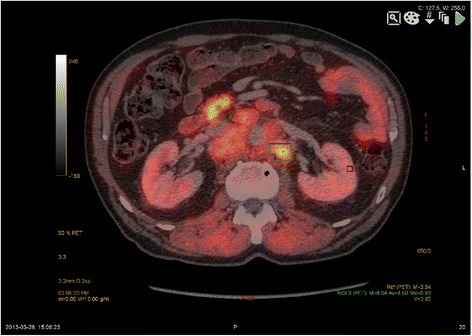
Increased acetate uptake in pathologically enlarged paraaortal lymph nodes in patient with prostate cancer.
Table 5.
Distribution of suspected distant metastases and incidental findings
| Localisation of suspected pathology | Number of PET + lesions | Number of CT + lesions | CT appearance | Pathology unrelated to prostate cancer | Number of patients | ∑ distant metastases |
|---|---|---|---|---|---|---|
| Paraaortal LN | 6 (mean SUVmax 5.8 g/ml) | 6 (mean short axis 13 mm) | Oval-rounded shape | 6 | 6 (4 solitary, 2 conglomerates) | |
| Mediastinal/hilar LN | 8 (mean SUVmax 3.7 g/ml) | 8 (mean short axis 10 mm) | Oval-rounded shape | 8 | 8 (6 solitary, 2 conglomerates) | |
| Axillary LN | 1 (SUVmax 9.0 g/ml) | 1 (short axis 10 mm) | Rounded shape | 1 | 1 | |
| Cervical LN | 2 (mean SUVmax 5.6 g/ml) | 2 (mean short axis 10 mm) | Rounded shape | 1 | 2 (2 conglomerates) | |
| Skeletal | 20 (mean SUVmax 7.1 g/ml) | 20 | Sclerotic | 4 | 20 | |
| Liver | 1 (SUVmax 14.3 g/ml) | 1 | Hypoattenuating mass | HCC | 1 | - |
| Kidney | 1 (SUVmax 14.2 g/ml) | 1 | Heterogeneous mass | RCC | 1 | - |
| ∑ | 39 | 39 | 22a | 37 |
aSix patients with multiple sites, in total 14 with suspected distant metastases, and two with incidental findings. HCC, hepatocellular carcinoma; RCC, renal cell carcinoma.
Low-grade mediastinal lymph node uptake (SUVmax range 2.3 to 5.8 g/ml) with low suspicion of lymph node metastasis was seen in 22% (11/50) of the patients with 22 nodal uptakes in total. In 55% (6/11) of these patients, only non-specific mediastinal lymph node uptake was seen and 45% (5/11) of the patients had both non-specific and suspected metastatic mediastinal lymph node uptakes.
Association between 11C-acetate PET/CT findings and the estimated risk of locoregional lymph node metastases
Patients were divided into three groups according to estimated risk of pelvic lymph node metastases, <15% (n = 12), 15 to 45% (n =24) and >45% (n = 13), respectively. The observed proportions of pelvic lymph node metastases in the three groups were 33, 33 and 69%, respectively. The Pearson chi-square test displayed that there was no significant association between the observed proportion and the estimated nomogram risk of pelvic lymph node metastases in the three original groups (p = 0.08). Merging the first and the second groups, those with ≤45% estimated risk had positive pelvic lymph nodes in 33% (12/36), and those with >45% risk had positive pelvic lymph nodes in 69% (9/13), and this association proved to be significant (p <0.05).
The overall estimated mean risk of pelvic lymph node metastases was 32%, while the observed proportion of suspected pelvic lymph node metastases was 43% (21/49). Twelve patients had an estimated risk <15%. All of these patients had 11C-acetate-positive lesions in the prostate and 3/12 patients (25%) showed suspected pelvic lymph node involvement, two with intermediate and one with high suspicion of metastasis.
Prognostic value of prostate SUVmax
Binary logistic regression analysis proved prostate SUVmax to be higher in patients with suspected pelvic lymph node spread (odds ratio (OR) 1.45, p <0.05). Neither prostate SUVmax, PSA or Gleason score was associated with the presence of suspected distant metastases, nor were PSA or Gleason score associated with suspected pelvic lymph node spread.
There was a significant positive correlation between prostate SUVmax and PSA (Pearson correlation coefficient 0.35, p <0.05), but not with Gleason score. PSA and Gleason score were negatively correlated (−0.33, p <0.05).
Impact of 11C-acetate PET/CT findings on treatment strategy
In 43% (20/47) of the patients, treatment strategy was altered due to 11C-acetate PET/CT findings (Table 6). Eleven of these had an estimated risk of pelvic lymph node metastases ≤45% and the remaining nine >45%, with treatment changes as indicated in Table 7. In 19% (9/47) of the patients, suspected pelvic lymph node metastases (SUVmax 2.6 to 11.0 g/ml, short axis 5 to 16 mm) were treated with additional radiotherapy boost (mean additional dose 17 Gy, range 15 to 26 Gy). The nine patients that received additional radiotherapy boost against suspected pelvic lymph node metastases were fully informed of the non-conventional approach in this treatment, and all chose to go forward with it. The selected lymph nodes were irradiated according to the proposed Radiotherapy Oncology Group (RTOG) lymph node template. Lymph nodes were only boosted if they were within this field. Otherwise, the patients were considered to have distant metastases. The disease was far more extensive than expected, and therapeutic options were no longer curative in 21% (11/47) of the patients. The findings were confirmed with conventional examinations such as bone scintigraphy, and occasionally with biopsy, according to clinical routine before changing therapy to non-curative. Patients that were switched to palliative treatment received androgen deprivation therapy except for one patient who declined because of a diagnosis of previously unknown synchronous hepatocellular carcinoma accidentally detected on 11C-acetate PET/CT. Three out of the eleven patients also got radiotherapy to the prostate to palliate local symptoms. In 1/11 patients, radiotherapy treatment was cancelled due to comorbidity.
Table 6.
11 C-acetate PET/CT findings resulting in altered treatment strategy
| Patient number | Localisation pelvic LN metastases | Localisation distant metastases | Synchronous finding | Curative → additional RT | Curative → non-curative RT |
|---|---|---|---|---|---|
| 1 | Iliac int/ext | Paraaortal LN | - | - | Palliative RT |
| 2 | Iliac ext | Skeletal | - | - | No RT |
| 3 | Iliac int/ext | - | - | RT boost 16 Gy | - |
| 4 | Iliac int/ext | - | RT boost 16 Gy | - | |
| 5 | Iliac ext | - | - | RT boost 16 Gy | - |
| 6 | Iliac com | - | RT boost 16 Gy | - | |
| 7 | Iliac int/ext | - | - | RT boost 16 Gy | - |
| 8 | Obt, iliac int/ext/com | - | RT boost 15 Gy | - | |
| 9 | - | - | HCC with paraaortal LN | - | No RT |
| 10 | Iliac ext | - | RT boost 20 Gy | - | |
| 11 | Obt, iliac int/ext/com | Paraaortal LN, skeletal | - | - | No RT |
| 12 | Pararectal, iliac ext | - | - | RT boost 26 Gy | - |
| 13 | Pararectal, obt, iliac int/ext/com | Paraaortal LN | - | - | Palliative RT |
| 14 | Iliac int/ext/com | Paraaortal, thoracic, cervical LN | - | - | No RT |
| 15 | - | Skeletal | - | - | No RT |
| 16 | Iliac ext | - | - | RT boost 16 Gy | - |
| 17 | Iliac ext | Skeletal | - | - | No RT |
| 18 | - | - | Aortic aneurysm | - | No RT |
| 19 | Pararectal, iliac int/ext/com | Paraaortal, thoracic LN | - | - | No RT |
| 20 | Pararectal, obt, iliac ext | - | - | - | Palliative RT |
| ∑ | 17 | 8 | 2 | 9 | 11 |
HCC, hepatocellular carcinoma; LN, lymph nodes; Obt, obturator; RT, radiotherapy.
Table 7.
Treatment change due to 11 C-acetate PET/CT findings in estimated risk groups according to Cagiannos nomogram
| Estimated risk | Addition of RT boost to pelvic LN | Change to no/palliative RT |
|---|---|---|
| ≤45% (n =11) | 4 | 7 |
| >45% (n =9) | 5 | 4 |
LN, lymph nodes.
The remaining 57% (27/47) were treated with standard radiotherapy as initially planned. Standard radiotherapy of the prostate gland did not change due to 11C-acetate PET/CT results.
Discussion
There was a statistically significant association between the observed proportions of 11C-acetate PET/CT findings suggestive of pelvic lymph node metastases in merged estimated risk groups ≤45 and >45% according to the established Cagiannos nomogram, which supports the value of 11C-acetate PET/CT in pelvic lymph node staging of primary prostate cancer. The lack of a statistically significant result in the original three risk groups can be explained by inadequate power of the study since the number of patients in each risk group is low. Surprisingly, patients with previously estimated low (<15%) risk of pelvic lymph node metastases were found to have PET/CT-positive lymph nodes in 25%. The overall observed proportion of positive PET/CT findings suggestive of pelvic lymph node metastases was higher than the estimated risk, suggesting either that 11C-acetate PET/CT is superior to the clinical prediction tool or that there is a high rate of false-positive findings. It is possible that the inclusion criteria were such that this resulted in higher numbers, and there may be a selection bias especially since 11C-acetate PET/CT was a new method at the time and is still used only in cases with risk of pelvic lymph node involvement and where curative radiotherapy is the intended treatment. That may explain why our results are not comparable with other studies based on low- and intermediate-risk groups, but it does not explain the difference in the observed proportion of suspected pelvic lymph node metastases versus the expected risk in the Cagiannos nomogram. Since the patients in our study were treated with radiotherapy, there was no possibility to obtain histopathological confirmation of the suspected lymph node metastases. Haseebuddin et al. have shown a sensitivity of 68% and specificity of 78% of 11C-acetate PET/CT for detecting pelvic lymph node metastases [15], but apart from their study, little is published on suspected lymph node metastases with this method. Another possible explanation for the discordance could be that the Cagiannos nomogram underestimates the risk of lymph node metastasis, as has been previously suggested by Walz et al. in 2012 [19]. Schiavina et al. showed in their study on 11C-choline PET/CT in intermediate-risk and high-risk prostate cancer that the specificity and accuracy of PET/CT was better than that of the Kattan and Briganti nomograms, although the results were not statistically significant [20]. Altogether, our conclusion is that the higher proportion of 11C-acetate-positive pelvic lymph nodes is not merely an artefact. The distinction between metastatic and non-metastatic unspecific findings in this study was based on the combination of increased SUVmax, morphological changes in size and structure and pathological contrast enhancement, i.e., the established variables for characterising a lesion as benign or malignant. In prostate cancer, however, some data indicate that pelvic lymph nodes may be enlarged not only due to metastatic disease but also because of associated hyperplastic or regressive alterations [21]. On the other hand, it is also well known that normal-sized lymph nodes can harbour metastases.
The relatively common low intense acetate uptake in otherwise normal-appearing mediastinal lymph nodes is considered non-specific, but the mechanism and possible prognostic features remain unclear. The presence of non-specific mediastinal lymph nodes did not influence therapy, and this finding will be followed clinically. Mediastinal lymphadenopathy in prostate cancer is described in several case reports in the literature as a rare symptom of advanced disease [22–24]. This needs further evaluation, especially with the contradictory findings from a post-mortem study on 176 cases describing a distribution of lymph node metastases from prostate cancer to the paraaortal regions most frequently, followed by the external iliac and tracheobronchial regions [25].
Higher prostate SUVmax correlates in our study with the presence of suspected pelvic lymph node metastases, in contrast to earlier studies by Kato et al. concluding that prostate SUV measurements in dynamic 11C-acetate PET in known normal prostate and benign prostatic hyperplasia overlap significantly with those for known prostate cancer [26]. The reason for this may be the selection of mainly high-risk prostate cancer patients in our material.
The weaknesses of this study are that two indirect methods to predict metastatic disease in prostate cancer patients are compared and, as before mentioned, that the sample population is relatively small. In future research, the need for histopathologic confirmation is obvious, although one recent study by Haseebuddin et al. shows that the presence of 11C-acetate PET/CT-positive pelvic lymph nodes independently predicts treatment failure, despite negative histopathologic findings [15]. Furthermore, there may be a risk of selection bias as mentioned above, but also in the low-risk group (<15%) in this material, since they have been submitted for 11C-acetate PET/CT despite their low risk of pelvic lymph node metastases and may have some other characteristic in common, of which we are unaware.
11C-acetate is a relatively new tracer for prostate cancer staging with molecular properties reflecting the pattern of lipid metabolism. It could potentially be used for other slow growing cancers apart from prostate cancer such as highly differentiated hepatocellular carcinoma (HCC), renal cell carcinoma (RCC), bladder carcinoma and brain tumours [27,28]. In our material of 50 patients, we found one histology-verified RCC and one HCC, thus supporting previous studies.
The impact of 11C-acetate PET/CT on treatment strategy is high and in line with a previous report from Kjölhede et al. where 20% of patients examined with combined 18F-choline PET/CT and 18F-FDG PET/CT had their treatment plans altered [29]. This result also complies with several other studies on 18F-FDG PET/CT in various kinds of cancer with changes in treatment in 21 to 62% of the patients [30–32]. In our study, patients with limited pelvic nodal disease received integrated radiotherapy boost to the pelvic lymph nodes. This is a strategy that has been explored and found feasible regarding toxicity and clinical outcome [5].
Our results indicate that 11C-acetate PET/CT might be of value in pelvic lymph node staging in previously untreated high-risk prostate cancer patients, but these results should be interpreted with caution especially since the number of patients was low and histopathological confirmation was absent. However, the prognosis in patients with high-risk prostate cancer is poor, there is no optional treatment, and the risk of negative side effects is low, which makes the possible benefit of added therapy greater than the possible harm. The reason for excluding patients from curative treatment has been unequivocal metastatic disease taken into account the specificity and sensitivity issue. In our ongoing prospective study, survival as well as biochemical response will be assessed.
Conclusions
11C-acetate PET/CT for staging of prostate cancer influences treatment strategy in a substantial way and the use of 11C-acetate PET/CT seems to be of value in clinical practice for previously untreated high-risk patients, although the method needs further validation. The overall observed proportion of 11C-acetate PET/CT-positive pelvic lymph nodes is higher than the estimated pre-treatment nomogram risk, suggesting the nomogram might underestimate the risk. Prostate SUVmax is positively correlated to the presence of suspected pelvic lymph node metastases in 11C-acetate PET/CT and to PSA. Further long-term studies are needed to evaluate the impact of 11C-acetate PET/CT findings on patient outcome and survival.
Acknowledgements
This study was supported by Umeå University, Västerbotten County Council (ALF) and Cancer Research Foundation Norrland. We thank Hans Stenlund who provided helpful assistance in the statistical analysis.
Abbreviations
- CECT
contrast-enhanced computed tomography
- FDG
fluoro-deoxy-glucose
- HCC
hepatocellular carcinoma
- i.v.
intravenous
- LN
lymph node
- OR
odds ratio
- PET/CT
positron emission tomography/computed tomography
- PSA
prostate-specific antigen
- RCC
renal cell carcinoma
- ROI
region of interest
- RT
radiotherapy
- SUV
standardised uptake value
Footnotes
Competing interests
Parts of this material have previously been published by the authors with the title ‘Prostate cancer staging with 11C-acetate-PET/CT’ at the electronic poster exhibition EPOS at the European Congress of Radiology 2014. The authors declare that they have no other competing interests.
Authors' contributions
SS performed the reading of the 11C-acetate PET/CT examinations, analysed the material and produced the manuscript. CTK and KR designed the study and helped to draft the manuscript. CTK also collected data from the patients' medical records. MatÖ set up the radiochemistry production of 11C-acetate and critically revised the manuscript. MarÖ, JA and TS revised the manuscript and contributed with important intellectual content. All authors read and approved the final manuscript.
Contributor Information
Sara Strandberg, Email: sara.strandberg@vll.se.
Camilla Thellenberg Karlsson, Email: Camilla.thellenberg@onkologi.umu.se.
Torbjörn Sundström, Email: Torbjorn.sundstrom@diagrad.umu.se.
Mattias Ögren, Email: Mattias.ogren@diagrad.umu.se.
Margareta Ögren, Email: Margareta.ogren@diagrad.umu.se.
Jan Axelsson, Email: Jan.e.axelsson@vll.se.
Katrine Riklund, Email: Katrine.riklund.ahlstrom@diagrad.umu.se.
References
- 1.SEER Stat Fact Sheets: Prostate Cancer. In [http://seer.cancer.gov/statfacts/html/prost.html]
- 2.Nationella prostatacancerregistret. In [http://www.cancercentrum.se/sv/INCA/kvalitetsregister/Prostatacancer332/]
- 3.Kessler B, Albertsen P. The natural history of prostate cancer. Urol. Clin: North Am; 2003. [DOI] [PubMed] [Google Scholar]
- 4.Cagiannos I, Karakiewicz P, Eastham JA, Ohori M, Rabbani F, Gerigk C, Reuter V, Graefen M, Hammerer PG, Erbersdobler A, Huland H, Kupelian P, Klein E, Quinn DI, Henshall SM, Grygiel JJ, Sutherland RL, Stricker PD, Morash CG, Scardino PT, Kattan MW. A preoperative nomogram identifying decreased risk of positive pelvic lymph nodes in patients with prostate cancer. J Urol. 2003;170:1798–803. doi: 10.1097/01.ju.0000091805.98960.13. [DOI] [PubMed] [Google Scholar]
- 5.Fonteyne V, Lumen N, Ost P, Van Praet C, Vandecasteele K, De Gersem IW, Villeirs G, De Neve W, Decaestecker K, De Meerleer G. Hypofractionated intensity-modulated arc therapy for lymph node metastasized prostate cancer: early late toxicity and 3-year clinical outcome. Radiother Oncol. 2013;109:229–34. doi: 10.1016/j.radonc.2013.08.006. [DOI] [PubMed] [Google Scholar]
- 6.Warburg O, Posener K, Negelein E: On Metabolism of Tumors. London: Constable; 1930, 152:319–344
- 7.Jadvar H. Prostate cancer: PET with 18F-FDG, 18F- or 11C-acetate, and 18F- or 11C-choline. J Nucl Med. 2011;52:81–9. doi: 10.2967/jnumed.110.077941. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Castellucci P, Jadvar H. PET/CT in prostate cancer: non-choline radiopharmaceuticals. Q J Nucl Med Mol Imag. 2012;56:367–74. [PMC free article] [PubMed] [Google Scholar]
- 9.Röthke MC, Afshar-Oromieh A, Schlemmer H-P. Potential of PET/MRI for diagnosis of prostate cancer. Radiologe. 2013;53(8):676–81. doi: 10.1007/s00117-013-2499-0. [DOI] [PubMed] [Google Scholar]
- 10.Buchegger F, Garibotto V, Zilli T, Allainmat L, Jorcano S, Vees H, Rager O, Steiner C, Zaidi H, Seimbille Y, Ratib O, Miralbell R. First imaging results of an intraindividual comparison of (11)C-acetate and (18)F-fluorocholine PET/CT in patients with prostate cancer at early biochemical first or second relapse after prostatectomy or radiotherapy. Eur J Nucl Med Mol Imag. 2014;41(1):68–70. doi: 10.1007/s00259-013-2540-6. [DOI] [PubMed] [Google Scholar]
- 11.Picchio M, Berardi G, Fodor A, Busnardo E, Crivellaro C, Giovacchini G, Fiorino C, Kirienko M, Incerti E, Messa C, Gianolli L, Di Muzio N. (11)C-Choline PET/CT as a guide to radiation treatment planning of lymph-node relapses in prostate cancer patients. Eur J Nucl Med Mol Imag. 2014;41(7):1270–9. doi: 10.1007/s00259-014-2734-6. [DOI] [PubMed] [Google Scholar]
- 12.Vāvere AL, Kridel SJ, Wheeler FB, Lewis JS. 1-11C-acetate as a PET radiopharmaceutical for imaging fatty acid synthase expression in prostate cancer. J Nucl Med. 2008;49:327–34. doi: 10.2967/jnumed.107.046672. [DOI] [PubMed] [Google Scholar]
- 13.Oyama N, Akino H, Kanamaru H, Suzuki Y, Muramoto S, Yonekura Y, Sadato N, Yamamoto K, Okada K. 11C-acetate PET imaging of prostate cancer. J Nucl Med. 2002;43:181–6. [PubMed] [Google Scholar]
- 14.Czernin J, Benz MR, Allen-Auerbach MS. PET imaging of prostate cancer using C-acetate. PET Clin. 2009;4:163–72. doi: 10.1016/j.cpet.2009.05.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Haseebuddin M, Dehdashti F, Siegel BA, Liu J, Roth EB, Nepple KG, Siegel CL, Fischer KC, Kibel AS, Andriole GL, Miller TR. 11C-acetate PET/CT before radical prostatectomy: nodal staging and treatment failure prediction. J Nucl Med. 2013;54:699–706. doi: 10.2967/jnumed.112.111153. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Prostate cancer nomograms: pre-treatment. [http://nomograms.mskcc.org/Prostate/PreTreatment.aspx]
- 17.Stroom J, Blaauwgeers H, van Baardwijk A, Boersma L, Lebesque J, Theuws J, van Suylen RJ, Klomp H, Liesker K, van Pel R, Siedschlag C, Gilhuijs K. Feasibility of pathology-correlated lung imaging for accurate target definition of lung tumors. Int J Radiat Oncol Biol Phys. 2007;69:267–75. doi: 10.1016/j.ijrobp.2007.04.065. [DOI] [PubMed] [Google Scholar]
- 18.Biehl KJ, Kong F-M, Dehdashti F, Jin J-Y, Mutic S, El Naqa I, Siegel BA, Bradley JD. 18F-FDG PET definition of gross tumor volume for radiotherapy of non-small cell lung cancer: is a single standardized uptake value threshold approach appropriate? J Nucl Med. 2006;47:1808–12. [PubMed] [Google Scholar]
- 19.Walz J, Bladou F, Rousseau B, Laroche J, Salem N, Gravis G, Briganti A, Chun FK, Karakiewicz PI, Fournier G. Head to head comparison of nomograms predicting probability of lymph node invasion of prostate cancer in patients undergoing extended pelvic lymph node dissection. Urology. 2012;79:546–51. doi: 10.1016/j.urology.2011.11.036. [DOI] [PubMed] [Google Scholar]
- 20.Schiavina R, Scattoni V, Castellucci P, Picchio M, Corti B, Briganti A, Franceschelli A, Sanguedolce F, Bertaccini A, Farsad M, Giovacchini G, Fanti S, Grigioni WF, Fazio F, Montorsi F, Rigatti P, Martorana G. 11C-choline positron emission tomography/computerized tomography for preoperative lymph-node staging in intermediate-risk and high-risk prostate cancer: comparison with clinical staging nomograms. Eur Urol. 2008;54(2):392–401. doi: 10.1016/j.eururo.2008.04.030. [DOI] [PubMed] [Google Scholar]
- 21.Weingartner K, Ramaswamy A, Bittinger A, Gerharz EW, Voge D, Riedmiller H. Anatomical basis for pelvic lymphadenectomy in prostate cancer: results of an autopsy study and implications for the clinic. J Urol. 1996;156:1969–71. doi: 10.1016/S0022-5347(01)65406-5. [DOI] [PubMed] [Google Scholar]
- 22.Roca Edreira A, Aguilera Tubet C, Villanueva Peña A, Ballestero Diego R, Zubillaga Guerrero S. Mediastinal lymph nodes during the course of a metastatic prostate cancer. Actas Urol Esp. 2007;31:693–5. doi: 10.1016/S0210-4806(07)73707-5. [DOI] [PubMed] [Google Scholar]
- 23.Tsujino K, Sasada S, Kawahara K, Terada H, Komori C, Suzuki H, Okamoto N, Kobayashi M, Hirashima T, Matsui K, Kawase I. A case of prostatic adenocarcinoma clinically presenting as supraclavicular and mediastinal lymphadenopathy. Nihon Kokyuki Gakkai Zasshi. 2007;45:648–53. [PubMed] [Google Scholar]
- 24.Perez NE, Maryala S, Seren S, Feng J, Pansare V, Dhar R. Metastatic prostate cancer presenting as mediastinal lymphadenopathy identified by EUS with FNA. Gastrointest Endosc. 2007;65(6):948–9. doi: 10.1016/j.gie.2006.10.001. [DOI] [PubMed] [Google Scholar]
- 25.Arnheim FK. Carcinoma of the prostate; a study of the postmortem findings in 176 cases. J Urol. 1948;60:599–603. doi: 10.1016/S0022-5347(17)69279-6. [DOI] [PubMed] [Google Scholar]
- 26.Kato T, Tsukamoto E, Kuge Y, Takei T, Shiga T, Shinohara N, Katoh C, Nakada K, Tamaki N. Accumulation of [11C]acetate in normal prostate and benign prostatic hyperplasia: comparison with prostate cancer. Eur J Nucl Med Mol Imag. 2002;29:1492–5. doi: 10.1007/s00259-002-0885-3. [DOI] [PubMed] [Google Scholar]
- 27.Grassi I, Nanni C, Allegri V, Morigi JJ, Montini GC, Castellucci P, Fanti S. The clinical use of PET with (11)C-acetate. Am J Nucl Med Mol Imag. 2012;2:33–47. [PMC free article] [PubMed] [Google Scholar]
- 28.Liu RS. Clinical application of [C-11]acetate in oncology. Clin Positron Imag. 2000;3(4):185. doi: 10.1016/S1095-0397(00)00097-2. [DOI] [PubMed] [Google Scholar]
- 29.Kjölhede H, Ahlgren G, Almquist H, Liedberg F, Lyttkens K, Ohlsson T, Bratt O. Combined 18F-fluorocholine and 18F-fluoride positron emission tomography/computed tomography imaging for staging of high-risk prostate cancer. BJU Int. 2012;110:1501–6. doi: 10.1111/j.1464-410X.2012.11123.x. [DOI] [PubMed] [Google Scholar]
- 30.Selzner M, Hany TF, Wildbrett P, McCormack L, Kadry Z, Clavien P-A. Does the novel PET/CT imaging modality impact on the treatment of patients with metastatic colorectal cancer of the liver? Ann Surg. 2004;240:1027–34. doi: 10.1097/01.sla.0000146145.69835.c5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Abdelmalik AG, Alenezi S, Muzaffar R, Osman MM. The incremental added value of including the head in (18)F-FDG PET/CT imaging for cancer patients. Front Oncol. 2013;3:71. doi: 10.3389/fonc.2013.00071. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Tural D, Selcukbiricik F, Sager S, Akar E, Yildiz O, Serdengecti SH. PET-CT changes the management and improves outcome in patients with recurrent colorectal cancer. J Cancer Res Ther Medknow Publications and Media Pvt Ltd. 2014;10:121–6. doi: 10.4103/0973-1482.131445. [DOI] [PubMed] [Google Scholar]