

Abstract
Background
The ankle—brachial blood pressure (BP) index (ABI) not only indicates the presence of peripheral artery occlusive disease (PAOD) but predicts mortality in patients undergoing hemodialysis (HD). However, whether the site of PAOD can provide additional contribution to predicting mortality have not been investigated yet. Our primary objective was to determine the associations between the site of PAOD and all-cause and cardiovascular mortality in chronic HD (CHD) patients.
Methods
A retrospective cohort study was conducted to evaluate 444 Taiwanese CHD patients between December 2006 and June 2013. The site of PAOD together with other explanatory variables such as demographic data, body mass index, a history of cardiovascular diseases, HD vintage, biochemical data, and cardiothoracic ratio (CTR) were assessed by the Cox proportional hazards regression model.
Results
The frequency of PAOD was 14.6% in both legs, 4.9% in the right side only, and 5.1% in the left side only. During the study period, 127 all-cause and 93 cardiovascular deaths occurred. PAOD site was found to have significant predictive power for all-cause mortality with the order of 3.04 (95% CI: 1.56–5.90) hazard ratio on the right side, 2.48 (95% CI: 1.27–4.82) on the left side, and 4.11 (95% CI: 2.76–6.13) on both sides. The corresponding figures for cardiovascular mortality were 3.81 (95% CI: 1.87–7.76) on the right side, 2.76 (95% CI: 1.30–5.82) on the left side, and 3.95 (95% CI: 2.45–6.36) on both sides. After adjustment for other explanatory variables, only right-sided PAOD still remained to have significant predictive power for all-cause and cardiovascular mortality and bilateral PAOD kept the significant association with all-cause mortality.
Conclusions
The site of PAOD revealed various predictive powers for all-cause and cardiovascular mortality in CHD patients and only right-sided PAOD remained an independent predictor for both types of mortality making allowance for relevant confounding factors.
Introduction
The ankle—brachial index (ABI; the ratio of ankle to brachial systolic blood pressure [BP]) has been proven to be a simple, noninvasive, and reliable tool for the diagnosis of PAOD and a representative of systemic vascular disease. A significant decrease in patients with end-stage renal disease (ESRD) is attributed to the common co-morbid cardiovascular disease (CVD)[1–3]. Identifying the risk factors responsible for all-cause and cardiovascular (CV) mortality may present an opportunity for early intervention and the improvement of survival in these patients. Peripheral artery occlusive disease (PAOD), an atherosclerotic disorder, is frequently found in CKD patients [4, 5] and HD patients [6, 7], and has been demonstrated as a predictor for all-cause and cardiovascular mortality [7–9].
Patients are considered with PAOD when their either leg shows a lower ABI (<0.9). However, the severity of PAOD with an ABI value < 0.9 in clinical practice[10, 11] may vary with each leg. Further evidence also shows that a blood pressure difference between the legs (a difference in systolic BP of ≥15 mmHg or diastolic BP of ≥10 mmHg) was relevant to PAOD and was significantly associated with overall and CV death in HD patients [12]. The unequal limb atherosclerosis had an association with the interleg BP difference [8, 13]. Lin et al. had used the interleg ABI difference to make the limb atherosclerosis difference comparable between individuals and verified that an interleg ABI difference of ≥0.15 is an independent risk factor for all-cause mortality in patients with CHD [14]. In spite of those findings, there has been limited data about various sites of PAOD in association with all-cause and CV mortality. The aim of this study was to investigate whether PAOD site is an independent predictor for all-cause and CV mortality with adjustments for other explanatory factors in patients undergoing CHD in Taiwan.
Study Population and Methods
Study Design and Patients
Patients were included in to our study between December 2006 and January 2009. The inclusion criterion was at least 3 months of regular HD in the dialysis unit of Shin Kong Wu Ho-Su Memorial Hospital. The observation continued until June 2013. We excluded patients with any acute cardiovascular, cerebrovascular, infectious, or other active diseases in 3 months before entering this study. Patients with ABI values >1.3 were also excluded from analysis.
History collection and laboratory data
Demographic and medical data were obtained from the patients’ medical records at entry to the study (baseline). The following data were included: age, gender, body mass index (BMI, weight/height2), cardiothoracic ratio (CTR), smoking (ever versus never), comorbid conditions, serum creatinine, albumin, lipid profiles, iron profiles, hemoglobin (Hb), intact parathyroid hormone (iPTH), ionized calcium (iCa), phosphate (P), and dialysis efficiency (Kt/V). Moreover, we also collected the baseline medication history, including anti-platelet, renin-angiotensin system (RAS) blockade, beta-blocker, and statin. CVD was diagnosed using documented histories of coronary artery disease or cerebrovascular disease. Patients with CTR > 0.5 on chest radiographs were diagnosed with cardiomegaly. Blood specimens were collected after at least 8 h of fasting before dialysis sessions. Kt/V was determined according to the procedure described by Shinzato et al [15].
Ethic Statements
The Institutional Review Boards of the Shin-Kong Wu Ho-Su Memorial Hospital, Taipei, Taiwan, approved the study and waived the informed consent because our study was base on medical chart review. The patients’ information were anonymized and de-identified prior to analysis.
ABI measurement
The ABIs were measured with an Oscillometric machine (VaSera VS-1000; Fukuda Denshi, Tokyo, Japan), with simultaneous BP measurements in the arm without vascular access and around both ankles. The systolic pressure of the arm without dialysis access and the bilateral ankle pressures were used separately for the calculations. ABI was calculated automatically by dividing the ankle pressure by the brachial pressure. The ABI measurement was performed once for each patient before a hemodialysis session. Patients with ABI < 0.9 were diagnosed with PAOD, implying varying degrees of atherosclerosis in the lower extremities. We also defined right-sided PAOD for ABI <0.9 in only the right leg and left-sided PAOD for ABI <0.9 in only the left leg. Moreover, right-sided dominance of ABI represented a lower ABI value in right leg than left leg and vice versa.
Statistical analyses
Patients were lost to follow-up if a change in HD units was documented, and their data were censored at the date of the last documented contact in our dialysis unit. The outcome measures were all-cause and CV mortality (ascertained from Shin Kong Wu Ho-Su Memorial Hospital electronic records). Data are expressed as mean ± standard deviation (SD. The Kruskal—Wallis test or Mann—Whitney U test was used to compare the means of continuous variables and the χ2 test was used for categorical variables. Survival curves were estimated by using the Kaplan—Meier method and tested with the log-rank test. Moreover, crude and multi-variable analyses of mortality were performed using a Cox proportional hazards model to determine the hazard rate of death as a function of the different sites of PAOD. The assumption of proportionality was not violated, which was tested by using time-dependent Cox regression model. The adjusted confounders in multivariable model included all parameters, which are significant in univariate mode and those parameters showing significant difference between groups. A P-value of ≤0.05 was considered statistically significant. All statistical analyses were performed using the statistical package for social sciences statistical software (SPSS version 18; IBM Inc, Chicago, IL, USA).
Results
Patient background information
A total of 444 ESRD patients who received regular HD sessions with a dialysis vintage of 7.7 ± 5.0 years were enrolled. The mean age of the cohort was 61.6 ± 13.1 years (Interquartile range, 53–71 years), and the mean follow-up duration was 51.5 ± 21.9 months. During the follow-up period, 127 (28.6%) all-cause mortality events were ascertained in these patients, including fatal CV events (n = 93), malignancies (n = 9), infectious diseases (n = 17), gastrointestinal bleeding (n = 2), and others (n = 6). Eighty patients dropped out of the study. Table 1 shows the baseline characteristics of the study population. We classified the participants into four subgroups based on the presence and site of PAOD (non-PAOD, right-sided PAOD, left-sided PAOD, and bilateral PAOD). Table 2 shows the baseline characteristics of patients stratified by site. The prevalence of bilateral PAOD was 14.6% (65/444), of right-sided disease was 4.9% (22/444), and of left-sided disease was 5.1% (23/444). The difference across the four subgroups was statistically significant with respect to age (P < 0.001), gender (P = 0.05), presence of DM (P < 0.001), previous CVD (P = 0.040), systolic and diastolic BP (P < 0.001), serum albumin (P < 0.001), triglycerides (P = 0.021), total cholesterol (P = 0.028), Kt/V (P = 0.043), and cardiomegaly (P = 0.09). In the comparison between patients with PAOD, there was significant difference in age, gender, DM history, serum albumin, cholesterol, and calcium-phosphate product (all P<0.05). Right-sided PAOD had a lower age, presence of DM, and Kt/V; a higher calcium—phosphate product and nutrition status (serum albumin and cholesterol level) than did left-sided and bilateral PAOD.
Table 1. Characteristics of study population.
| Characteristic | All patients (444) |
|---|---|
| Age (years) | 61.6 ± 13.1 |
| Males (%) | 206 (46.4) |
| Duration of dialysis (year) | 7.7 ± 5.0 |
| Diabetes mellitus (%) | 145 (32.7) |
| Previous CVD (%) | 93 (20.9) |
| Smoking (%) | 92 (20.7) |
| Systolic BP (mmHg) | 151 ± 77 |
| Diastolic BP (mmHg) | 78 ± 17 |
| Body mass index (kg/m2) | 22.9 ± 3.7 |
| Albumin level (g/dL) | 4.1 ± 0.3 |
| Triglyceride (mg/dL) | 152 ± 124 |
| Cholesterol level (mg/dL) | 175 ± 42 |
| Kt/V | 1.66 ± 0.23 |
| Cardiothoracic ratio | 0.5 ± 0.07 |
| Hemoglobin (g/dL) | 10.4 ± 1.3 |
| iPTH (pg/mL) | 193 ± 204 |
| Ferritin (μg/dL) | 636 ± 784 |
| Ca P product (mg/dL)2 | 48.2 ± 13.5 |
| Right side ABI | 1.03 ± 0.18 |
| Left side ABI | 1.03 ± 0.20 |
| Medications | |
| Anti-platelet use (%) | 154 (34.7) |
| RAS blockader use (%) | 90 (20.3) |
| Beta-blocker use (%) | 142 (32.0) |
| Statin use (%) | 143 (32.2) |
| All cause mortality events (%) | 127 (28.6) |
| Cardiovascular mortality events (%) | 93 (20.9) |
Abbreviations: CVD, cardiovascular disease; BP, blood pressure; iPTH, intact parathyroid hormone; Ca, calcium; P, phosphate; ABI, ankle-brachial index; RAS, renin-angiotensin system.
Table 2. Characteristics of patients at inclusion according to the location of PAOD.
| Characteristic | Non (n = 334) | Right (n = 22) | Left (n = 23) | Bilateral (n = 65) | P * | P # |
|---|---|---|---|---|---|---|
| Age (years) | 59.3 ± 13.1 | 65.0 ± 10.9 | 73.0 ± 7.9 | 68.6 ± 10.6 | <0.001 | 0.017 |
| Male (%) | 165 (49) | 12 (54) | 12 (52) | 17 (26) | 0.005 | 0.015 |
| Duration of dialysis (years) | 7.8 ± 5.1 | 6.7 ± 4.6 | 8.5 ± 5.6 | 6.9 ± 4.3 | 0.526 | 0.559 |
| Diabetes mellitus (%) | 83 (24) | 8 (36) | 10 (43) | 44 (67) | <0.001 | 0.014 |
| Previous CVD (%) | 63 (18) | 5 (22) | 3 (13) | 22 (34) | 0.040 | 0.136 |
| Smoking history (%) | 75 (22) | 5 (22) | 5 (21) | 7 (10) | 0.204 | 0.262 |
| Systolic BP (mmHg) | 161 ± 82 | 141 ± 44 | 114 ± 30 | 116 ± 44 | <0.001 | 0.077 |
| Diastolic BP (mmHg) | 82 ± 15 | 74 ± 17 | 62 ± 11 | 64 ± 19 | <0.001 | 0.081 |
| Body mass index (kg/m2) | 22.9 ± 3.8 | 22.7 ± 2.7 | 22.0 ± 3.3 | 23.2 ± 4.0 | 0.624 | 0.396 |
| Albumin level (g/dL) | 4.2 ± 0.3 | 4.2 ± 0.4 | 4.0 ± 0.3 | 3.9 ± 0.3 | <0.001 | 0.008 |
| Triglyceride (mg/dL) | 147 ± 126 | 209 ± 185 | 133 ± 79 | 167 ± 95 | 0.021 | 0.278 |
| Cholesterol level (mg/dL) | 173 ± 40 | 207 ± 65 | 159 ± 40 | 179 ± 38 | 0.028 | 0.030 |
| Kt/V | 1.65 ± 0.24 | 1.58 ± 0.18 | 1.73 ± 0.21 | 1.71 ± 0.20 | 0.043 | 0.056 |
| Cardiomegaly (%) | 142 (42) | 9 (40) | 13 (56) | 41 (63) | 0.009 | 0.138 |
| Hemoglobin (g/dL) | 10.5 ± 1.4 | 10.6 ± 1.7 | 10.2 ± 1.3 | 10.2 ± 1.1 | 0.281 | 0.496 |
| iPTH (pg/mL) | 202 ± 211 | 191 ± 170 | 136 ± 118 | 166 ± 196 | 0.109 | 0.528 |
| Ferritin (μg/dL) | 648 ± 893 | 556 ± 230 | 597 ± 189 | 620 ± 202 | 0.784 | 0.660 |
| Ca P product (mg/dL)2 | 48.8 ± 13.7 | 54.2 ± 12.7 | 42.8 ± 10.8 | 44.5 ± 12.8 | 0.003 | 0.004 |
| Medications | ||||||
| Anti-platelet use (%) | 123 (36) | 12 (54) | 16 (69) | 51 (78) | 0.074 | 0.095 |
| RAS blockade use (%) | 72 (21) | 3 (13) | 6 (26) | 9 (13) | 0.379 | 0.366 |
| Beta-blocker use (%) | 105 (31) | 10 (45) | 7 (30) | 20 (30) | 0.583 | 0.423 |
| Statin use (%) | 103 (30) | 8 (40) | 11 (47) | 21 (32) | 0.387 | 0.413 |
Abbreviations: CVD, cardiovascular disease; BP, blood pressure; iPTH, intact parathyroid hormone; Ca, calcium; P, phosphate; RAS, renin-angiotensin system
*Comparison between all four groups
# Comparison between all groups except non-PAOD group.
Kaplan—Meier survival curves
Fig 1 shows that the Kaplan—Meier survival curves of all-cause (Fig 1A) and CV mortality (Fig 1B) according to the site of PAOD. The difference in survival among the four groups was significant for all-cause (χ2 = 60.89, P < 0.001) and CV (χ2 = 45.24, P < 0.001) mortality using the log-rank test. However, no significant difference in survival among the three groups of right side, left side, and bilateral PAOD was noted.
Fig 1. Kaplan—Meier survival curves.
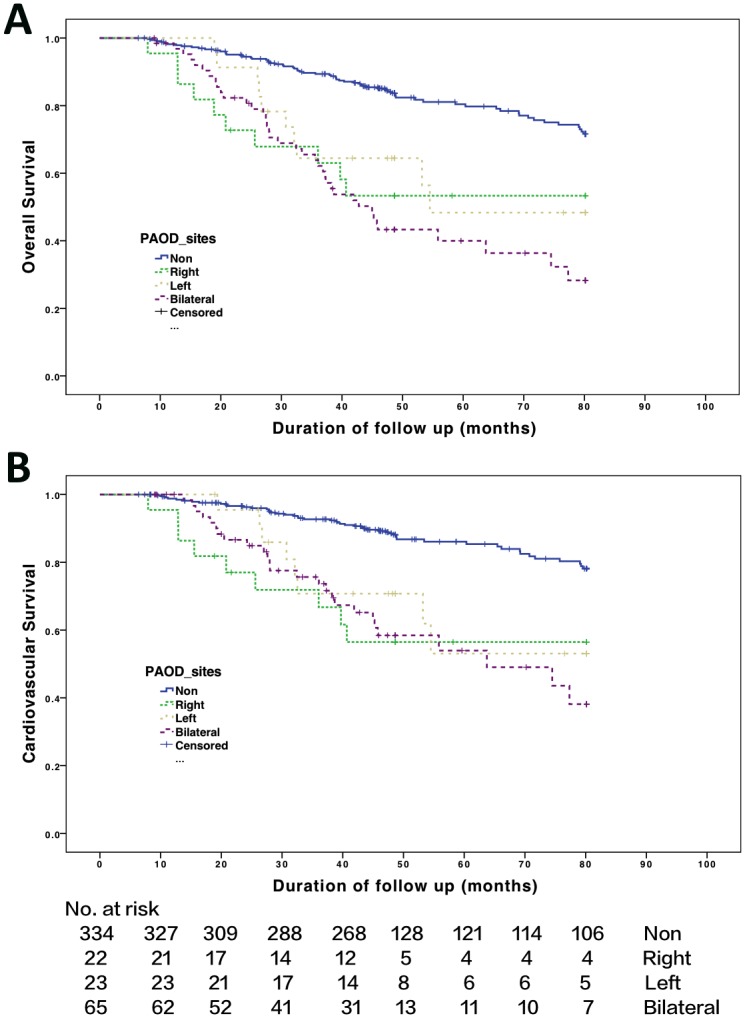
Probabilities of (A) overall survival with log-rank test: χ2 = 60.89; P ≤ 0.001 in the four groups and χ2 = 2.02; P = 0.364 in the three PAOD groups. (B) Cardiovascular survival with log-rank test: χ2 = 45.24; P ≤ 0.001 in the four groups and χ2 = 0.69; P = 0.708 in the three PAOD groups.
All-cause mortality in CHD patients
During the 6.6-year follow-up period, 127 deaths were recorded. Compared with patients without PAOD, the hazard ratio (HR) for all-cause death was 3.04 (95% CI: 1.56 to 5.90) in patients with right-sided PAOD, 2.48 (95% CI: 1.27 to 4.82) with left-sided PAOD, and 4.11, (95% CI: 2.76 to 6.13) with bilateral PAOD (Table 3). Other significant predictors for all-cause death included age, DM, previous CVD, systolic and diastolic BP, serum albumin, cardiomegaly, and calcium phosphate products (all P < 0.05). In the multi-variable analysis, the HR for all-cause death was 3.04 (95% CI: 1.50 to 6.14) in patients with right-sided PAOD, 1.36 (95% CI: 0.65 to 2.82) with left-sided PAOD, and 1.86 (95% CI: 1.09 to 3.16) for bilateral PAOD after adjustment for age, gender, DM, previous CVD, Kt/V, CTR> 0.5, blood pressure, statin use and serum albumin, triglycerides, cholesterol, and calcium—phosphate product. Among the risk factors, HRs for age (1.02, 95% CI: 1.00–1.04), previous CVD (1.92, 95% CI: 1.29–2.84), cardiomegaly (1.63, 95% CI: 1.10–2.41), and serum albumin level (0.25, 95% CI: 0.14–0.44) remained significant.
Table 3. Cox proportional hazards regression analysis for all-cause mortality.
| Crude | Multivariable | |||
|---|---|---|---|---|
| Parameter | Hazard ratios (95% CI) | P | Hazard ratios (95% CI) | P |
| Age (per year) | 1.05 (1.03–1.06) | <0.001 | 1.02 (1.00–1.04) | 0.005 |
| Male versus female | 1.04 (0.73–1.47) | 0.814 | 1.47 (0.94–2.28) | 0.086 |
| Duration of dialysis (per year) | 0.99 (0.95–1.03) | 0.727 | ||
| Diabetes mellitus | 1.92 (1.35–2.72) | <0.001 | 1.07 (0.69–1.65) | 0.738 |
| Previous CVD | 2.41 (1.66–3.48) | <0.001 | 1.92 (1.29–2.84) | 0.001 |
| Smoking (ever versus never) | 1.10 (0.72–1.67) | 0.645 | ||
| Systolic BP (per 1 mmHg) | 0.98 (0.98–0.99) | <0.001 | 1.00 (0.99–1.00) | 0.908 |
| Diastolic BP (per 1 mmHg) | 0.97 (0.96–0.98) | <0.001 | 0.99 (0.99–1.00) | 0.323 |
| Body mass index (per 1 kg/m2) | 0.98 (0.93–1.03) | 0.461 | ||
| Albumin level (per 1 g/dL) | 0.18 (0.12–0.28) | <0.001 | 0.25 (0.14–0.44) | <0.001 |
| Triglyceride (per 1 mg/dL) | 0.99 (0.99–1.00) | 0.100 | 0.99 (0.99–1.00) | 0.065 |
| Cholesterol level (per 1 mg/dL) | 0.99 (0.99–1.00) | 0.329 | 1.00 (0.99–1.01) | 0.233 |
| Kt/V (per 1 unit) | 0.82 (0.38–1.76) | 0.628 | 1.05 (0.40–2.74) | 0.914 |
| Cardiomegaly | 2.33 (1.62–3.36) | <0.001 | 1.63 (1.10–2.41) | 0.015 |
| Hemoglobin (per 1 g/dL) | 0.89 (0.78–1.02) | 0.102 | ||
| iPTH (per 1 pg/mL) | 0.99 (0.99–1.00) | 0.244 | ||
| Ferritin (per 1.0 μg/dL) | 1.00 (0.99–1.00) | 0.558 | ||
| Ca P product (per 1 mg2/dL2) | 0.98 (0.97–0.36) | 0.017 | 1.00 (0.98–1.01) | 0.590 |
| Medications | ||||
| Anti-platelet use | 0.87 (0.60–1.27) | 0.481 | ||
| RAS blockade use | 1.14 (0.75–1.73) | 0.514 | ||
| Beta-blocker use | 0.72 (0.48–1.08) | 0.726 | ||
| Statin use | 0.64 (0.42–0.96) | 0.031 | 0.691 (0.45–1.05) | 0.086 |
| PAOD (versus non) | ||||
| Right side | 3.04 (1.56–5.90) | 0.001 | 3.04 (1.50–6.14) | 0.002 |
| Left side | 2.48 (1.27–4.82) | 0.007 | 1.36 (0.65–2.82) | 0.407 |
| Bilateral | 4.11 (2.76–6.13) | <0.001 | 1.86 (1.09–3.16) | 0.022 |
Abbreviation: CVD, cardiovascular disease; BP, blood pressure; RAS, renin-angiotensin system; iPTH, intact parathyroid hormone; Ca, calcium; P, phosphate; PAOD, peripheral arterial occlusion disease.
Cardiovascular mortality in CHD patients
Ninety-three fatal CV events were ascertained during the follow-up period. Table 4 shows the results of the Cox proportional hazards regression analysis of various parameters as predictors for CV mortality. Compared with patients without PAOD, the crude HRs for CV mortality in patients with right-sided PAOD, left-sided PAOD, and bilateral PAOD were 3.81 (95% CI: 1.87–7.76), 2.76 (95% CI: 1.30–5.82), and 3.95 (95% CI: 2.45–6.36), respectively. Other significant predictors in the univariate analysis were age (1.04, 95% CI: 1.02–1.06), a history of DM (2.02, 95% CI: 1.34–3.05), previous CVD (2.26, 95% CI: 1.46–3.49), systolic BP (0.98, 95% CI: 0.98–0.99), diastolic BP (0.96, 95% CI: 0.95–0.97), albumin level (0.19, 95% CI: 0.12–0.32), and cardiomegaly (2.22, 95% CI: 1.45–3.39). After adjusting for a history of cardiomegaly, previous CVD, low serum albumin level, and advanced age in the multi-variable regression model, right-sided PAOD (3.65, 95% CI: 1.72–7.74) was still significant for CV mortality, whereas left-sided PAOD (1.11, 95% CI: 0.48–2.53) and bilateral PAOD (1.51, 95% CI: 0.79–2.87) were no longer statistically significant.
Table 4. Cox proportional hazards regression analysis for cardiovascular mortality.
| Crude | Multivariable | |||
|---|---|---|---|---|
| Parameter | Hazard ratios (95% CI) | P | Hazard ratios (95% CI) | P |
| Age (per 1 year) | 1.04 (1.02–1.06) | <0.001 | 1.02 (1.00–1.04) | 0.042 |
| Male versus female | 1.13 (0.75–1.70) | 0.541 | 1.87 (1.11–3.16) | 0.018 |
| Duration of dialysis (per 1 year) | 1.00 (0.95–1.04) | 0.983 | ||
| Diabetes mellitus | 2.02 (1.34–3.05) | 0.001 | 1.20 (0.73–1.98) | 0.463 |
| Previous CVD | 2.26 (1.46–3.49) | <0.001 | 1.91 (1.20–3.04) | 0.006 |
| Smoking (ever versus never) | 1.27 (0.79–2.04) | 0.309 | ||
| Systolic BP (per 1 mmHg) | 0.98 (0.98–0.99) | <0.001 | 1.00 (0.99–1.00) | 0.980 |
| Diastolic BP (per 1 mmHg) | 0.96 (0.95–0.97) | <0.001 | 0.97 (0.95–0.99) | 0.041 |
| Body mass index (per 1 kg/m2) | 0.96 (0.90–1.02) | 0.202 | ||
| Albumin level (per 1g/dL) | 0.19 (0.12–0.32) | <0.001 | 0.27 (0.14–0.52) | <0.001 |
| Triglyceride (per 1 mg/dL) | 0.99 (0.99–1.00) | 0.170 | 0.99 (0.99–1.00) | 0.120 |
| Cholesterol level (per 1 mg/dL) | 0.99 (0.99–1.00) | 0.409 | 1.00 (0.99–1.00) | 0.334 |
| Kt/V (per 1.0) | 0.97 (0.40–2.36) | 0.957 | 1.73 (0.56–5.33) | 0.334 |
| Cardiomegaly | 2.22 (1.45–3.39) | <0.001 | 1.58 (1.00–2.50) | 0.047 |
| Hemoglobin (per 1 g/dL) | 0.86 (0.74–1.01) | 0.079 | ||
| iPTH (per 1 pg/mL) | 1.00 (0.99–1.00) | 0.909 | ||
| Ferritin (per 1 μg/dL) | 1.00 (0.99–1.00) | 0.636 | ||
| Ca P product (per 1 mg2/dL2) | 0.99 (0.97–1.00) | 0.178 | 1.01 (0.99–1.02) | 0.240 |
| Medications | ||||
| Anti-platelet use | 0.95 (0.63–1.47) | 0.854 | ||
| RAS blockade use | 1.06 (0.64–1.73) | 0.817 | ||
| Beta-blocker use | 0.71 (0.45–1.14) | 0.163 | ||
| Statin use | 0.65 (0.40–1.04) | 0.075 | ||
| PAOD (versus non) | ||||
| Right side | 3.81 (1.87–7.76) | <0.001 | 3.65 (1.72–7.74) | 0.001 |
| Left side | 2.76 (1.30–5.82) | 0.008 | 1.11 (0.48–2.53) | 0.800 |
| Bilateral | 3.95 (2.45–6.36) | <0.001 | 1.51 (0.79–2.87) | 0.207 |
Abbreviation: CVD, cardiovascular disease; BP, blood pressure; RAS, renin-angiotensin system; PAOD, iPTH, intact parathyroid hormone; Ca, calcium; P, phosphate; peripheral arterial occlusion disease.
Right-sided dominance vs. left-sided dominance of ABI
The prevalence of right-sided dominance in ABI was 50.2% (223/444) and of left-sided dominance was 43.2% (192/444). There was no significant difference of ABI value between legs in individuals (P = 0.412, by Wilcoxon signed-rank test). The comparison of survival outcomes between right-sided and left-sided dominance in ABI values is shown in Fig 2, which demonstrated a lacking of significant difference in survival between right-sided and left-sided dominance for ABI values in all patients (Fig 2A, χ2 = 1.32, P = 0.249), patients without PAOD (Fig 2B, χ2 = 3.47, P = 0.062), and patients with PAOD (Fig 2C, χ2 = 0.20, P = 0.651). However, the trend suggested that right-sided disease may have poorer survival results.
Fig 2. Probabilities of overall survival according to dominance side of ABI value.
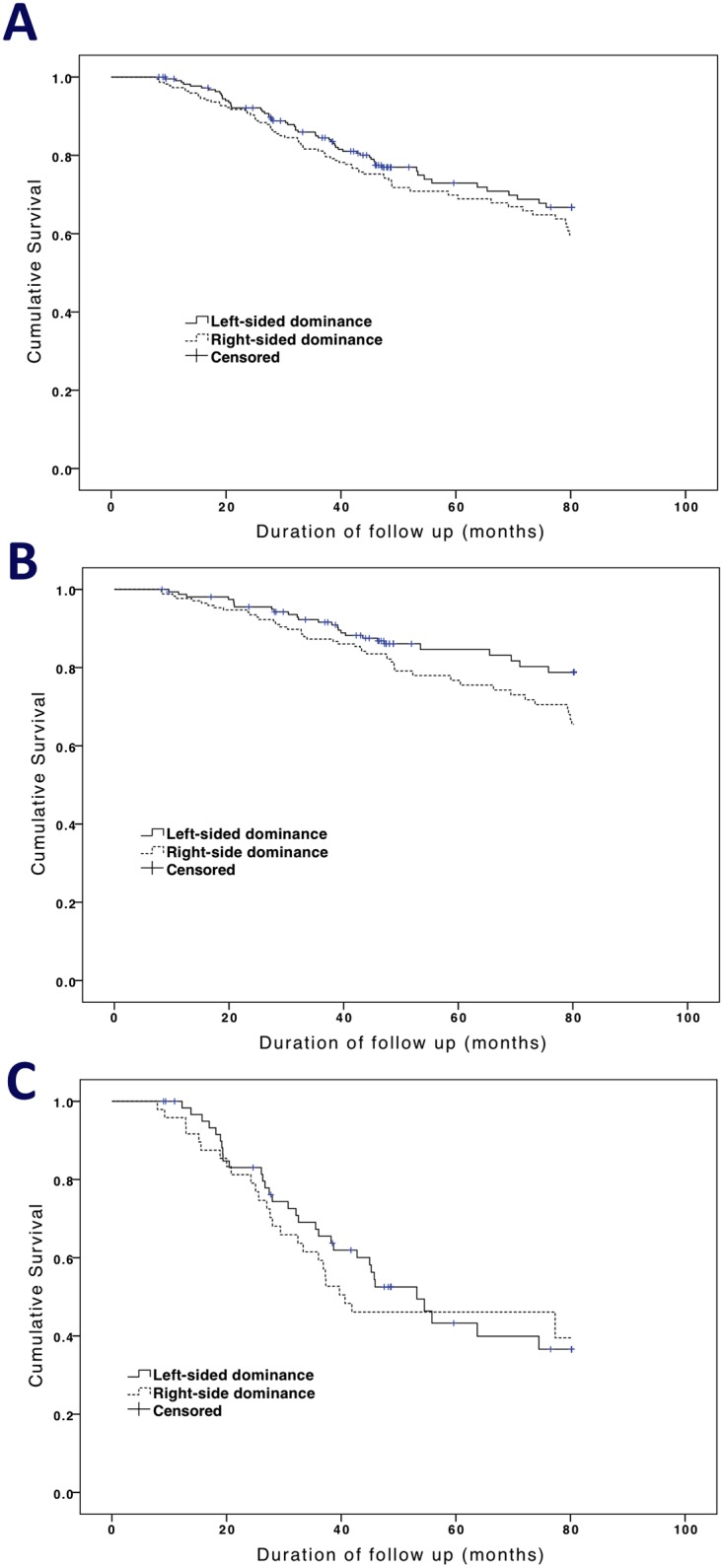
(A) in all patients with log-rank test: χ2 = 1.32; P = 0.249; (B) in patients without PAOD with log-rank test: χ2 = 3.47; P = 0.062; (C) in patients with PAOD with log-rank test: χ2 = 0.20; P = 0.651.
Discussion
Both PAOD and ABI are prognostic factors for predicting subsequent all-cause and CV mortality in the general population [7, 16, 17] as well as in HD patients [8, 9, 18]. In our study, we successfully demonstrated that the site of PAOD, as defined by ABI findings, was another independent predictor for all-cause and CV mortality in CHD patients. After adjustment for risk factors in the multivariate analysis, patients with right-sided PAOD had a higher risk for all-cause and CV mortality, whereas patients with left-sided PAOD did not. The two hypotheses were postulated to explain this finding. One was that right-sided ABI values may mean more severe vascular stenosis when they were the same to left-sided ABI values. Zhang et al. had reported the mean right ankle systolic blood pressure was about 1.7 mmHg higher than left side in Chinese population[19]. Therefore, the same ABI value in both sides didn’t mean the same atherosclerosis extent. The other possible explanation was that right-side disability may lead to a poorer prognosis because the general population is right-side dominant. Fig 2 shows a trend that right-side dominant ABI values had poorer survival outcomes in all patients and patients with/without PAOD. In fact, patients with right-sided PAOD also had higher calcium—phosphate product levels and lower Kt/v values, which suggested that this finding may be associated with poor dialysis adequacy and worse systemic calcium deposition. Therefore, to increase the dialysis dose and to control the serum calcium and phosphate levels in patients with CHD could prevent the developing of right-sided PAOD and delay the progression of vascular stenosis.
Cardiomegaly was higher in the group with abnormal ABI values on both sides. This finding was reasonable as some evidence had suggested that cardiomegaly was related to advanced age and malnutrition [20, 21]. Our data show that bilateral PAOD patients were older and had lower serum albumin levels. Serum calcium—phosphate product also lost its predictive power for all-cause mortality after adjusting for prognostic factors. This suggests that its impact might be also mediated through systemic arterial problems [22–24]. A low level of serum albumin has been a predictor for the poor prognosis of HD patients [8, 24–26].
The previously-identified risk factors for HD patients with PAOD included advanced age, DM, a history of CVD, smoking history, low diastolic BP, low pulse pressure, and low albumin levels [8, 27]; most were confirmed in our univariate analysis. However, several risk factors lost their significance in the multi-variate analysis. For example, although DM was a predictor of all-cause and CV mortality in our crude analysis, it was not significant in the multivariate analysis. The impact of DM on the multifactorial events that included vascular atherosclerosis and calcification was attributed to this phenomenon [8]. A CTR >0.5 was significantly related to the high mortality rate in our CHD patients and in diabetic HD patients [20]. However, Bohn et al failed to demonstrate CTR as a predictor of mortality in CHD patients [28]. Therefore, the clinical implications of CTR in HD patients for prediction of mortality are still controversial.
Our study has some limitations. First, it was single-center study, which might not be generalizable to all HD populations. Second, the patient population was small; nevertheless, this concern may be trivial because there was a significant relationship between PAOD site and mortality. Third, the gold-standard method for detecting PAOD is Doppler but we adopted ABI method to access the diagnosis of PAOD. Sometime, ABI method would lead to pseudomorphic normal when stenosis appeared in both arm and legs. However, ABI method had been extensively validated to be a reliable, and non-invasive tool for the diagnosis of PAOD[11, 29]. Finally, we only used baseline covariates to predict mortality. This may have resulted in biased estimates when the related variable was a time-varying predictor. However, there were two strengths in our current study. First, our follow-up duration was adequate to obtain sufficient numbers of deaths. Second, several well-established confounding factors related to dialysis therapy were adjusted.
To the best of our knowledge, this is first study that demonstrated an association between the site of PAOD and all-cause and CV mortality in CHD patients. The different findings on the site of PAOD may be attributed to the level of dialysis adequacy and calcium phosphate precipitation, which may contribute to vascular atherosclerosis and calcification. However, large-scale multicenter studies will be needed to verify our findings.
Conclusion
The site of PAOD has been associated with all-cause and CV mortality in the Taiwanese HD population. We also found that right-side dominant PAOD was an independent predictor for mortality in HD patients independent of other predictors. We suggest routine screening for PAOD in HD patients with noninvasive ABI and that physicians should be vigilant for HD patients with abnormal ABI values, especially on the right side.
Supporting Information
(XLS)
Data Availability
All relevant data are within the paper and its Supporting Information files.
Funding Statement
This study was sponsored by the Shin Kong Wu Ho-Su Memorial Hospital (SKH-8302-104-DR-08). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
References
- 1. Mallick NP, Jones E, Selwood N. The European (European Dialysis and Transplantation Association-European Renal Association) Registry. American journal of kidney diseases: the official journal of the National Kidney Foundation. 1995;25(1):176–87. . [DOI] [PubMed] [Google Scholar]
- 2. Shinzato T, Nakai S, Akiba T, Yamagami S, Yamazaki C, Kitaoka T, et al. Report of the annual statistical survey of the Japanese Society for Dialysis Therapy in 1996. Kidney international. 1999;55(2):700–12. 10.1046/j.1523-1755.1999.00297.x . [DOI] [PubMed] [Google Scholar]
- 3. Ortiz A, Covic A, Fliser D, Fouque D, Goldsmith D, Kanbay M, et al. Epidemiology, contributors to, and clinical trials of mortality risk in chronic kidney failure. Lancet. 2014;383(9931):1831–43. 10.1016/S0140-6736(14)60384-6 . [DOI] [PubMed] [Google Scholar]
- 4. de Vinuesa SG, Ortega M, Martinez P, Goicoechea M, Campdera FG, Luno J. Subclinical peripheral arterial disease in patients with chronic kidney disease: prevalence and related risk factors. Kidney international Supplement. 2005;(93):S44–7. 10.1111/j.1523-1755.2005.09310.x . [DOI] [PubMed] [Google Scholar]
- 5. Leskinen Y, Salenius JP, Lehtimaki T, Huhtala H, Saha H. The prevalence of peripheral arterial disease and medial arterial calcification in patients with chronic renal failure: requirements for diagnostics. American journal of kidney diseases: the official journal of the National Kidney Foundation. 2002;40(3):472–9. 10.1053/ajkd.2002.34885 . [DOI] [PubMed] [Google Scholar]
- 6. Cheung AK, Sarnak MJ, Yan G, Dwyer JT, Heyka RJ, Rocco MV, et al. Atherosclerotic cardiovascular disease risks in chronic hemodialysis patients. Kidney international. 2000;58(1):353–62. 10.1046/j.1523-1755.2000.00173.x . [DOI] [PubMed] [Google Scholar]
- 7. Newman AB, Shemanski L, Manolio TA, Cushman M, Mittelmark M, Polak JF, et al. Ankle-arm index as a predictor of cardiovascular disease and mortality in the Cardiovascular Health Study. The Cardiovascular Health Study Group. Arteriosclerosis, thrombosis, and vascular biology. 1999;19(3):538–45. . [DOI] [PubMed] [Google Scholar]
- 8. Ono K, Tsuchida A, Kawai H, Matsuo H, Wakamatsu R, Maezawa A, et al. Ankle-brachial blood pressure index predicts all-cause and cardiovascular mortality in hemodialysis patients. Journal of the American Society of Nephrology: JASN. 2003;14(6):1591–8. . [DOI] [PubMed] [Google Scholar]
- 9. Chen SC, Chang JM, Hwang SJ, Tsai JC, Liu WC, Wang CS, et al. Ankle brachial index as a predictor for mortality in patients with chronic kidney disease and undergoing haemodialysis. Nephrology. 2010;15(3):294–9. 10.1111/j.1440-1797.2010.01187.x . [DOI] [PubMed] [Google Scholar]
- 10. Newman AB, Tyrrell KS, Kuller LH. Mortality over four years in SHEP participants with a low ankle-arm index. Journal of the American Geriatrics Society. 1997;45(12):1472–8. . [DOI] [PubMed] [Google Scholar]
- 11. Laing S, Greenhalgh RM. The detection and progression of asymptomatic peripheral arterial disease. The British journal of surgery. 1983;70(10):628–30. . [DOI] [PubMed] [Google Scholar]
- 12. Chen SC, Chang JM, Tsai YC, Tsai JC, Su HM, Hwang SJ, et al. Association of interleg BP difference with overall and cardiovascular mortality in hemodialysis. Clinical journal of the American Society of Nephrology: CJASN. 2012;7(10):1646–53. 10.2215/CJN.04570512 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Clark CE, Powell RJ. The differential blood pressure sign in general practice: prevalence and prognostic value. Family practice. 2002;19(5):439–41. . [DOI] [PubMed] [Google Scholar]
- 14. Lin CY, Leu JG, Fang YW, Tsai MH. Association of interleg difference of ankle brachial index with overall and cardiovascular mortality in chronic hemodialysis patients. Renal failure. 2015;37(1):88–95. 10.3109/0886022X.2014.976104 . [DOI] [PubMed] [Google Scholar]
- 15. Shinzato T, Nakai S, Fujita Y, Takai I, Morita H, Nakane K, et al. Determination of Kt/V and protein catabolic rate using pre- and postdialysis blood urea nitrogen concentrations. Nephron. 1994;67(3):280–90. . [DOI] [PubMed] [Google Scholar]
- 16. Newman AB, Sutton-Tyrrell K, Vogt MT, Kuller LH. Morbidity and mortality in hypertensive adults with a low ankle/arm blood pressure index. JAMA: the journal of the American Medical Association. 1993;270(4):487–9. . [PubMed] [Google Scholar]
- 17. Leng GC, Lee AJ, Fowkes FG, Whiteman M, Dunbar J, Housley E, et al. Incidence, natural history and cardiovascular events in symptomatic and asymptomatic peripheral arterial disease in the general population. International journal of epidemiology. 1996;25(6):1172–81. . [DOI] [PubMed] [Google Scholar]
- 18. Guerrero A, Montes R, Munoz-Terol J, Gil-Peralta A, Toro J, Naranjo M, et al. Peripheral arterial disease in patients with stages IV and V chronic renal failure. Nephrology, dialysis, transplantation: official publication of the European Dialysis and Transplant Association—European Renal Association. 2006;21(12):3525–31. 10.1093/ndt/gfl470 . [DOI] [PubMed] [Google Scholar]
- 19. Zhang Z, Ma J, Tao X, Zhou Y, Liu X, Su H. The prevalence and influence factors of inter-ankle systolic blood pressure difference in community population. PloS one. 2013;8(8):e70777 10.1371/journal.pone.0070777 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Yen TH, Lin JL, Lin-Tan DT, Hsu KH. Cardiothoracic ratio, inflammation, malnutrition, and mortality in diabetes patients on maintenance hemodialysis. The American journal of the medical sciences. 2009;337(6):421–8. 10.1097/MAJ.0b013e31819bbec1 . [DOI] [PubMed] [Google Scholar]
- 21. Chen KH, Hung CC, Lin-Tan DT, Huang WH, Hsu CW, Weng SM, et al. Cardiothoracic ratio association with mortality in patients on maintenance peritoneal dialysis. Therapeutic apheresis and dialysis: official peer-reviewed journal of the International Society for Apheresis, the Japanese Society for Apheresis, the Japanese Society for Dialysis Therapy. 2011;15(1):81–8. 10.1111/j.1744-9987.2010.00860.x . [DOI] [PubMed] [Google Scholar]
- 22. Mehrotra R. Vascular calcification in chronic kidney disease: evolving pathogenesis with progressive chronic kidney disease? Kidney international. 2006;69(1):195 10.1038/sj.ki.5000039 . [DOI] [PubMed] [Google Scholar]
- 23. Disthabanchong S. Vascular calcification in chronic kidney disease: Pathogenesis and clinical implication. World journal of nephrology. 2012;1(2):43–53. 10.5527/wjn.v1.i2.43 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Kitahara T, Ono K, Tsuchida A, Kawai H, Shinohara M, Ishii Y, et al. Impact of brachial-ankle pulse wave velocity and ankle-brachial blood pressure index on mortality in hemodialysis patients. American journal of kidney diseases: the official journal of the National Kidney Foundation. 2005;46(4):688–96. 10.1053/j.ajkd.2005.06.016 . [DOI] [PubMed] [Google Scholar]
- 25. Jimenez ZN, Pereira BJ, Romao JE Jr., Makida SC, Abensur H, Moyses RM, et al. Ankle-brachial index: a simple way to predict mortality among patients on hemodialysis—a prospective study. PloS one. 2012;7(7):e42290 10.1371/journal.pone.0042290 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Merkus MP, Jager KJ, Dekker FW, de Haan RJ, Boeschoten EW, Krediet RT. Predictors of poor outcome in chronic dialysis patients: The Netherlands Cooperative Study on the Adequacy of Dialysis. The NECOSAD Study Group. American journal of kidney diseases: the official journal of the National Kidney Foundation. 2000;35(1):69–79. . [DOI] [PubMed] [Google Scholar]
- 27. O'Hare AM, Hsu CY, Bacchetti P, Johansen KL. Peripheral vascular disease risk factors among patients undergoing hemodialysis. Journal of the American Society of Nephrology: JASN. 2002;13(2):497–503. . [DOI] [PubMed] [Google Scholar]
- 28. Bohn E, Tangri N, Gali B, Henderson B, Sood MM, Komenda P, et al. Predicting risk of mortality in dialysis patients: a retrospective cohort study evaluating the prognostic value of a simple chest X-ray. BMC nephrology. 2013;14:263 10.1186/1471-2369-14-263 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Fishbane S, Youn S, Kowalski EJ, Frei GL. Ankle-arm blood pressure index as a marker for atherosclerotic vascular diseases in hemodialysis patients. American journal of kidney diseases: the official journal of the National Kidney Foundation. 1995;25(1):34–9. . [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
(XLS)
Data Availability Statement
All relevant data are within the paper and its Supporting Information files.