

Abstract
Objective. To explore the current status of pharmacy education in Thailand.
Methods. The International Pharmaceutical Federation of the World Health Organization’s (FIP-WHO) Global Survey of Pharmacy Schools was used for this study. The survey instrument was distributed to the deans of the 19 faculties (colleges) of pharmacy in Thailand.
Results. More than half the colleges have been in existence less than 20 years, and the government owns 80% of them. There were 2 paths of admission to study pharmacy: direct admission and central admission system. The doctor of pharmacy (PharmD) programs can be divided into 4 types. Approximately 60% of all teaching staff holds a doctoral degree. Regarding the work balance among teaching staff, around 60% focus on teaching activities, 20% focus on research, and less than 20% focus on patient care services concurrent with real practice teaching. The proportion of student time dedicated to theory, practice, and research in PharmD programs is 51.5%, 46.7%, and 1.8%, respectively. Sites owned by the colleges or by others were used for student training. Colleges followed the Office of the National Education Standards’ Internal Quality Assurance (IQA) and External Quality Assurance (EQA), and the Pharmacy Council’s Quality Assessment (ONESQA) .
Conclusion. This study provides a picture of the current status of curriculum, teaching staff, and students in pharmacy education in Thailand. The curriculum was adapted from the US PharmD program with the aim of meeting the country’s needs and includes industrial pharmacy and public health tracks as well as clinical tracks. However, this transition in pharmacy education in Thailand needs to be monitored and evaluated.
Keywords: pharmacy education, Thailand, PharmD, International Pharmaceutical Federation (FIP) Global Survey
INTRODUCTION
The World Health Organization (WHO) warned that the severe lack of a health workforce is a significant issue worldwide with no sign of change in sight.1 Thus, there is an urgent need to focus on increasing educational capacity and production of all types of health care providers.
The quantity and quality of educators and preceptors are both essential to the success of health professionals’ education.1,2 Globally, pharmacy educators face challenges in producing pharmacy graduates who meet stakeholder requirements for each country’s specific job market. This is more difficult in developing countries where there is a lack of resources, expertise, and infrastructure.3 The WHO, the United Nations Educational, Scientific and Cultural Organisation (UNESCO), and International Pharmaceutical Federation (FIP) Pharmacy Education Taskforce aims to promote needs-based education as a model for developing pharmacy education worldwide, which both improves global pharmacy education and is suitable for local application.3-5 Doctor of pharmacy programs are expected to produce pharmaceutical care experts and to provide more clinical experiences during training.6 There is much commentary about the merits and viability of adopting the PharmD program as an entry-level degree in developing countries, but it remains to be seen whether such a change would meet the true needs of those countries or simply follow international trends?4,6-8
Pharmacy education in Thailand began in 1923 during the reign of King Rama VI.9 Initially, pharmacy was only a part of the Faculty of Medicine at the Royal Medical School. In 1914, the first pharmacy school separated and became part of Chulalongkorn University.9,10 It was a 3-year program and graduates received a certificate of compounding, which then changed to a certificate of pharmacy after 1932 when the term “pharmacy” was adopted.9,10 During 1922-1936, the professional curriculum was developed, led by British pharmacist A. H. Hale.9 Pharmacy education expanded to a 4-year program in 1941, then to a 5-year bachelor of science in pharmacy in 1957, and between 1989 and 1990, courses were further developed to introduce the concept of clinical pharmacy.11,12
In 1993, the US-Thai consortium was developed, in which Thai pharmacy educators and practitioners participated to develop an academic workforce supported by the Ministry of University Affairs (now the Office of the Higher Education Commission, or OHEC). The collaboration was an impetus for pharmacy educators to develop PharmD programs, and the first Thai PharmD program was created at the Faculty of Pharmaceutical Sciences at Naresuan University in 1999. This program was also the first curriculum of its kind in Asia.9,13,14
A 6-year PharmD program was proposed by the Pharmacy Education Consortium of Thailand (PECT) in 1993 and at the First National Pharmaceutical Education Forum in 1994, but it was not implemented until 2008 by the Pharmacy Council of Thailand.15,16 The council made the 6-year program a compulsory perquisite for pharmacy licensure during 2014 because it believed the 6-year program would help move pharmacy competencies from generalist to specialist and thus meet the required needs of the job market, solve the curriculum overload (ie, extend the high number of required credits over 6 years instead of 5 years), and provide the same standards within the pharmacy profession throughout Thailand.9,15 The council expected the transition from bachelor of pharmacy (BPharm) to PharmD not only to extend the duration of the program by 1 year but also to include a reconstructed curriculum that would produce graduates who could perform competently in the health care system.7, 17
Thai pharmacists are still involved in many settings such as pharmaceutical manufacturing (eg, drug production, quality control, research, and development), pharmaceutical enterprises (eg, pharmacy marketing) and public health (eg, law and regulations, consumer protection).9,18 The 6-year PharmD curriculum in Thailand is designed to prepare Thai pharmacy graduates to handle diverse responsibilities in different practice settings. Pharmacy education in Thailand has undergone a significant transition and will have only PharmD graduates from 2014 onwards.9 There has been no research into the current status of the pharmacy education workforce for the PharmD programs in Thailand. The objective of this study was to explore the current status of pharmacy education in Thailand, thus aiming to provide a better understanding of the pharmacy education workforce within the country.
METHODS
The original FIP global pharmacy education survey was validated and developed in collaboration with the FIP Collaborating Centre at the University College London, the School of Pharmacy at the University of Nottingham, and the FIPEd and WHO Human Resources for Health staff. The global survey aimed to collect the educational background of pharmacy students prior to registration as licensed pharmacists and pharmacy educators, as well as to collect the quality assurance accreditation mechanisms. The findings were used to identify workforce shortages and collaboration opportunities and to provide evidence-based information needed for policy development. Respondents included FIP member organizations, country level contacts in education, and associations from 109 countries and territories. The FIPEd survey was conducted in English and other languages (eg, Arabic, Chinese, French, Japanese, Portuguese, and Spanish) between January 2012 and April 2013. The results represented 175 000 pharmacy students and 2500 educational institutions and are available in the 2013 FIPEd Global Education Report.19, 20
This study received permission from FIPEd to use the original English version of the survey. Translations and cross-cultural adaptations to Thai language were allowed. The details of forward-backward translation21-24 are as follows: the questionnaire was forward translated into a Thai language version by 2 bilingual Thai translators, using a symmetrical translation approach and was checked by another bilingual pharmacy academic. Agreement on the veracity of the forward-translated version was reached by all translators using 2 criteria: (1) clarity and ease of understanding of the translation (2) conceptual equivalence. The questionnaire was then processed 100% blind-backward translation from Thai into English by the bilingual Thai-English speaker. The backward translation (English) was reviewed for conceptual equivalence with the forward translation (Thai version). Researchers confirmed Thai and English language consistency. Two English versions (original and backward translation) were considered by a FIPEd expert. Then, a consensus among researchers was reached on the final translation.
The survey was divided into 2 parts. Part 1 covered details of the college or school, such as a list of academic programs offered, types and qualifications of teaching staff, number of students who enrolled, left the program, or graduated between 2009 and 2012, maximum capacity for new admissions, requirements for admission, and descriptions of sites for student training. Part 2 covered quality assurance and included questions regarding quality assurance mechanisms and processes, and continuing education for graduated professionals. The researchers also asked for the related documents each school used to fill out the survey. Respondents were typically the dean or the deputy dean for academic affairs. The survey took about 3 hours to complete because information was required from various other faculty members (eg academic, quality assurance, and clerkship staff who arrange the rotations).
All 19 universities providing pharmacy programs were contacted by conventional or electronic mail and asked to complete the survey. A cover letter, survey instrument, and self-addressed stamped return envelope were mailed to them. Six weeks later, a follow-up e-mail and new cover letter were sent to those who hadn’t responded to the initial mailing. To increase the response rate, the survey instrument was sent three times and respondents were offered £20 as an incentive. The incentive amount was based on rate of overtime compensation suggested by the Ministry of Finance.25
To ensure the accuracy of the information in this study, respondents were asked to include documents relevant to pharmacy education and the academic programs they described in the survey (eg, quality assurance reports, self-assessment reports, curriculum, list of academic staff and students, research, and article references). The survey data were compared to these documents as well as with other publicly accessible documents. The data analysis was based on the best available validated data checked by the researchers.20 Data were entered into Microsoft Excel and percentages were calculated. Data from open-ended questions were coded for quantitative analysis. Respondents were asked about any missing data, and percentages of missing data and discussion about possible reasons for missing data were presented. Ethical approval for this study was granted by the Faculty of Sciences, University of Nottingham, United Kingdom.
A pilot study with a dean of one of the colleges of pharmaceutical sciences in Thailand was undertaken to determine what resources were needed to answer the survey questions and to identify practical problems. The dean was also asked to identify any difficult or confusing items. The dean’s responses and the time taken to complete each part of the survey were noted. Then the translation was revised as needed. The pilot results were included in the main results.
RESULTS
The response rate was 84.2% (n=16). Table 1 summarizes the characteristics of the colleges of pharmacy that responded to this survey. Most colleges were located in the central part of Thailand. More than half of the colleges have been in existence for less than 20 years and the government owned 80% of them. There were 2 paths of admission to pharmacy programs: through direct admission or the central admission system. The direct admission process, through which candidates could apply to the university directly, might recruit students to about 60% of capacity for new admissions. The criteria included cumulative Grade Point Average (CGPA), total General Aptitude Test (GAT) scores, Professional Aptitude Test (PAT) scores, physical examination, and color blindness test. The other path was through the central university admission system managed by the Commission on Higher Education. It recruited students to about 40% of capacity for new admissions. The criteria are the same as direct admission system but also include Ordinary National Educational Test (O-NET).
Table 1.
Characteristics of the Colleges of Pharmacy Surveyed (n=16)
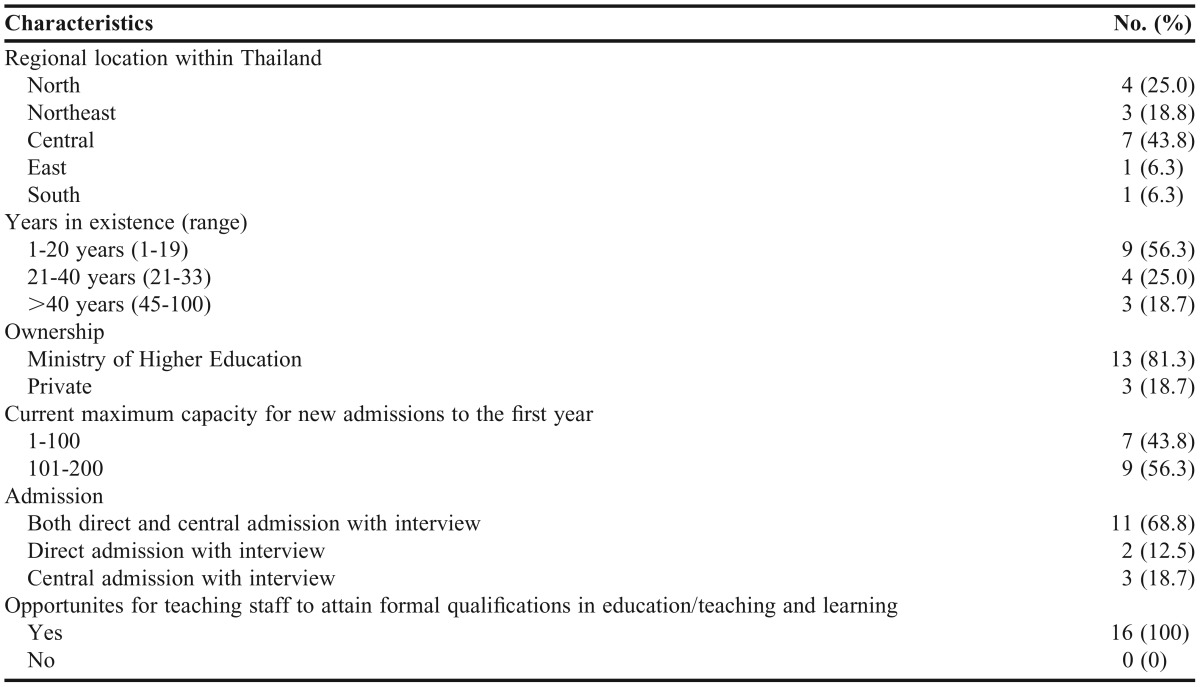
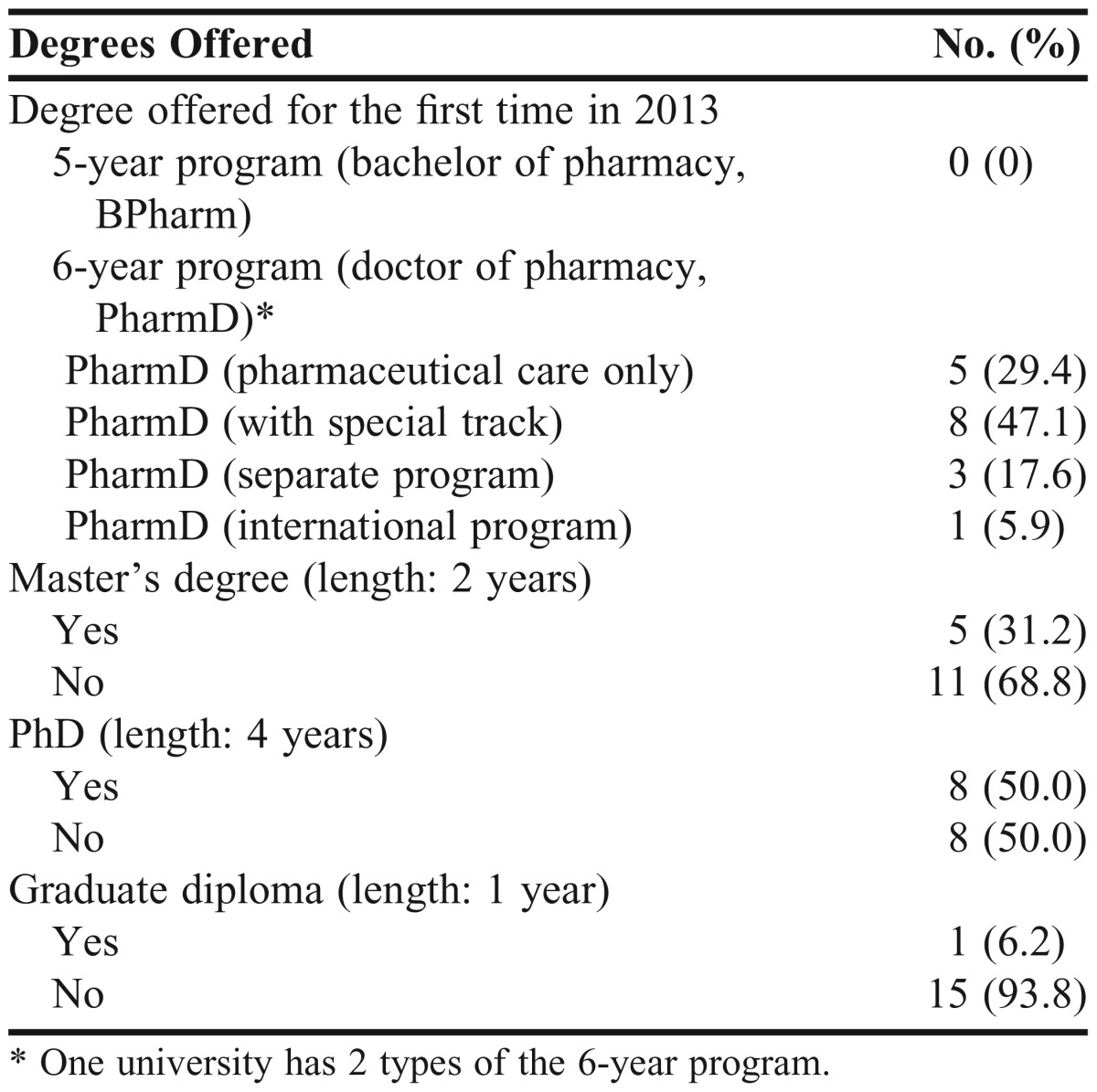
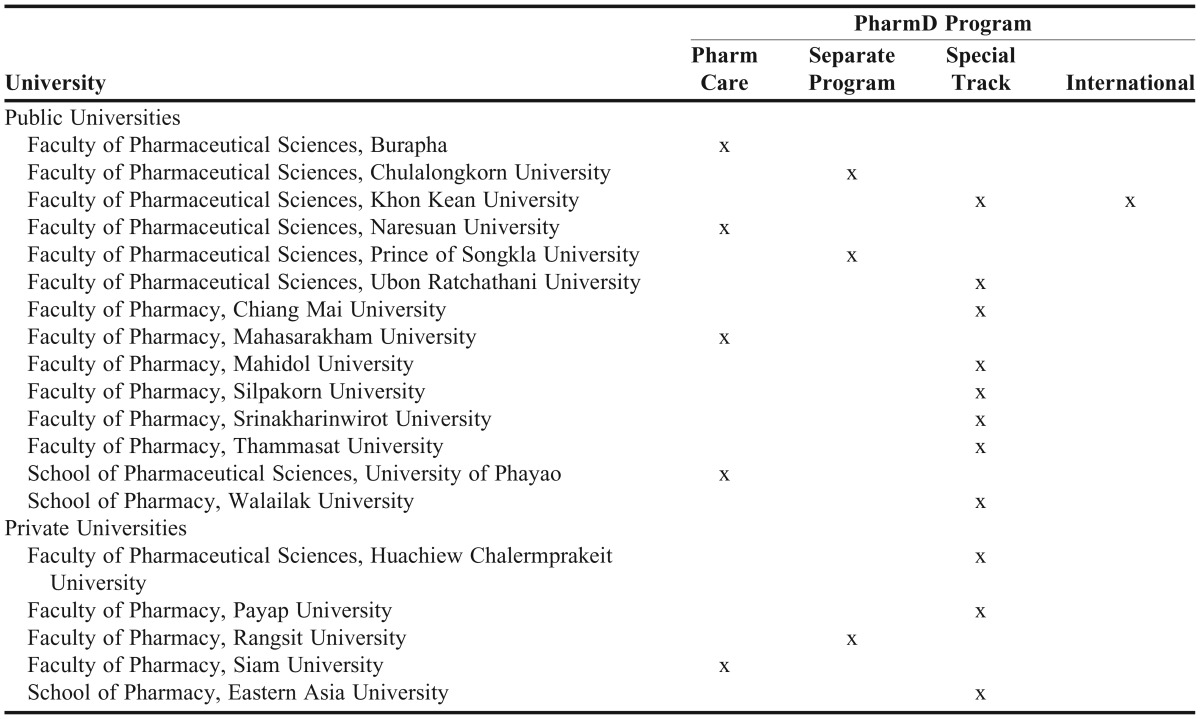
Table 2 provides the number of the types of degree offered. The PharmD programs can be divided into 4 types: (1) PharmD (pharmaceutical care program only); (2) PharmD with 2 to 4 specialized tracks chosedn in the fourth year (eg, industrial pharmacy—an official name used by The Pharmacy Council of Thailand instead of pharmaceutical sciences, pharmaceutical care, primary pharmacy and consumer health protection, pharmaceutical and health informatics, etc.); (3) PharmD separate program, for which course of study is chosen during the admissions process (eg, industrial pharmacy, which includes 4 parts: research and development, quality assurance and quality control, manufacturing and regulatory affairs, and product registration and PharmD pharmaceutical care); (4) PharmD international program, applicants for which might have been students coming from international schools in Thailand or from schools in foreign countries. This program was taught in English but had the same setting, resources, and curriculum as the Thai language program and was managed in conjunction with a PharmD program taught in Thai.
Table 2.
Degrees Offered in Academic Year 2013 in 16 Pharmacy Colleges
Characteristics of the teaching staff from the colleges of pharmacy surveyed are shown in Table 3. The majority (90%) of the teaching staff were full time Thai nationals. More than half of the total staff was female. Approximately 60% of all teaching staff held a doctoral degree. Less than 2% of staff completed a residency. Concerning the work balance among teaching staff, an average of 60% from 4 years of responses focused on teaching activities, 20% focused on research, and less than 20% focused on patient care services in real practice settings such as hospitals or community pharmacies. The trend towards patient care-focused workload increased over the past few years because all colleges were providing a PharmD program.
Table 3.
Characteristics of Teaching Staff from the Colleges of Pharmacy Surveyed (n=15, missing data=1)
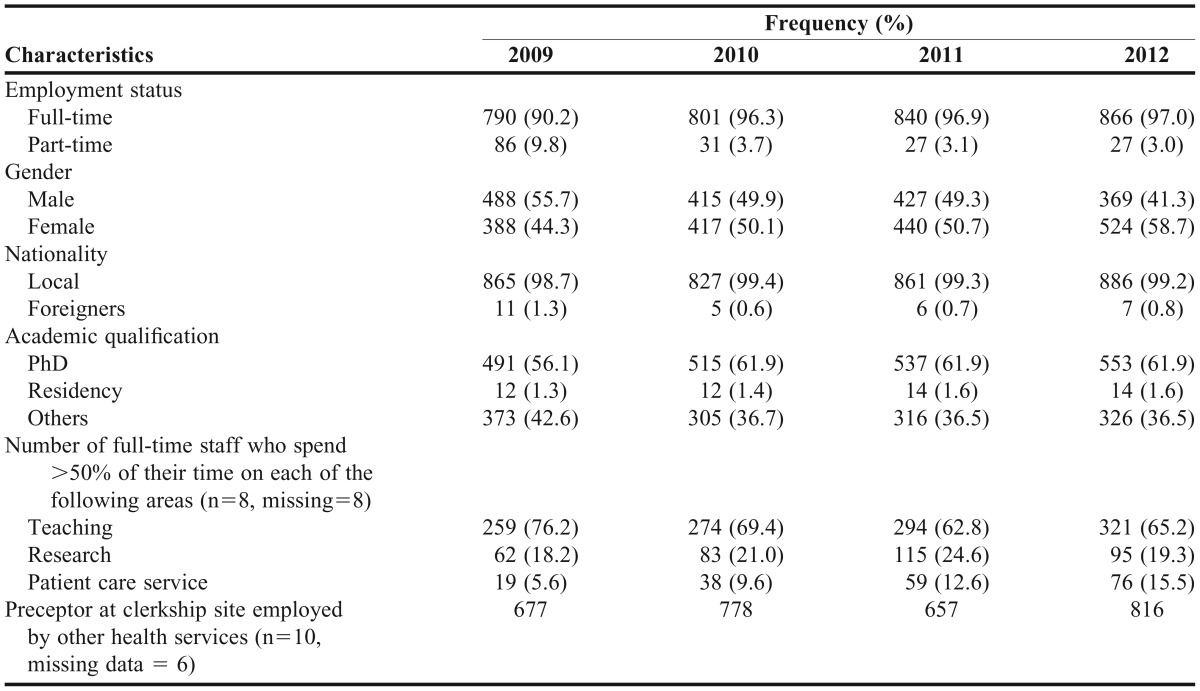
From 8 sets of missing data, 4 colleges responded that they could not place their staff into the 3 categories described in the questionnaire: teaching activities, research, and patient care service. It should be noted that Thai universities/institutions have 4 primary missions to perform as follows: (1) Teaching and learning aim to provide knowledge and skills to students to achieve success in their lives; (2) Research among academic staff is encouraged to support the country’s development; (3) Providing academic services aims to provide various kinds of academic services to the community and encourage community development; (4) Preservation of art and culture aims to promote, conserve, and maintain the traditions and values of Thai culture. One university revealed that the teaching staff all had equivalent responsibility for each of these 4 main tasks.
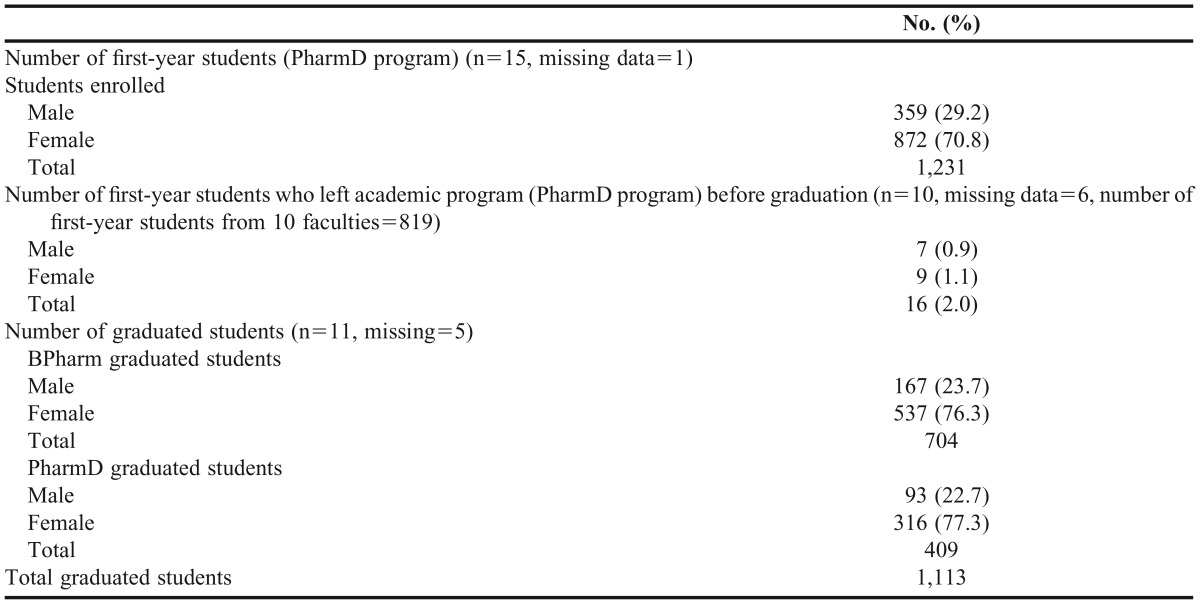
The number of first-year students enrolled at 15 universities in 2012 was 1231. Sixteen students from 10 universities left before graduation and the number of pharmacy graduates in 2012 from 11 universities was 1113 (Table 4).
Table 4.
Overview of Student Enrollment, Drop-out and Graduation Rates in 2012
Pharmacy education in Thailand is in a period of major transition. The majority of the universities used to offer a 5-year BPharm program that consisted of a number of different tracks including pharmaceutical technology, pharmaceutical care, and social pharmacy. However, the BPharm program was not offered after 2010 because the Pharmacy Council of Thailand implemented a policy in 2008 that a 6-year PharmD would be compulsory for pharmacy licensure starting in 2014. Any BPharm students remaining in the educational system graduated in 2013.
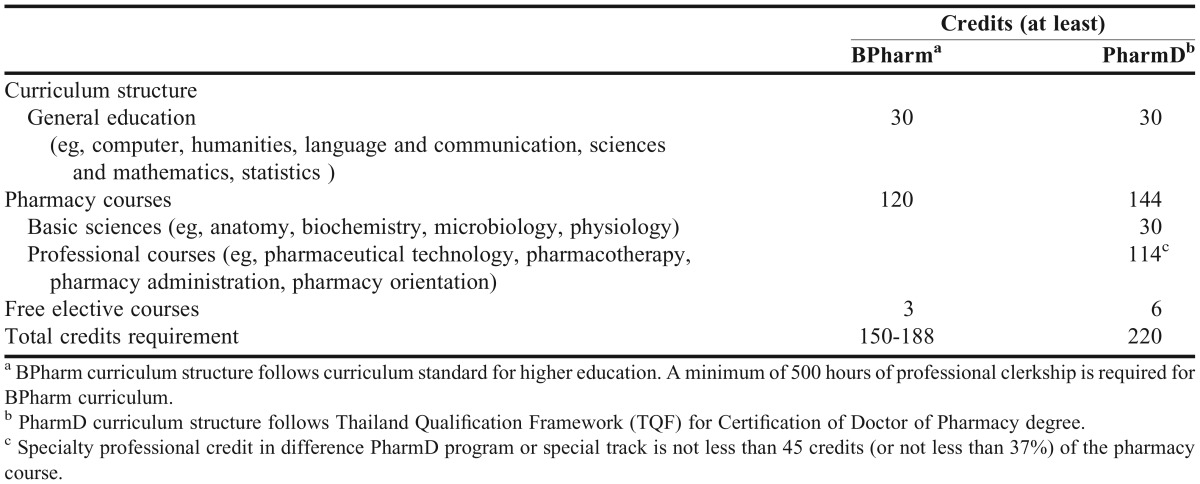
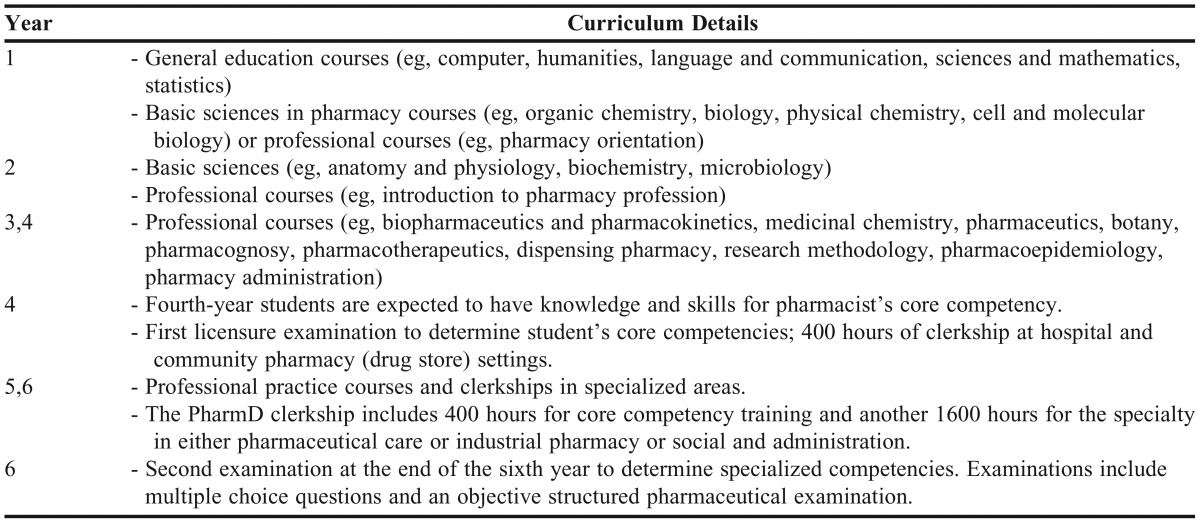
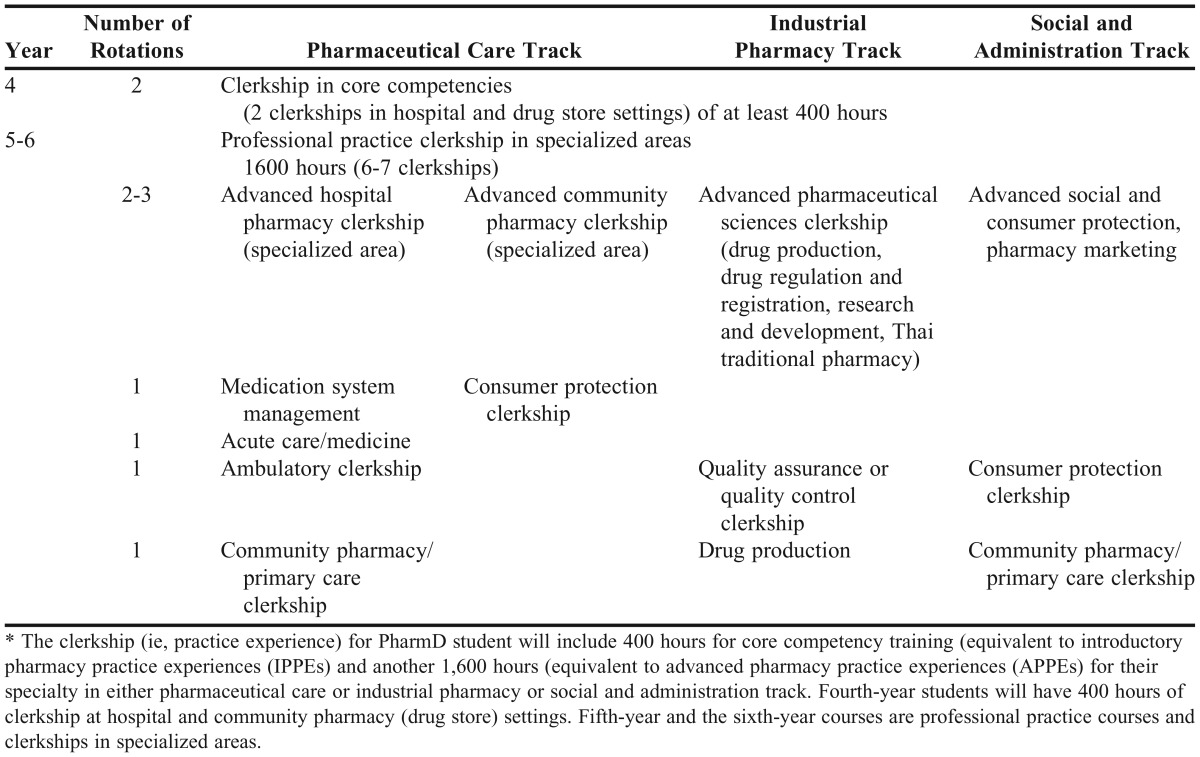
All 6-year pharmacy courses in Thailand complied with the core pharmacy course structure guidelines as recommended by the Pharmacy Council of Thailand with not less than 140 credit hours for professional content. During the first 4 years, the curriculum provided students with core competencies for professional practice. In the last 2 years, pharmacy students selected their specialties. During the fifth year, students had course work and the sixth year consisted of specialized clerkships similar to various American pharmacy practice experiences. Clerkship experiences needed to be 2000 practice hours. Students had the first 400-hour clerkship at the end of the fourth year. These practice experiences in the areas of hospital pharmacy and community pharmacy (ie, drugstores) were compulsory for all pharmacy students. The remaining professional practice time depended on each individual’s interest (eg, hospital, community, research and development, manufacturing, regulation and jurisdiction). The proportion of student time dedicated to theory, practice, and research in PharmD programs was 51.5%, 46.7% and 1.8%, respectively (Table 5).
Table 5.
Proportion of Student Credit Hours in Theory, Practice, and Research in PharmD programs (n=13, missing data=3)

Student training sites were owned by both the colleges and by external entities (Figure 1). The medication system clerkship was at the time a new clerkship (eg, conceptual framework of hospital accreditation, observation of policy, and management decision making), which was mandated by a policy of the Pharmacy Council of Thailand. This clerkship was only for the students who studied the pharmaceutical care track; therefore, some faculties did not offer this clerkship.
Figure 1.

Ownership of Training Sites (n=16).
The quality assurance system had tw2o components, internal and external. Internal quality assurance (IQA) was the responsibility of each educational institution and followed the policy of OHEC (under the Ministry of Education). Assessment and evaluation occured mostly once a year (n=14, 88%). External quality assurance (EQA) was overseen by the Office of the National Education Standards and Quality Assessment (ONESQA), a public organization not associated with the Ministry of Education. Inspections were conducted every 3-5 years. Ten colleges underwent EQA every 3-5 years (62%) and 6 colleges underwent EQA every year (38%).
Under the Pharmacy Education Committee of the Pharmacy Council of Thailand, a quality assurance system was developed for the accreditation of pharmacy graduates in each pharmacy school via 2 main processes: (1) curriculum and institution accreditation and; (2) pharmacy license examination. Accreditation aimed to ensure that graduates were of high quality. The frequency of institutional accreditation by the Pharmacy Council was once every 5 years for established schools and once a year for new schools. New colleges of pharmacy changed their accreditation to once every 5 years when 50% of their graduates passed the licensure examination for 3 consecutive years. All colleges were accredited by the Pharmacy Council of Thailand (n=16, 100%).
DISCUSSION
This study showed that all colleges offered a 6-year PharmD program in 2012. The PharmD program in Thailand with 4 tracks (pharmaceutical care, industrial pharmacy, specialized tracks, and an international program) differs from the PharmD model in the United States, which offers a patient-focused curriculum,26-28 as well as from models in countries such as India, Jordan, and Japan, which only offer a PharmD in pharmaceutical care.29-31 The Thai PharmD curriculum is, however, similar to that of countries such as Pakistan, which offers a clinical PharmD and doctor of pharmaceutical technology,32 or South Korea, where students might have 12 elective credits for their specified track (eg, clinical pharmacy, industrial pharmacy, or pharmacy research).33
The shortage of qualified professional practice educators in Thailand might affect the scaling up and transformation of health professionals’ education, including pharmacy.1 For example, the percentage of instructors who focused on patient care (15.5%) in 2012 was relatively low when compared with the percentage of US pharmacy faculty members in the pharmacy practice discipline (52%).2 There is a need to bridge the gap between teaching and practice. Policy makers might consider facilitating staff development for clinical work and development of more clinical teaching or teacher practitioner roles by providing new career structure, incentives, or reward systems.1 While the new PharmD program in Thailand is more clinically oriented, more residency programs could be the key in bridging that gap. Residents have postgraduate experiences that enhance competency and might be in the position to help develop new roles, contribute to the improvement of the pharmacy profession, and be role models for students, pharmacists, and preceptors.34 Some colleges are already planning to develop new staff for PharmD residency programs to support their PharmD curriculum.
Before 1994, there were 6 public colleges of pharmacy in Thailand. After 1994, many additional colleges of pharmacy were formed, both in public and private universities. Now, there are 19 universities providing pharmacy education in Thailand (14 in public universities and 5 in private universities). All colleges have an internal and external quality assurance system, as well as accreditation from the Pharmacy Council of Thailand. The accreditation criteria help control admission capacity, prepare the faculty facilities, and manage laboratory safety.35, 36
The data collected show the current status of pharmacy education in Thailand but further studies could be carried out that consider the WHO guideline of transforming and scaling up health professionals’ education and training.1 Areas to investigate might be the cost of such a scaling up for both colleges and students, accreditation of preceptor sites, monitoring and evaluation of the pharmacy workforce after graduation, and how implementation of the proposed changes would be planned and what policies would govern them.
Qualified preceptors and expert training sites are key success factors for the PharmD programs. However, most preceptors are currently volunteers, and there was weak evidence regarding training site accreditation. The professional regulatory bodies might need to consider reviewing this situation.1
Normally, Thai pharmacists in hospitals have a high workload dedicated to high prescription volumes. This is one barrier to practicing effective and efficient pharmaceutical care, which is the same challenge pharmacists experienced in Japan.29 It will be interesting to observe how the first groups of PharmD graduates—who are expected to have higher competencies—will practice in their new roles and interact with traditional BPharm pharmacists and the rest of the health care team.
Policy makers and stakeholders might consider quality assurance, competency, and academic and institutional capacity as pharmacy education changes in Thailand.37 Revisiting these factors might help ensure that pharmacy education provides the necessary competencies for graduates to perform the pharmaceutical services needed in the country.
A significant transition requires cooperation between colleges of pharmacy, pharmacy councils, government, and pharmacists already in the workforce to encourage better pharmacy education in terms of quality of the curriculum, curriculum validation, competencies of pharmacy graduates, training (eg, training site accreditation, preceptor development plan). Further studies are needed to determine obstacles to the transitional process, how workforce planning links to pharmacist production, and what role other stakeholder opinions play regarding these changes.
CONCLUSION
This study provides a picture of the current status of curriculum, teaching staff, and students in pharmacy education in Thailand. The Thai PharmD curriculum, which differs from the US PharmD curriculum, was adapted with the aim to meet the country’s needs and includes industrial pharmacy and public health tracks as well as clinical tracks. However, pharmacy education in Thailand needs to be monitored and evaluated. It should have a long-term strategy to ensure the quantity and quality of pharmacy graduates emerging from the new PharmD program.
ACKNOWLEDGMENTS
The researchers would like to thank the Thai Royal Government for the funds granted to undertake this research and The International Pharmaceutical Federation Education Initiatives (FIPEd) for their permission to adapt the original English version of the FIP-WHO Global Survey of Pharmacy Schools. The authors would like to thank the Faculties of Pharmacy in Thailand for their kind participation, Dr. Nonglek Kunwaradisai for her forward translation, Ms. Wiwan Worakulpanich for administering the survey, and Ms. Mayuree Tangkiatkumjai for her valuable suggestions.
Appendix 1.
The Official Name of Faculties (Colleges) of Pharmacy Surveyed and Types of PharmD Programs Offered
Appendix 2. Curriculum Structure for a 6-year PharmD Program
Curriculum Structure of a 5-year BPharm Curriculum and a 6-year PharmD Curriculum
Structure Guideline of a 6-year PharmD Curriculum in Thailand for Students Starting in 2015.38

Curriculum Details of a 6-year PharmD Curriculum in Thailand38
Appendix 3.
Clerkship* Structure of PharmD Program for Each Special Track
REFERENCES
- 1.WHO. Transforming and scaling up health professionals’ education and training: World Health Organization Guidelines 2013. The World Health Organization. http://apps.who.int/iris/bitstream/10665/93635/1/9789241506502_eng.pdf?ua=1. Accessed November 1, 2013.
- 2.Beardsley R, Matzke GR, Rospond R, et al. Factors influencing the pharmacy faculty workforce. Am J Pharm Educ. 2008;72(2) doi: 10.5688/aj720234. Article 34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Anderson C, Bates I, Brock T, et al. Needs-based education in the context of globalization. Am J Pharm Educ. 2012;76(4) doi: 10.5688/ajpe76456. Article 56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Anderson C, Futter B. PharmD or needs-based education: which comes first? Am J Pharm Educ. 2009;73(5) doi: 10.5688/aj730592. Article 92. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.FIP. 2012 FIP Global Pharmacy: Workforce report. International Pharmaceutical Federation (FIP). http://www.fip.org/static/fipeducation/2012/FIP-Workforce-Report-2012/?page=hr2012. Accessed December 10, 2013.
- 6.Ahmed SI, Hassali MAA. The controversy of PharmD degree. Am J Pharm Educ. 2008;72(3) doi: 10.5688/aj720371. Article 71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Babar Z, Scahill SL, Akhlaq M, Garg S. A bibliometric review of pharmacy education literature in the context of low-to middle-income countries. Currents Pharm Teach Learn. 2013;5(3):218–232. [Google Scholar]
- 8.Khan T, Anwar M, Ahmed KM. A perspective for clinical pharmacy curriculum development and validation in Asian developing nations. J Young Pharm. 2011;3(2):151–154. doi: 10.4103/0975-1483.80304. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Pongcharoensuk P, Prakongpan S. Centennial pharmacy education in Thailand. JAASP. 2012;1(1):8–15. [Google Scholar]
- 10.Faculty of Pharmacy Mahidol University. Brief History of Pharmacy Education in Thailand. http://www.pharmacy.mahidol.ac.th/eng/aboutus.php. Accessed March 14, 2014.
- 11.Kapol N, Maitreemit P, Pongcharoensuk P, Armstrong E. Evaluation of curricula content based on Thai pharmacy competency standards. Am J Pharm Educ. 2008;72(1) doi: 10.5688/aj720109. Article 9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Chan RC, Ching PL. Pharmacy practice in Thailand. Am J Health Syst Pharm. 2005;62(1):1408–1411. doi: 10.2146/ajhp040393. [DOI] [PubMed] [Google Scholar]
- 13.Sonthisombat P. Pharmacy student and preceptor perceptions of preceptor teaching behaviors. Am J Pharm Educ. 2008;72(5) doi: 10.5688/aj7205110. Article 110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Srisopa S, Asuphon O, Montakantikul P. Role of clinical pharmacists for managing infectious diseases in Thailand. J Infect Dis Antimicrob Agents. 2012;29(3):105–112. [Google Scholar]
- 15.Pramyothin P, Sripanidkulchai B, Thirawarapan S, Khunkitti W. Strategies for Managing Pharmacy Education in the Next Two Decades. Ministry of University Affairs; Thailand: 1999. [Google Scholar]
- 16. The Royal Thai Government Gazette Vol 125 SPN, dated 3rd April. The Pharmacy Council of Thailand’s regulation about accredited pharmacy degree http://pharmacycouncil.org/share/file/file_269.pdf. Accessed March 12, 2014.
- 17.American Association of Colleges of Pharmacy. Commission to implement change in pharmaceutical education. American Association of Colleges of Pharmacy (AACP). http://www.aacp.org/resources/historicaldocuments/Documents/COMMISSPOSPAPER3.pdf. Accessed December 1, 2013.
- 18.Anderson C. Education trends, innovations and transformations - case studies. International Pharmaceutical Federation (FIP). http://www.fip.org/files/fip/PharmacyEducation/2013_FIPEd_Global_Education_Report_final.pdf. Accessed October 1, 2013.
- 19.Anderson C, Bates I, Brock T, et al. Highlights from the FIPEd Global Education Report. Am J Pharm Educ. 2014;78(1) doi: 10.5688/ajpe7814. Article 4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Bates I, Bruno A, Arakawa N. Global education description: 2013 FIPEd Global Education Report. International Pharmaceutical Federation. http://www.fip.org/files/fip/FIPEd_Global_Education_Report_2013.pdf. Accessed March 6, 2014.
- 21.Chen H, Boore JR. Translation and back-translation in qualitative nursing research: methodological review. J Clin Nurs. 2010;19:234–239. doi: 10.1111/j.1365-2702.2009.02896.x. [DOI] [PubMed] [Google Scholar]
- 22.Lopez GI, Figueroa M, Connor SE, Maliski SL. Translation barriers in conducting qualitative research with Spanish speakers. Qual Health Res. 2008;18(12):1729–1737. doi: 10.1177/1049732308325857. [DOI] [PubMed] [Google Scholar]
- 23.Van Nes F, Abma T, Jonsson H, Deeg D. Language differences in qualitative research: is meaning lost in translation? Eur J Ageing. 2010;7:313–316. doi: 10.1007/s10433-010-0168-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Feng-bin L, Yong-xing J, Yu-hang W, Zheng-kun H, Xin-lin C. Translation and psychometric evaluation of the Chinese version of functional digestive disorders quality of life questionnaire. Dig Dis Sci. 2014;59:390–420. doi: 10.1007/s10620-013-2897-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Grant RW, Sugarman J. Ethics in human subjects research: do incentives matter? J Med Phil. 2004;29(6):717–738. doi: 10.1080/03605310490883046. [DOI] [PubMed] [Google Scholar]
- 26.Nemire RE, Meyer SM. Educating students for practice: educational outcomes and community experience. Am J Pharm Educ. 2006;70(1) doi: 10.5688/aj700120. Article 20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.New J, Garner S, Ragucci K, Spencer A. An advanced clinical track within a Doctor of Pharmacy program. Am J Pharm Educ. 2012;76(3) doi: 10.5688/ajpe76343. Article 43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Bradberry JC, Droege M, Evans RL, et al. AACP Report: curricula then and now - an environmental scan and recommendations since the commission to implement change in pharmaceutical education: Report of the 2006-2007 Academic Affairs Committee. Am J Pharm Educ. 2007;71(4) Article S10. [Google Scholar]
- 29.Dolder C, Nakagawa S, Sakamaki A. Changes in Japanese pharmacy education and practice. Am J Health Syst Pharm. 2008;65(3):201–202. doi: 10.2146/ajhp070422. [DOI] [PubMed] [Google Scholar]
- 30.Basak SC, Sathyanarayana D. Pharmacy education in India. Am J Pharm Educ. 2010;74(4) doi: 10.5688/aj740468. Article 68. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Al-Wazaify M, Matowe L, Albsoul-Younes A, Al-Omran OA. Pharmacy education in Jordan, Saudi Arabia, and Kuwait. Am J Pharm Educ. 2006;70(1) doi: 10.5688/aj700118. Article 18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Khan TM. Glimpse of pharmacy education in Pakistan and current challenges to pharmacy education. IJPTP. 2010;1(1):5–10. [Google Scholar]
- 33.Kim E, Ghimire S. Career perspectives of future graduates of the newly implemented 6-year pharmacy educational system in South Korea. Am J Pharm Educ. 2013;77(2) doi: 10.5688/ajpe77237. Article 37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.American Association of Colleges of Pharmacy. AACP commission to implement change in pharmaceutical education: The responsibility of pharmaceutical education for scholarship, graduate education, fellowships, and postgraduate professional education and training. http://www.aacp.org/resources/historicaldocuments/Documents/BackgroundPaper4.pdf. Accessed December 1, 2013.
- 35.Wongpoowarak P. The Pharmacy Education Committee of Pharmacy Council of Thailand Report. http://www.pharmacycouncil.org/index.php?option=content_detail&view=detail&itemid=359. Accessed December 1, 2013.
- 36.The Pharmacy Council of Thailand. List of the accredited pharmacy programme in Thailand. http://www.pharmacycouncil.org/index.php?option=content_detail&view=detail&itemid=406. Accessed March 16, 2014.
- 37.Anderson C, Bates I, Beck D, et al. The WHO UNESCO FIP Pharmacy Education Taskforce. Hum Resour Health. 2009;7(45) doi: 10.1186/1478-4491-7-45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.The Pharmacy Council of Thailand. The core pharmacy course structure guideline. http://www.pharmacycouncil.org/share/file/file_193.pdf. Accessed October 10, 2013.