

Abstract
Isolation of the right subclavian artery (RSCA) is rare, and this finding in association with d-transposition of the great arteries (d-TGA) is extremely unusual. We present a case of an isolated RSCA in a newborn with d-TGA in whom the clinical presentation was diagnostic. We discuss the imaging modalities used to confirm the diagnosis, the embryological basis of the finding, and the surgical repair.
Keywords: Anomalous origin of right subclavian artery, congenital heart disease, isolated right subclavian artery, transposition of the great arteries
INTRODUCTION
Isolation of the right subclavian artery (RSCA) is a rare anomaly in which the RSCA arises from the pulmonary artery via a ductus arteriosus, usually with a right aortic arch and lesions associated with a right arch, such as tetralogy of Fallot.[1] The presence of an isolated RSCA arising from the pulmonary artery in association with d-transposition of the great arteries (d-TGA) is extremely unusual, with few cases previously reported in the literature.[2,3,4,5] We illustrate a case in which the clinical presentation was diagnostic, and discuss the imaging modalities used to confirm the diagnosis, the embryological basis of the finding, and implications for surgical repair.
CLINICAL SUMMARY
The patient was a full-term, 3.7 kg male newborn with a fetal echocardiogram performed at 22 weeks gestational age revealing d-TGA with an intact ventricular septum. He was born via repeat cesarean section with Apgars 8 and 8 at 1 and 5 min, respectively. After transfer to the intensive care unit, initial pulse oximetry demonstrated a right arm saturation of 99%; while right ear, left arm, and right leg saturations ranged from 50 to 60%. Arterial blood gas sampling revealed a partial pressure of oxygen (paO2) of 148 mmHg from a right radial arterial puncture and paO2 of 24 mmHg from the indwelling umbilical arterial catheter. The right arm and shoulder demonstrated a well-demarcated pink appearance; his face, left arm, and rest of the body remained deeply cyanotic. An initial transthoracic echocardiogram was performed (Phillips iE33, Phillips Medical Systems, Bothell, WA, USA) and confirmed the diagnosis of d-TGA with a restrictive atrial communication. Balloon atrial septostomy was performed with ultrasound guidance at the bedside. The atrial septum was subsequently seen to be widely patent and the right ear, left arm, and right leg oxygen saturations increased to 85%. The right arm remained 99 to 100% saturated, a finding diagnostic of a RSCA arising from the pulmonary artery in d-TGA.
Further detailed echocardiographic imaging revealed a left-sided aortic arch with the first head and neck vessel from the aorta coursing rightward and superiorly without bifurcation. A vessel with pulsatile flow by spectral Doppler appeared to arise from the proximal right pulmonary artery and course rightward, suggesting an isolated RSCA arising from the pulmonary artery [Figure 1 and Video 1]. Contrast-enhanced magnetic resonance imaging (MRI) with thin-slab three-dimensional surface rendering was performed the following day, confirming the origin of the RSCA from a ductus arteriosus arising from the proximal right pulmonary artery [Figure 2].
Figure 1.
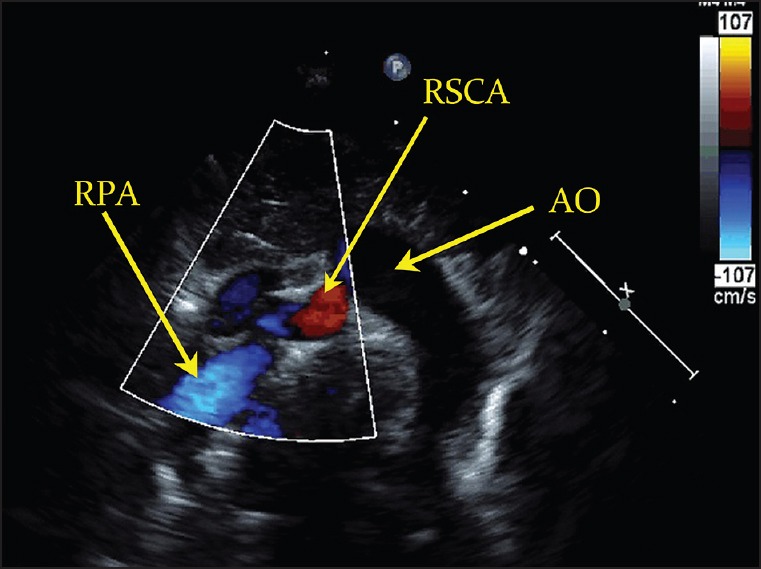
Transthoracic echocardiogram demonstrating a vessel arising from the proximal right pulmonary artery (RPA) and coursing superior and rightward, suggestive of an anomalous origin of the right subclavian artery (RSCA). AO = Aorta
Figure 2.
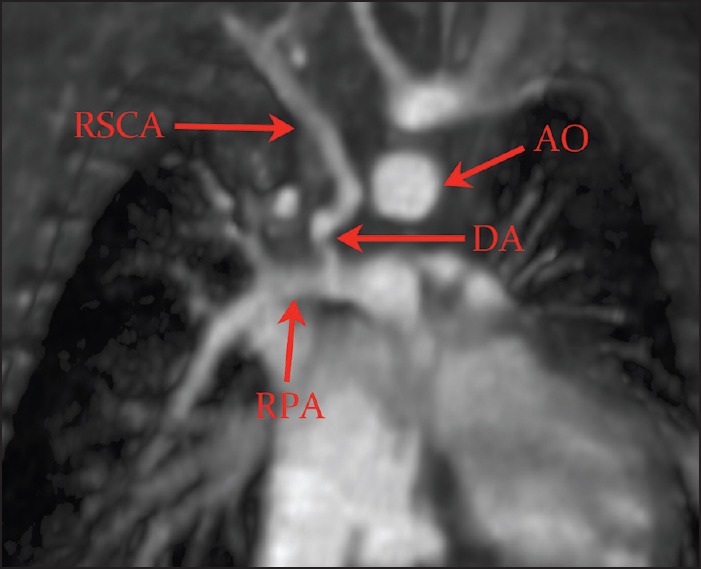
Thin-slab three-dimensional surface rendering magnetic resonance imaging confirming the isolated RSCA from a right ductus arteriosus (DA) arising from the proximal RPA
The patient subsequently underwent arterial switch operation at 5 days of life. Intraoperatively, the RSCA was found to arise from the right pulmonary artery via a long segment of ductal tissue [Figure 3]. The right ductus arteriosus was ligated, the ductal tissue from the RSCA was trimmed, and the artery was anastomosed to the right common carotid artery. The postoperative course was complicated by an atrial reentrant tachycardia controlled by beta-blockade, with otherwise stable hemodynamics and normal perfusion and mobility of the right arm. Postoperative echocardiogram revealed no gradient from the right common carotid artery to the RSCA. Simultaneous four-limb blood pressures demonstrated no differential between the right arm, left arm, and legs.
Figure 3.
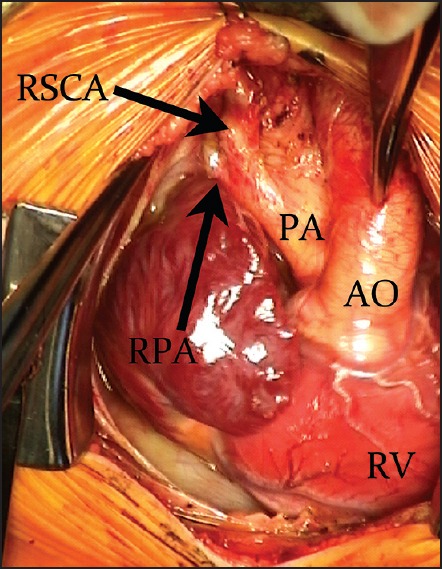
Intraoperative image of the RSCA connected to the RPA via a long segment of ductal tissue. RV = Right ventricle
DISCUSSION
The finding of an isolated RSCA can be described embryologically on the basis of Edwards’ hypothetical double arch.[6] During normal embryonic development, the arteries supplying the head, neck, and arms are formed by the migration and dissolution of the pharyngeal arches, which extend symmetrically to reach the dorsal aorta.[7] Anderson et al. have demonstrated in embryonic mouse hearts that the intrapericardial component of the pulmonary arteries are formed within the distal part of the outflow tract, while the extrapericardial component of the right and left pulmonary arteries are formed within the pharyngeal mesenchyme from the sixth (VI) aortic arch, as illustrated in Figure 4a.[8] During normal development, there is cranial migration of the right seventh (VII) intersegmental artery, eventually becoming the RSCA arising from the brachiocephalic trunk, which itself is believed to arise from the right fourth (IV) aortic arch.[7,9] Typically, the distal components of the right IV and VI arches regress, with the left IV arch becoming the definitive aortic arch, and the left VI arch persisting as the patent ductus arteriosus, illustrated in Figure 4a. However, dissolution of the right IV aortic arch with persistence of the distal right VI arch forming the right ductus arteriosus and pulmonary artery can lead to isolation of the RSCA, as illustrated in Figure 4b. The RSCA then arises from the pulmonary artery via the right ductus arteriosus rather than from the aorta via the right IV aortic arch. Of note, isolated brachiocephalic arteries have also been described, which can be explained by an interruption in the arch distal to the ductus arteriosus and a second interruption proximal to the common carotid artery.[10]
Figure 4.
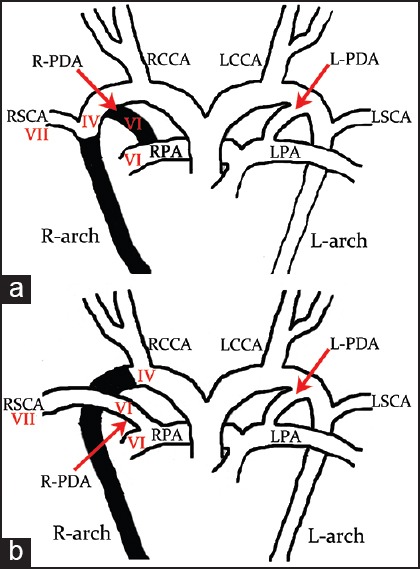
(a) Diagram of the normal embryological origin of the RSCA from the seventh (VII) intersegmental artery with subsequent cranial migration, and dissolution (in black) of the R-PDA and right fourth (IV) aortic arch (R-arch). (b) Isolation of the RSCA occurs when there is dissolution (in black) of the right IV aortic arch but persistence of the right sixth (VI) arch from which the R-PDA and RPA take their origin. L-arch = Left aortic arch, LCCA = left common carotid artery, L-PDA = left ductus arteriosus, LSVC = left subclavian artery, LPA = left pulmonary artery, RCCA = right common carotid artery
In a patient with normally related great arteries and this unusual aortic arch abnormality, when the right ductus arteriosus closes, the isolated RSCA is typically supplied by retrograde flow from the vertebral artery via the circle of Willis, and may lead to subclavian steal syndrome with subsequent neurological deficits and syncope.[11] Hence, at the time of arterial switch operation, our decision was to reimplant the RSCA to the ipsilateral carotid artery rather than simply ligate the right ductus arteriosus.
CONCLUSION
The diagnosis of an isolated RSCA can be made by clinical presentation alone in a patient with d-TGA. Noninvasive imaging modalities such as transthoracic echocardiography and MRI can confirm the origin of the RSCA. Surgical reimplantation of the anomalous RSCA with appropriate excision of residual ductal tissue can be performed at the time of the arterial switch operation to prevent subclavian steal phenomenon.
Video available on www.annalspc.com
Footnotes
Source of Support: NIH 2 R01EB0096090,
Conflict of Interest: None declared.
REFERENCES
- 1.McElhinney DB, Silverman NH, Brook MM, Reddy VM, Hanley FL. Rare forms of isolation of the subclavian artery: Echocardiographic diagnosis and surgical considerations. Cardiol Young. 1998;8:344–51. doi: 10.1017/s1047951100006855. [DOI] [PubMed] [Google Scholar]
- 2.Mosieri J, Chintala K, Delius RE, Walters HL, 3rd, Hakimi M. Abnormal origin of the right subclavian artery from the right pulmonary artery in a patient with D-transposition of the great vessels and left juxtaposition of the right atrial appendage: An unusual anatomical variant. J Card Surg. 2004;19:41–4. doi: 10.1111/j.0886-0440.2004.04008.x. [DOI] [PubMed] [Google Scholar]
- 3.Hofbeck M, Rupprecht T, Reif R, Singer H. Faulty origin of the right subclavian artery from the pulmonary artery: A rare cause of subclavian steal syndrome in childhood. Monatsschr Kinderheilkd. 1991;139:363–5. [PubMed] [Google Scholar]
- 4.Paquet M, Williams RL. Origin of the right subclavian artery from the right pulmonary artery in a newborn with complete transposition of the great arteries. Can J Cardiol. 1994;10:932–4. [PubMed] [Google Scholar]
- 5.Marin C, Sanchez ML, Fernandez-Velilla M, Ruiz Y, Maroto E, Delgado J. MR imaging of isolated right subclavian artery. Pediatr Radiol. 2008;38:216–9. doi: 10.1007/s00247-007-0629-4. [DOI] [PubMed] [Google Scholar]
- 6.Edwards JE. Anomalies of the derivatives of the aortic arch system. Med Clin North Am. 1948;32:925–49. doi: 10.1016/s0025-7125(16)35662-0. [DOI] [PubMed] [Google Scholar]
- 7.Hernandez LE, Shepard CW, Bamforth SD, Anderson RH. The right subclavian artery arising as the first branch of a left-sided aortic arch. World J Pediatr Congenit Heart Surg. 2014;5:456–9. doi: 10.1177/2150135113519457. [DOI] [PubMed] [Google Scholar]
- 8.Anderson RH, Chaudhry B, Mohun TJ, Bamforth SD, Hoyland D, Phillips HM, et al. Normal and abnormal development of the intrapericardial arterial trunks in humans and mice. Cardiovasc Res. 2012;95:108–15. doi: 10.1093/cvr/cvs147. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Gupta SK, Bamforth SD, Anderson RH. How frequent is the fifth arch artery? Cardiol Young. 2014;29:1–19. doi: 10.1017/S1047951114002182. [DOI] [PubMed] [Google Scholar]
- 10.Gowda SLG, Bhat PS, Jayaranganath M, Hedge M. Isolated left brachiocephalic trunk arising from the main pulmonary artery with right aortic arch. J Thorac Cardiovasc Surg. 2014;147:822–3. doi: 10.1016/j.jtcvs.2013.07.015. [DOI] [PubMed] [Google Scholar]
- 11.Miller SG, Campbell MJ, Barker PC, Hill KD. Isolated right subclavian artery arising from the right pulmonary artery via a right-sided ductus arteriosus with associated pulmonary steal phenomenon. Cardiol Young. 2012;22:216–8. doi: 10.1017/S1047951111001065. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.