

Abstract
Background
The developing world accounts for 99% of global maternal deaths. Men in developing countries are the chief decision-makers, determining women's access to maternal health services and influencing their health outcomes. At present, it is unclear whether involving men in maternal health can improve maternal outcomes. This systematic review and meta-analysis aimed to investigate the impact of male involvement on maternal health outcomes of women in developing countries.
Methods
Four electronic databases and grey literature sources were searched (up to May 2013), together with reference lists of included studies. Two reviewers independently screened and assessed the quality of studies based on prespecified criteria. Measures of effects were pooled and random effect meta-analysis was conducted, where possible.
Results
Fourteen studies met the inclusion criteria. Male involvement was significantly associated with reduced odds of postpartum depression (OR=0.36, 95% CI 0.19 to 0.68 for male involvement during pregnancy; OR=0.34, 95% CI 0.19 to 0.62 for male involvement post partum), and also with improved utilisation of maternal health services (skilled birth attendance and postnatal care). Male involvement during pregnancy and at post partum appeared to have greater benefits than male involvement during delivery.
Conclusions
Male involvement is associated with improved maternal health outcomes in developing countries. Contrary to reports from developed countries, there was little evidence of positive impacts of husbands’ presence in delivery rooms. However, more rigorous studies are needed to improve this area's evidence base.
Keywords: MATERNAL HEALTH, DEVELOPING COUNTR, SYSTEMATIC REVIEWS, INTERNATIONAL HLTH, ACCESS TO HLTH CARE
Introduction
Developing countries account for 99% of global maternal deaths.1 In Sub-Saharan Africa, for example, a woman's lifetime risk of dying from preventable or treatable complications of pregnancy and childbirth is 1 in 39, compared to 1 in 3800 in the developed regions.2 The 1994 International Conference on Population and Development advocated for the active inclusion and shared responsibility of men in reproductive health.3 Male involvement, an all-encompassing term which refers to “the various ways in which men relate to reproductive health problems and programmes, reproductive rights and reproductive behaviour”, is considered an important intervention for improving maternal health.4 In many developing countries, men are the key decision-makers and chief providers, often determining women's access to economic resources. This practice has implications for maternal health as it determines the nutritional status of women during pregnancy;5 women's access to maternal health services since healthcare systems in most developing countries require out-of-pocket payments;6–9 and women's chances of receiving emergency obstetrics care, which is vital in averting maternal mortality.5
Many studies have reported positive benefits of male involvement in maternal health in developed and developing countries, which include: increased maternal access to antenatal and postnatal services;10 11 discouragement of unhealthy maternal practices such as smoking;12 13 improved maternal mental health;14–23 increased likelihood of contraception usage;24 25 and allayment of stress, pain and anxiety during delivery.26–29 However, arguments on the downsides of male involvement have also been highlighted such as increased male dominance in decision-making30 31 and the potential for escalating labour difficulty when husbands become anxious in delivery rooms.10
Evidence suggests that male involvement may be beneficial to maternal health; however, the magnitude of the association is not clear. There have also been speculations on possible negative impacts if men were involved in maternal health, hence it is necessary to undertake a systematic review to reconcile these opposing views. However, it is paramount that the review focuses on developing countries since they bear the greatest burden of global maternal deaths and men's dominant roles in these regions have been shown to influence health outcomes. Previous systematic reviews have focused on developed regions,16 on the impact of male involvement on non-maternal health areas such as child health outcomes,32 33 or on its impact on HIV/AIDS topics in developing countries.34–36 Thus, this systematic review aimed to assess the impact of male involvement on maternal health outcomes of women in developing countries. The review was restricted to maternal outcomes in order to have a much more focused research question. In addition, improved maternal health is one of the Millennium Development Goals in which “progress…is falling short”, thus necessitating research on alternative interventions.37
Methods
Criteria for selecting studies
We included all comparative observational studies or controlled trials assessing the impact of male involvement on maternal health outcomes in women of childbearing age (15–49 years) from developing countries (as defined by the World Bank).38
The term ‘male involvement’ is subjective and very multifaceted.34 The most basic criterion used for identifying male involvement in this review was men being in marital unions with the women (legal, religious or traditional). However, being in a marital relationship does not necessarily translate into male involvement. Hence three broad categories were considered as indicating male involvement:
Active participation in maternal health services and care (husband's attendance of antenatal care (ANC); husband's presence at delivery room; and husband's support/help to wife during pregnancy, delivery or at post partum);
Financial support given for pregnancy-related and childbirth-related expenses;
Shared decision-making powers on maternal health with wife.
We excluded studies which focused on male involvement within out-of-wedlock adolescent pregnancies; studies on the impact of male involvement on women's uptake of prevention of mother-to-child transmission and HIV Counselling and Testing services, since systematic reviews have already been conducted on these areas34–36; non-journal articles (commentaries, editorials, letters, reviews and policy statements) and qualitative studies.
Types of outcome measures
Primary outcomes:
Complications (during pregnancy and during childbirth)
Duration of postpartum stay at hospital
Maternal depression (antenatal depression and postpartum depression)
Secondary outcomes:
Maternal health service utilisation ( ANC, skilled birth attendance (SBA), postnatal care and emergency obstetrics care)
Maternal mortality
Data sources
MEDLINE, EMBASE, CENTRAL, CINAHL and grey literature sources (http://www.theses.com and the Electronic Theses Online Service http://www.ethos.ac.uk) were searched from inception to May 2013. The references of included studies were also tracked for additional papers. Searches were conducted using both free texts and medical subject headings based on the exposure/intervention and outcomes (see online supplementary appendix 1).
Study selection
The authors independently screened the titles and abstracts of retrieved studies, and the full texts of potentially eligible studies. Discrepancies on decisions between the two reviewers were resolved via discussion at respective screening stages. Language restrictions were not imposed and three non-English papers were translated. Data extraction was conducted by both authors independently using a previously piloted data extraction form, with disagreements resolved via discussion. The methodological quality of studies was assessed independently by the two authors and disagreements were also resolved via consensus. The Cochrane Collaboration's Risk of Bias tool was used to assess the quality of randomised controlled trials (RCTs) and quasi-experimental studies.39 Studies were categorised as having low, unclear or high risk of bias depending on how they met the criteria stipulated in the six domains of the Risk of Bias tool. For example, for studies to be termed high quality, they had to meet rigorous RCT standards such as demonstrating evidence of randomisation, allocation concealment and blinding. For observational studies, quality was assessed using the Newcastle-Ottawa Scale (NOS).40 A NOS score of <4 was deemed low quality, 4–5 as moderate quality and ≥6 as high quality. The Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) Statement was adhered to in the review.41
Data synthesis and analysis
Crude or adjusted ORs with 95% CI were extracted from the included studies. Adjusted measures of effects were used in preference where both were reported. p Values less than 0.05 were deemed statistically significant. Using Cochrane Review Manager V.5.2 software (RevMan),42 meta-analysis was conducted using a random effect model43 to pool measures of effects where studies were available and “sufficiently homogenous in terms of participants, interventions and outcomes to provide a meaningful summary”.44
Heterogeneity was quantified using I2,45 which measures the degree of inconsistency between the studies. A value of 0% indicated no observed heterogeneity between the studies, with larger values indicating increased levels of heterogeneity. We anticipated that there would be moderate to substantial levels of heterogeneity in the meta-analyses due to clinical and methodological differences between the studies. Where we observed extreme levels of heterogeneity (I2 values between 85% and 100%), we identified which studies appeared to be contributing to the inconsistency.
A number of subgroup analyses were specified a priori in the review protocol to explore reasons for heterogeneity between studies, where sufficient numbers of studies were included in the meta-analyses. A subgroup analysis, based on timing of male involvement (at pregnancy, delivery, post partum) was performed to determine whether there were any descriptive differences on maternal health outcomes. Publication bias was assessed using funnel-plot where sufficient numbers of studies were available.
Results
Overview of search hits and included studies
The electronic databases yielded a total of 11 702 hits. After removing duplicates and screening papers based on their titles and abstracts, 60 papers were screened at the full text stage. Fourteen papers were finally included in the review (figure 1). The reference lists of the included papers were checked, but no additional papers were identified. Similarly, the grey literature searches did not yield additional papers for inclusion. The reasons for excluding papers at the full text stage are listed in online supplementary appendix 2. Four full-text papers could not be obtained even after contacting authors; the impact of this on findings cannot be ascertained.
Figure 1.

Flowchart of search results from data sources.
Of the 14 studies included (table 1), 7 were conducted in South Asia,46–52 3 in East Asia and Pacific,53–55 2 in Europe and Central Asia,56 57 1 in Sub-Saharan Africa58 and 1 in the Middle-East and North Africa.59 Seven studies used a cross-sectional design,46 52 54 56–59 three a cohort design,47 48 55 two a quasi-experimental design,50 53 one an RCT design49 and one a case–control design.51 With respect to maternal health outcomes, 4 of the 14 studies focused on complications (all on complications during childbirth; 2 studies considered a broad list of complications, including some that occurred during pregnancy; however, a significant majority of the complications occurred during childbirth, hence were classified as ‘complications during childbirth’),50 52 53 58 8 on maternal depression (3 focused on antenatal depression and 5 on postpartum depression)47 48 51 54–57 59 and 2 on maternal health service utilisation (1 on ANC, 2 on SBA and 1 on postnatal care; 1 study reported the impact of male involvement on more than one maternal health service, hence the numbers do not add up to 2).46 49 In considering male involvement, 13 studies focused on the first category “active participation in maternal health services and care”;46–57 59 0 studies on “financial support given for pregnancy-related and childbirth-related expenses” and 1 study focused on the third category “shared decision-making on maternal health with wife”.58 Of the 13 studies that considered the first category of male involvement, 9 focused on the impact of a husband's support/help to his wife in the maternal phase,47 48 51 52 54–57 59 2 considered the impact of a husband's attendance of ANC,46 49 and the last 2 studies focused on the effects of a husband's presence in the delivery room.50 53
Table 1.
Summary descriptions of included studies
| General paper information | Exposure and outcome information | Quality assessment | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Paper and reference number | Study design | Country and World Bank subregion | Participants and final sample size | Study period | Exposure: type of male involvement | Timing of male involvement | Relevant maternal health outcome(s) | Method(s) used to measure/collect outcome(s) | Quality assessment results/score |
| Andersson et al58 | Cross-sectional | Nigeria—Sub-Saharan Africa | 15 629 (7870 in Bauchi; 7759 in C/River) women who had been pregnant in the past 3 years | May–Nov 2009 | Shared decision-making powers with wife | Pregnancy | Complications (during childbirth) | Self-reports (structured questionnaires via face-to-face interviews and focus group discussions) | Moderate quality (NOS 5/7) |
| Aydin et al56 | Cross-sectional | Turkey—Europe and Central Asia | 728 women within first postnatal year | Jan–Feb 2003 | Active participation in maternal healthcare/services—husband's support/help to wife | Post partum | Maternal depression (postpartum depression) | EPDS; ≥13 EPDS scores indicated depression | High quality (NOS 7/7) |
| Chattopadhyay46 | Cross-sectional | India—South Asia | Men and women aged 15–49 (9155, 2335 and 6216 in 3 different areas) | 2005–2006 | Active participation in maternal health services/care—husband's ANC attendance with wife | Pregnancy | Maternal health service utilisation (SBA) | National Family Health Survey III, the equivalent of DHS survey in India | Moderate quality (NOS 5/7) |
| Gausia et al47 | Cohort | Bangladesh—South Asia | 361 women aged 15–49 in rural Matlab subdistrict | July–Dec 2005 | Active participation in maternal healthcare/services—husband's support/help to wife | Pregnancy | Maternal depression (antenatal depression) | EPDS; cut-off score of ≥10 indicated depression | High quality (NOS 9/9) |
| Gausia et al48 | Cohort | Bangladesh—South Asia | 361 women aged 15–49 in rural Matlab subdistrict (346 finally reassessed postdelivery) | July–Dec 2005 | Active participation in maternal healthcare/services—husband's support/help to wife | Post partum | Maternal depression (postpartum depression) | EPDS; cut-off score of ≥10 indicated depression | High quality (NOS 9/9) |
| Ip53 | Quasi-experimental | China (Hong Kong)—East Asia and Pacific | 63 women in maternity unit of a public hospital | A 6-month period (not specified) | Active participation in maternal health services/care—husband's presence in delivery room | Delivery | Complications (during childbirth) | Extracted from medical records | Low quality |
| Lteif et al59 | Cross-sectional | Lebanon—Middle East and North Africa | 79 women consulting a gynaecological outpatient department | July–Aug 2002 | Active participation in maternal health services/care—husband's support/help to wife | Pregnancy | Maternal depression (antenatal depression) | Beck Depression Inventory (<10 no depression, 10–18 moderate, >18 severe) & questionnaire | Low quality (NOS 2/7) |
| Mullany et al49 | RCT | Nepal—South Asia | 442 women attending ANC during second trimester (but only 386 evaluated for some outcomes) | Aug 2003–Jan 2004 | Active participation in maternal health services/care—husband's attendance of ANC with wife | Pregnancy | Maternal health service utilisation (ANC, SBA and postnatal care) | RCT data records | High quality |
| Sapkota et al50 | Quasi-experimental | Nepal—South Asia | 309 women in a central level referral hospital | Feb–Apr 2011 | Active participation in maternal health services/care—Husband's presence in delivery room | Delivery | Complications (during childbirth) | Extracted from medical records | Low quality |
| Senturk et al57 | Cross-sectional | Turkey—Europe and Central Asia | 751 women attending ANC in third trimester from urban and rural settings, Ankara (but 730 analysed finally) | Dec 2007–Aug 2008 | Active participation in maternal healthcare/services—husband's offer of emotional and practical support to wife | Pregnancy | Maternal depression (antenatal depression) | EPDS; ≥13 EPDS scores indicated depression | High quality (NOS 7/7) |
| Sreelekshmi et al51 | Case–control | India—South Asia | 50 cases and 150 controls in a hospital | Aug–Nov 2009 | Active participation in maternal healthcare/services—husband's support/help to wife | Post partum | Maternal depression (postpartum depression) | EPDS; ≥10 EPDS score or a positive answer to question 10 indicated depression | Low quality (NOS 3/9) |
| Wan et al54 | Cross-sectional | China—East Asia and Pacific | 342 women coming for their 6–8 week postpartum follow-up in an obstetric outpatient clinic | May–July 2006 | Active participation in maternal healthcare or services—husband's support/help to wife | Pregnancy and at post partum | Maternal depression (postpartum depression) | EPDS; ≥13 EPDS scores indicated depression | Moderate quality (NOS 5/7) |
| Wasti et al52 | Cross-sectional | Nepal—South Asia | 144 women aged 15–49 who had given birth in the past 5 years | Feb–March 2010 | Active participation in maternal healthcare/services—husband's support/help to wife | Pregnancy | Complications (during childbirth) | Semistructured questionnaire, which was used to construct a maternal health problem index | Low quality (NOS 3/7) |
| Xie et al55 | Cohort | China—East Asia and Pacific | 634 women recruited from hospitals at prenatal phase (534 finally evaluated by end of post partum) | Feb–Sept 2007 | Active participation in maternal healthcare/services—husband's support/help to wife | Pregnancy and at post partum | Maternal depression (postpartum depression) | EPDS; ≥13 EPDS scores indicated depression | High quality (NOS 6/9) |
ANC, antenatal care; EPDS, Edinburgh Postnatal Depression Scale; NOS, Newcastle-Ottawa Scale; RCT, randomised controlled trial; SBA, skilled birth attendance.
Using the quality assessment tools described in the methods section, six studies were considered high quality,47–49 55–57 three moderate46 54 58 and five were low quality.50–53 59 Nine studies adjusted for a measure of socioeconomic status, using education and/or income.46–49 54–58
Findings from studies by outcome
Primary outcome I—complications: Four studies reported the impact of male involvement on complications during childbirth.50 52 53 58 Of these four, only three studies provided relevant information that could be included in the meta-analysis.50 53 58 Two meta-analyses were conducted for this outcome.
Male involvement was not significantly associated with the risk of childbirth complications (OR=0.58, 95% CI 0.28 to 1.21; two studies; figure 2). High levels of heterogeneity were detected between the studies (I2=87%), which appeared to be related to differences in composition of the diverse sample populations (women in the Andersson et al58 study were more deprived with respect to education and institutional delivery compared with women in the other studies; thus the women in the former group may have perceived these complications as ‘normal’ and under-reported them).
Figure 2.
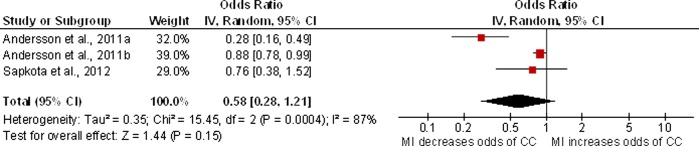
Forest-plot for the impact of MI on complications during childbirth. The Andersson et al58 study was split into two groups because the paper reported separate statistics for the two Nigerian sample states (MI, male involvement; CC, childbirth complications).
Having husbands present in the delivery room was not significantly related to the risk of non-spontaneous deliveries (OR 0.85, 95% CI 0.45 to 1.58; two studies; I2=0%; figure 3).
Figure 3.

Forest-plot for the impact of a husband's presence in the delivery room during NSD (MI, male involvement; NSD, non-spontaneous delivery).
The remaining study52 could not be included in the meta-analyses because it reported results from linear regression, as opposed to using the measures of effects considered in the meta-analyses we conducted (binary outcome). It found a significant decrease in the number of childbirth complications with increasing male involvement (p=0.0181).
Primary outcome II—duration of postpartum stay at hospital: None of the included studies reported this outcome.
Primary outcome III—maternal depression: Three studies assessed the impact of male involvement on antenatal depression.47 57 59 Findings from two studies found out that male involvement significantly decreased the likelihood of antenatal depression by approximately 90% (OR=0.12, 95% CI 0.02 to 0.60;47 59 OR=0.10, 95% CI not reported; p=0.001).59 In the remaining study,57 women with antenatal depression had significantly lower emotional and practical support from their husbands than women without antenatal depression (p<0.05; OR and corresponding CIs not available).
Five of the included studies assessed the impact of male involvement on postpartum depression.48 51 54–56 During pregnancy, male involvement significantly decreased the likelihood of postpartum depression by 64% (OR=0.36, 95% CI 0.19 to 0.68; I2=49%; two studies; figure 4). Also, during the postpartum period, male involvement significantly decreased the likelihood of postpartum depression by 66%, (OR 0.34, 95% CI 0.19 to 0.62; I2=57%; five studies; figure 4).
Figure 4.

Forest-plot for the impact of male involvement (MI) on postpartum depression (PPD). The Wan et al54 and Xie et al55 studies were split into two because they provided statistics on PPD for two phases—MI during pregnancy and MI postpartum.
Secondary outcome I—maternal health service utilisation: Two of the included studies reported the impact of male involvement on use of maternal health services.46 49 One study found husbands’ attendance of antenatal appointments was not significantly associated with women's ANC attendance (OR=0.97, 95% CI 0.88 to 1.07).49 One of the included studies found that husbands’ attendance at ANC was significantly associated with having a skilled attendant at birth (OR=1.35, 95% CI not reported; p=0.01)46 while the other study found a ‘borderline’ non-significant association (OR=1.09, 95% CI 0.99 to 1.2).49 In addition, women whose husbands attended ANC were significantly more likely to receive postnatal care than women who either received health education alone (OR=1.25, 95% CI 1.01 to 1.54) or no education (OR=1.29, 95% CI 1.04 to 1.60). None of the studies reported on the emergency obstetrics care outcome.
Secondary outcome II—maternal mortality: None of the included studies reported this outcome.
Relationship between the type of male involvement and its corresponding effect on maternal health outcomes
Most studies in this review defined male involvement as the active participation of men in maternal health services/care. Within this category, studies on husbands’ offer of support/care tended to report positive effects on decreased likelihood of maternal depression57 59 (figure 4) and childbirth complications;52 whereas studies focusing on the husband's attendance at ANC appeared to have more impact on women's utilisation of maternal health services, relating to SBA and postnatal care.46 49 The remaining studies, which defined male involvement as shared decision-making on maternal health with wife, did not appear to have any significant effect on maternal health outcomes. None of the included studies defined male involvement as providing financial support given for pregnancy-related and childbirth-related expenses.
Comparison of effects of male involvement by timing of involvement
Studies which assessed the effect of male involvement during pregnancy and at post partum were more likely to report statistically significant beneficial maternal health effects than those which assessed the impact of male involvement during delivery. In particular, results from studies on husband's attendance at ANC visits or his offer of support/care during pregnancy or at post partum showed similar statistically significant beneficial effects on maternal depression 57 59(figure 4) and maternal health service utilisation;46 49 however, studies assessing the impact of a husband's presence in the delivery room found no significant effect on non-spontaneous delivery.50 53
Assessment of publication bias
A funnel plot of the meta-analysis assessing the association between male involvement and postpartum depression found no evidence of publication bias (online supplementary appendix 3).
Discussion
Main findings
This is the first systematic review and meta-analysis to consider the impact of male involvement on maternal health outcomes in developing countries. This review has demonstrated statistically significant beneficial impacts of male involvement on maternal health through reduced odds of maternal depression and improved utilisation of maternal health services (relating to SBA and postnatal care). Male involvement was also associated with decreased likelihood of childbirth complications, although results showed contradictory significance (the meta-analysis result did not show significant findings while the study excluded from the meta-analysis did). There was little evidence of beneficial maternal health outcomes from husbands’ presence in the delivery room. Furthermore, the synthesis of evidence suggests that male involvement during pregnancy and at post partum appear to offer statistically significant maternal health benefits than male involvement during delivery.
Interpretation
The observed protective effect conferred by husbands’ support/care on odds of maternal depression is consistent with evidence from developed countries.15–23 60 61 A husband's practical support in terms of assisting with child-care and household chores, and his emotional support expressed via boosting his wife's self-esteem in her ability to care for the baby could help explain this protective effect against maternal depression.61 In developing countries where practices adverse to maternal mental health—such as gender inequality and domestic violence—are common, the impact of a husband's support/care can go a long way in boosting maternal mental health. These results should be interpreted with some caution however. Approximately half of the maternal depression studies utilised a cross-sectional design, thus reverse causation may be a possible alternative explanation. For example, is lack of husband support a risk factor for postpartum depression, or are women with postpartum depression more likely to isolate themselves from their husbands hence decreasing their chances of obtaining support from them?55
This review has also demonstrated statistically significant beneficial impacts of male involvement on maternal health through improved utilisation of maternal health services (relating to SBA and postnatal care). Previous studies elsewhere have linked husbands’ attendance of ANC with increased maternal health service utilisation.10 62 A possible explanation for this association is that men's knowledge about the importance of maternal health services increases with active participation, which in turn makes them more likely to encourage and support their wives to use them.63–65 In a developing country setting, this acquired knowledge could also translate into the husbands’ grant of permission and provision of resources for accessing maternal services such as transportation to hospital for delivery, payment of user fees and so on.
Furthermore, male involvement was associated with decreased likelihood of childbirth complications, although results showed contradictory significance. It has been reported in literature that men's offer of practical support can reduce women's workload during pregnancy and ensure they rest sufficiently, therefore one could hypothesise that this offer of practical support could translate through pregnancy to childbirth, where the risk of complications may be minimised. In addition, male involvement fosters adequate complication readiness and birth preparation in the form of recognising danger signs and making arrangement for SBA among other things.66 This in turn prevents delays in accessing care, decreases risk of developing complications and also averts maternal mortality.65 In the Indonesian Suami SIAGA (‘alert husband’) campaign, men exposed to the programme were 1.7 times more likely than unexposed men to take alert actions against birth complications (p<0.001),67 thereby reducing women's likelihood of experiencing them.
There was little evidence of the impact of a husband's presence in the delivery room on beneficial maternal health outcomes. This finding deviates from evidence/reports from developed countries where findings suggest significant maternal effects when husbands are present in the delivery room.26–29 This deviation could be due to a lack of power to detect a clinically significant effect since only two studies50 53 constituted the meta-analysis, or due to the poor quality of the two quasi-experimental studies included in the meta-analysis, where inadequate or no randomisation was performed.
Finally, the findings from this review suggest male involvement during pregnancy and the postpartum period appear to offer statistically significant maternal health benefits than male involvement during delivery. The explanation for this association is not clear in literature. It is plausible that the dearth of studies or lack of power in the studies on male involvement during delivery could be likely reasons. Duration of exposure could also be a possible explanation. The pregnancy and postpartum phases are longer time periods compared with the delivery phase, thus the male involvement exposure would have occurred long enough for perceived maternal benefits to be observed unlike the delivery phase. In addition, the pregnancy and postpartum phases are less characterised with highly intense maternal anxiety and pain compared to the delivery phase, therefore more benefits could potentially be easily seen in the former two.
Strengths and limitations
Overall, the studies included in this review provided valuable insights on the research topic. Almost half of the studies were assessed as high quality, with some studies using robust RCT and cohort designs. In general, majority of studies adjusted for confounding and also had good response rates, with several exceeding 90%. The literature search for evidence was comprehensive and filters were not used for study design or countries in order to increase sensitivity of the search. In addition, restrictions were not placed in terms of time and language and non-English papers were translated. Authors were also contacted for inaccessible papers and missing details in studies. Widely known tools were also used to assess some outcomes; for example, the Edinburgh Postnatal Depression Scale (EPDS) was used to screen for postpartum depression. The EPDS appears to be culturally relevant as included studies used translated (and sometimes validated) versions of this tool, with sensitivity and specificity percentages in the 70s and 80s.
However, this review has certain limitations. The review found a general dearth of evidence on male involvement in the developing world. A significant weakness was the paucity of studies in specific regions of the globe such as Latin America and the Caribbeans and Sub-Saharan Africa. Ten of the 14 included studies were conducted in Asia, raising questions on the generalisability of findings to other developing regions. The majority of the research also focused on maternal depression, which is a less pressing issue for developing countries due to high rates of maternal mortality and low rates of mental health service utilisation. Thus the evidence base needs to be improved in terms of regional representation, study robustness, and consideration of more pressing outcomes such as maternal mortality.
In addition, some studies appeared to be insufficiently powered, which may have contributed to the non-significant findings observed for few of the outcomes. The data on the definition and timing of male involvement were generally obtained via self-reports, potentially introducing reporting bias. Although the meta-analysis for male involvement on complications during childbirth was non-significant, one additional study52 which could not be included in the meta-analysis due to how the data were reported, did find a significant improvement in outcome; therefore, we are not currently able to conclude the effect of male involvement on this outcome.
Furthermore, due to the nature of the countries considered in this review and their unique economic constraints, some studies may not have been published. It is plausible that such studies may have been published in regional databases that are largely absent in the international scene. On one hand, however, certain regional databases with ample representation at the international level (such as LILACS) were not searched, thus some papers could potentially have been missed. On the other hand, one paper that explored the effectiveness of numerous databases in identifying studies for systematic reviews on a WHO case study topic found that MEDLINE alone identified 75% of electronic citations and 62% of all included citations, the highest yield.68 Thus the probability of missing relevant papers in this review appears to be very negligible.
Conclusions
There is some evidence that male involvement improves maternal health in developing countries. It is therefore paramount to consider men as part of ‘the solution’ rather than ‘the problem’.8 The results underscore the need to shift from women-only maternal health services to ‘male-friendly’, couple-services, and also to dissolve healthcare/government policies that inadvertently isolate/discourage men from active engagement in maternal health programmes. Effective awareness campaigns promoting male involvement should be organised so that men can be aware of their roles and specific ways to get involved in maternal health.
This review could not conclusively reconcile the contradictory perspectives with respect to the impact of husbands’ presence in the delivery room on maternal health. Further studies should be conducted to reconcile the differences so that male involvement efforts are not counterproductive. Finally, the evidence base on male involvement in maternal health in developing countries needs to be improved in terms of quality as well as quantity.
Key messages.
Male involvement significantly reduced the odds of postpartum depression in women and improved overall utilisation of maternal health services.
Male involvement during pregnancy and postpartum may offer greater maternal benefits than male involvement during delivery.
There is a general dearth of evidence on male involvement in assessing its effect on specific maternal health outcomes in the developing world; further high quality studies need to be performed.
Supplementary Material
Acknowledgments
The research was internally supported by the University of Nottingham, UK.
Footnotes
Contributors: This paper originated from a master's dissertation submitted to the Division of Epidemiology and Public Health, University of Nottingham, UK. JY was the master's student while JL-Bee was the supervisor. Thus both authors contributed significantly at every stage of the paper, including protocol design, screening, data extraction, quality assessment, meta-analysis and other relevant sections. The two authors independently carried out the screening, data extraction and quality assessment components of the review and settled discrepancies/disagreements via consensus.
Funding: The research was internally supported by the University of Nottingham.
Competing interests: None.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.World Health Organisation. Maternal mortality. http://www.who.int/mediacentre/factsheets/fs348/en/index.html (accessed 5 Feb 2013).
- 2.World Health Organisation. MDG 5: Improve maternal health. http://www.who.int/topics/millennium_development_goals/maternal_health/en/index.html (accessed 18 Mar 2013).
- 3.United Nations Department of Public Information. International Conference on Population and Development, ICPD ‘94: Summary of the programme of action 1995. http://www.un.org/ecosocdev/geninfo/populatin/icpd.htm (accessed 5 Feb 2013).
- 4.United Nations Population Fund. Male involvement in reproductive health, including family planning and sexual health 1995. http://snap3.uas.mx/RECURSO1/unfpa/data/docs/unpf0074.pdf (accessed 6 Feb 2013). [Google Scholar]
- 5.Dudgeon MR, Inhorn MC. Men's influences on women's reproductive health: medical anthropological perspectives. Soc Sci Med 2004;59:1379–95. [DOI] [PubMed] [Google Scholar]
- 6.Gharoro EP, Igbafe AA. Antenatal care: some characteristics of the booking visit in a major teaching hospital in the developing world. Med Sci Monit 2000;6:519–22. [PubMed] [Google Scholar]
- 7.Bhalerao V, Galwankar M, Kowli S, et al. Contribution of the education of the prospective fathers to the success of maternal health care programme. J Postgraudate Med 1984;30:10–2. [PubMed] [Google Scholar]
- 8.Beenhakker BC. The impact of male involvement in antenatal care in Kathmandu, Nepal. Proquest Dissertations and Theses: Doctor of Philosophy Dissertation. Johns Hopkins University, 2005. [Google Scholar]
- 9.Banos JP, Banos C, Moumouni Z. Constraints faced by hospitalized maternity patients in Niamey, Niger. Sante 1996;6:345–51. [PubMed] [Google Scholar]
- 10.Redshaw M, Henderson J. Fathers’ engagement in pregnancy and childbirth: evidence from a national survey. BMC Pregnancy Childbirth 2013;13:1–15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Schaffer MA, Lia-Hoagberg B. Effects of social support on prenatal care and health behaviors of low-income women. J Obstet Gynecol Neonatal Nurs 1997;26:433–40. [DOI] [PubMed] [Google Scholar]
- 12.Martin LT, McNamara MJ, Milot AS, et al. The effects of father involvement during pregnancy on receipt of prenatal care and maternal smoking. Matern Child Health J 2007;11:595–602. [DOI] [PubMed] [Google Scholar]
- 13.Kiernan K, Pickett KE. Marital status disparities in maternal smoking during pregnancy, breastfeeding and maternal depression. Soc Sci Med 2006;2:335–46. [DOI] [PubMed] [Google Scholar]
- 14.Bielinski-Blattmann D, Lemola S, Jaussi C, et al. Postpartum depressive symptoms in the first 17 months after childbirth: the impact of an emotionally supportive partnership. Int J Public Health 2009;54:333–9. [DOI] [PubMed] [Google Scholar]
- 15.O'Hara MW. Social support, life events, and depression during pregnancy and the puerperium. Arch Gen Psychiatry 1986;43:569–73. [DOI] [PubMed] [Google Scholar]
- 16.Plantin L, Olukoya AA, Ny P. Positive health outcomes of fathers’ involvement in pregnancy and childbirth paternal support: a scope study literature review. Fathering 2011;9:87–102. [Google Scholar]
- 17.Dennis CL, Ross L. Women's perceptions of partner support and conflict in the development of postpartum depressive symptoms. J Adv Nurs 2006;56:588–99. [DOI] [PubMed] [Google Scholar]
- 18.Gremigni P, Mariani L, Marracino V, et al. Partner support and postpartum depressive symptoms. J Psychosom Obstet Gynaecol 2011;32:135–40. [DOI] [PubMed] [Google Scholar]
- 19.Grube M. Inpatient treatment of women with postpartum psychiatric disorders—the role of the male partners. Arch Womens Ment Health 2005;8:163–70. [DOI] [PubMed] [Google Scholar]
- 20.Al Dallal FH, Grant IN. Postnatal depression among Bahraini women: prevalence of symptoms and psychosocial risk factors. East Mediterr Health J 2012;18:432–8. [PubMed] [Google Scholar]
- 21.Lee D. Partner support reduced depressive symptoms in postpartum depression. Evid Based Ment Health 2001;4:51. [Google Scholar]
- 22.Reid H, Power M, Cheshire K. Factors influencing antenatal depression, anxiety and stress. Br J Midwifery 2009;17:501–8. [Google Scholar]
- 23.Stapleton LR, Schetter CD, Westling E, et al. Perceived partner support in pregnancy predicts lower maternal and infant distress. J Fam Psychol 2012;26:453–63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Mekonnen W, Worku A. Determinants of low family planning use and high unmet need in Butajira District, South Central Ethiopia. Reprod Health 2011;8:1–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Yue K, O'Donnell C, Sparks PL. The effect of spousal communication on contraceptive use in Central Terai, Nepal. Patient Educ Couns 2010;81:402–8. [DOI] [PubMed] [Google Scholar]
- 26.D'Aliesio L, Vellone E, Amato E, et al. The positive effects of father's attendance to labour and delivery: a quasi experimental study. Int Nurs Perspect 2009;9:5–10. [Google Scholar]
- 27.Block CR, Norr KL, Meyering S, et al. Husband gatekeeping in childbirth. Fam Relations 1981;30:197–204. [Google Scholar]
- 28.Guthrie K, Taylor DJ, Defriend D. Maternal hypnosis induced by husbands during childbirth. J Obstet Gynaecol 1984;5:93–5. [Google Scholar]
- 29.Henneborn WJ, Cogan R. The effect of husband participation on reported pain and probability of medication during labour and birth. J Psychosom Res 1975;19:215–22. [DOI] [PubMed] [Google Scholar]
- 30.Helzner JF. Men's involvement in family planning. Reprod Health Matters 1996;7:146–54. [Google Scholar]
- 31.Char A. Male involvement in family planning and reproductive health in rural central India. Finland: University of Tampere, 2011. [Google Scholar]
- 32.Sarkadi A, Kristiansson R, Oberklaid F, et al. Fathers’ involvement and children's developmental outcomes: a systematic review of longitudinal studies. Acta paediatrica 2008;97:153–8. [DOI] [PubMed] [Google Scholar]
- 33.Alio AP, Salihu HM, Kornosky JL, et al. Feto-infant health and survival: does paternal involvement matter? Matern Child Health J 2010;14:931–7. [DOI] [PubMed] [Google Scholar]
- 34.Morfaw F, Mbuagbaw L, Thabane L, et al. Male involvement in prevention programs of mother to child transmission of HIV: a systematic review to identify barriers and facilitators. Syst Rev 2013;2:5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Brusamento S, Ghanotakis E, Car LT, et al. Male involvement for increasing the effectiveness of prevention of mother-to-child HIV transmission (PMTCT) programmes (review). Cochrane Database Cyst Rev 2012;10:1–18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Ditekemena J, Koole O, Engmann C, et al. Determinants of male involvement in maternal and child health services in sub-Saharan Africa: a review. Reprod Health 2012;9:32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.United Nations. The Millennium Development Goals Report 2013. 2013. http://www.un.org/millenniumgoals/pdf/report-2013/mdg-report-2013-english.pdf (accessed 21 Oct 2013).
- 38.World Bank. Data: Country and lending groups. http://data.worldbank.org/about/country-classifications/country-and-lending-groups 2013. (accessed 4 Feb 2013).
- 39.Higgins JPT, Green S. Assessing risk of bias in included studies. In: Cochrane Handbook for Systematic Reviews of Interventions. Chichester: Wiley-Blackwell, 2008:187–242. [Google Scholar]
- 40.Wells GA, Shea B, O'Connell D, et al. Newcastle-Ottawa Quality Assessment Scale. In: Ottawa Hospital Research Institute, 2013. Our Research: The Newcastle- Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses 2013. http://www.ohri.ca/programs/clinical_epidemiology/nosgen.pdf (accessed 15 Mar 2013).
- 41.Moher D, Liberati A, Tetzlaff J, et al. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA Statement. BMJ 2009;339:332–6. [PMC free article] [PubMed] [Google Scholar]
- 42.Cochrane Information Management System. RevMan 2012. http://ims.cochrane.org/revman (accessed).
- 43.Dersimonian R, Laird N. Meta-analysis in clinical trials. Controlled Clin Trials 1986;7:177–88. [DOI] [PubMed] [Google Scholar]
- 44.Higgins JPT, Green S. Analysing data and undertaking meta-analyses. In: Cochrane Handbook for Systematic Reviews of Interventions. Chichester: Wiley-Blackwell, 2008:243–96. [Google Scholar]
- 45.Higgins JPT, Thompson SG, Deeks JJ, et al. Measuring inconsistency in meta-analyses. BMJ 2003;327:557–60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Chattopadhyay A. Men in maternal care: evidence from India. J Biosoc Sci 2012;44:129–53. [DOI] [PubMed] [Google Scholar]
- 47.Gausia K, Fisher C, Ali M, et al. Antenatal depression and suicidal ideation among rural Bangladeshi women: a community-based study. Arch Womens Ment Health 2009;12:351–8. [DOI] [PubMed] [Google Scholar]
- 48.Gausia K, Fisher C, Ali M, et al. Magnitude and contributory factors of postnatal depression: a community-based cohort study from a rural subdistrict of Bangladesh. Psychol Med 2009;39:999–1007. [DOI] [PubMed] [Google Scholar]
- 49.Mullany BC, Becker S, Hindin MJ. The impact of including husbands in antenatal health education services on maternal health practices in urban Nepal: results from a randomized controlled trial. Health Educ Res 2007;22:166–76. [DOI] [PubMed] [Google Scholar]
- 50.Sapkota S, Kobayashi T, Kakehashi M, et al. In the Nepalese context, can a husband's attendance during childbirth help his wife feel more in control of labour? BMC Pregnancy Childbirth 2012;12:1–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Sreelekshmi F, Sharika S, Vidyakrishna V, et al. Risk factors of postpartum depression among married mothers attending SAT Hospital, Trivandrum. Aust Med J 2010;3:222. [Google Scholar]
- 52.Wasti D, Lim A, Pathak RS. Influence of husband domestic support on maternal morbidity in rural Nepal. Southeast Asian J Trop Med Public Health 2012;43:1009–17. [PubMed] [Google Scholar]
- 53.Ip WY. Chinese husbands’ presence during labour: a preliminary study in Hong Kong. Int J Nurs Pract 2000;6:89–96. [DOI] [PubMed] [Google Scholar]
- 54.Wan EY, Moyer CA, Harlow SD, et al. Postpartum depression and traditional postpartum care in China: role of zuoyuezi. Int J Gynaecol Obstet 2009;104:209–13. [DOI] [PubMed] [Google Scholar]
- 55.Xie RH, Yang J, Liao S, et al. Prenatal family support, postnatal family support and postpartum depression. Aust N Z J Obstet Gynaecol 2010;50:340–5. [DOI] [PubMed] [Google Scholar]
- 56.Aydin N, Inandi T, Karabulut N. Depression and associated factors among women within their first postnatal year in Erzurum province in eastern Turkey. Women Health 2005;41:1–12. [DOI] [PubMed] [Google Scholar]
- 57.Senturk V, Abas M, Berksun O, et al. Social support and antenatal depression in extended and nuclear family environments in Turkey: a cross-sectional survey. BMC Psychiatry 2011;11:48. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Andersson N, Omer K, Caldwell D, et al. Male responsibility and maternal morbidity: a cross-sectional study in two Nigerian states. BMC Health Serv Res 2011;11(Suppl 2):1–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Lteif Y, Kesrouani A, Richa S. Depressive syndromes during pregnancy: prevalence and risk factors. J Gynecol Obstet Biol Reprod (Paris) 2005;34(3 Pt 1):262–9. [DOI] [PubMed] [Google Scholar]
- 60.Sexton MB, Flynn HA, Lancaster C, et al. Predictors of recovery from prenatal depressive symptoms from pregnancy through postpartum. J Womens Health (Larchmt) 2012;21:43–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Stewart DE, Robertson E, Dennis CL, et al. Postpartum depression: literature review of risk factors and interventions. Univ Health Netw Womens Health Program 2003. [Google Scholar]
- 62.Tweheyo R, Konde-Lule J, Tumwesigye NM, et al. Male partner attendance of skilled antenatal care in peri-urban Gulu district, Northern Uganda. BMC Pregnancy Childbirth 2010;10:53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Ahmed A, Hossain SAS, Quaiyum A, et al. Husbands’ knowledge on maternal health care in rural Bangladesh: an untapped resource? Trop Med Int Health 2011;16:291. [Google Scholar]
- 64.Ali M, Rizwan H, Ushijima H. Men and reproductive health in rural Pakistan: the case for increased male participation. Eur J Contracept Reprod Health Care 2004;9:260–6. [DOI] [PubMed] [Google Scholar]
- 65.Kakaire O, Kaye DK, Osinde MO. Male involvement in birth preparedness and complication readiness for emergency obstetric referrals in rural Uganda. Reprod Health 2011;8:12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Bhatta DN. Involvement of males in antenatal care, birth preparedness, exclusive breast feeding and immunizations for children in Kathmandu, Nepal. BMC Pregnancy Childbirth 2013;13:14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Shefner-Rogers CL, Sood S. Involving husbands in safe motherhood: effects of the SUAMI SIAGA campaign in Indonesia. J Health Commun 2004;9:233–58. In: Davis J, Luchters S, Holmes W. Men and maternal and newborn health: Benefits, harms, challenges and potential strategies for engaging men. 2012. [DOI] [PubMed] [Google Scholar]
- 68.Betran AP, Say L, Gulmezoglu AM, et al. Effectiveness of different databases in identifying studies for systematic reviews: Experience from the WHO systematic review of maternal morbidity and mortality. BMC Med Res Methodol 2005;5:1–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.