

Abstract
Background
Many studies have been carried out and many methods have been used for estimating health staff re-quirements in health facilities or system, each have different advantages and disadvantages. Differences in the extent to which utilization matches needs in different conditions intensify the limitations of each approach when used in iso-lation. Is the utilization-based approach efficient in a situation of over servicing? Is it sufficient in a situation of under-utilization? These questions can be similarly asked about the needs-based approach. This study is looking for a flexible approach to estimate the health staff requirements efficiently in these different conditions.
Method
This study was carried out in 2011 in some stages: It was conducted in order to identify the formula used in the different approaches. The basic formulas used in the utilization-based approach and the needs-based approach were identified and then combined using simple mathematical principles to develop a new formula. Finally, the new formula was piloted by assessing family health staff requirements in the health posts in Kashan City, Iran.
Results
Comparison of the two formulas showed that the basic formulas used in the two approaches can be com-bined by including the variable ‘Coverage’. The pilot study confirmed the role of coverage in the suggested combined approach.
Conclusions
The variables in the developed formula allow combining needs-based, target-based and utilization-based approaches. A limitation of this approach is applicability to a given service package.
Keywords: Health staff requirement, Utilization-based approach, Needs-based approach, Combined approach
Introduction
In the health system, with abundant problems and restricted resources, the need to optimize the utilization of the available resources is ever present and requires considering both quality and access to deliver health care efficiently (1-4). Therefore it is necessary to manage human resources in order to ensure that appropriate health staff are available to deliver health care services when and where they are needed(5-6). Some approaches have been developed to define health staff requirements; the difference between them is how to identify the quantum of required services (5, 7-14) but three main approaches are emphasized in the literature; The Needs-based approach estimates the required health workforce based on the anticipated health service needs of a given population after adjustment for age and gender (5, 7-8). This approach assumes all health care needs can and should be met (5, 15). It assumes the demand for health services is equal to needs and is applicable to provide a given service package. In addition, it does not reflect technology develop-pments that affect service delivery; it also ignores efficiency in resources allocation, and requires extensive epidemiologic data (5, 15). The Utilization-based approach; projects the expected health service requirements based on present health service utilization and factoring in demographic changes trend (5, 7-8). This approach assumes that future population will utilize the health services in a way similar to the base year (5, 9), therefore it does not consider variations in the quality of and access to the health services nor it take into account future changes in behavior patterns or in productivity (8, 15). This approach also requires extensive data not always available, in particular regarding service utilization in the private sector(16). The Service target-based approach specifies targets for specific health services provision. Targets are determined by considering current services, current technologies, economic factors, and other planning considerations (5, 10, 13). This approach assumes the same needs in all settings and similar productivity of all providers. Targets are not always determined by transparent criteria and may reflect the interests of the professionals and experts(16).
In order to quantify required services, the relationship between needs, demand and utilization needs clarification. Some researchers assume that demand is larger than needs (7, 17) as in a situation of induced demand for curative services(12) (Situation 1). Others assume that need is larger than demand and they emphasize the fact that the needs-based approach overestimates the health workforce (15). This can be observed in the provision of preventive or curative care in low and middle income countries (Situation 2)(18). In the two situations the utilization is a portion of the demand, due to unmet demand(Fig.1). Then is the same approach to project health staff requirements appropriate in these two situations? Is the utilization-based approach efficient in a situation of over servicing? Is it sufficient in a situation of under-utilization? These questions can be similarly asked about the needs-based approach. Although this point has been considered as one cause of imbalance in the health work force by some researchers (9, 19) it has not been taken into account in most studies that deal with the limitations of the approaches (5, 7, 10, 12).
Fig. 1.
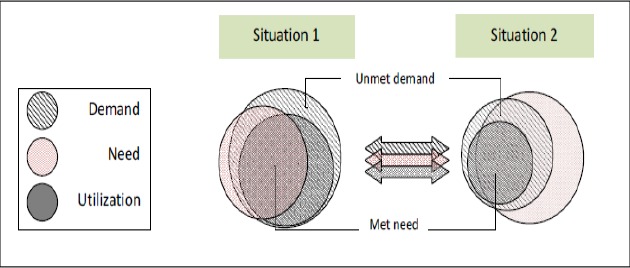
Comparing utilization and need in curative and non-curative services
This study is looking for a flexible approach to estimate the health staff requirements efficiently in these different conditions.
Materials and Methods
This study was conducted in 2011 in two stages. The first, we compared the basic formula applied in the utilization-based approach with the basic formula applied in the needs-based approach. A new formula was then built. The second, we piloted this new formula to assess the family health staff requirements in 13 health posts in Kashan City, Iran.
Comparison of the basic formulas in utilization-based and needs-based approaches
Searching PubMed database and WHO site, we reviewed literature to find papers dealing with the estimation of the health staff requirements in the needs-based or utilization-based approaches in order to identify the basic formulas used. In the formula applied in utilization-based approach the number of required health staff is calculated as ‘the number of the delivered services' (utilization) divided by ‘the number of services that a person is able to provide yearly' (15, 18, 20-23). In the studies in the needs-based approach, the number of the required health staff is assessed from ‘the number of services that should be provided to a given population yearly' divided by the ‘the number of services that a person is able to provide yearly' (11, 24-26).
The number of services that a person is able to provide yearly is calculated as the ‘Standard Workload'(SW) which is ‘Available Working Time' (AWT) per year per health worker divided by ‘Activity Standard' (AS) which is the time per unit of activity as shown in the following equation;
(Equation 1
The staff requirements for yearly service provision is then calculated as, ‘total number of the services delivered in the previous year' or ‘Delivered Services' (DS) divided by Standard Workload as in the following equation;
(Equation 2
If SW in equation2 be replaced with its equal from equation1, the result is;
(Equation 3
Although the formulas in the selected needs-based studies are apparently diverse, they are indeed similar. In all formula, first the target population is calculated by considering population size, age distribution and the given proportion of the population that should receive the health service because of diseases prevalence or other conditions that necessitate the provision of specific service to them (k, need coefficient). The total needed services that should be provided yearly is calculated multiplying ‘the number of target population' by ‘the number of services that should be provided yearly to each person' (frequency) as in the following equation in which ‘Needed Services' (NS) reflects needs.
(Equation 4
The number of Needed Services is then multiplied by the standard time of service provision (AS) to calculate total time that should be spent for yearly service provision as in equation 5;
(Equation 5
In the final step, staff requirement is calculated by dividing ‘Expected Time' by the time that each health worker would spend yearly (AWT) as in the following equation;
(Equation 6)
Finally we developed a new formula combining two formulas considering their ratio mentioned in results.
Applying developed formula to assess the health staff requirements in pilot study.
We applied developed formula to calculate the family health staff requirements in 13 health posts in Kashan City, Iran. In the first step we listed the services provided by family health staff in a health post. In the next step the time needed to provide each type of services per year was calculated by designing a table according the variables in the developed formula in Excel spreadsheet. Then number of required staff was calculated in three scenarios according to the three approaches; utilization-based, needs-based and target-based and compared. The comparison results were presented by ratio of the numbers to show difference between approaches and as a proxy measure to show sufficiency and efficiency.
Results
Some researchers have assessed human resources needed for health in the utilization-based approach (15,18,20-23) via Workload Indicator Staffing Need (WISN) method suggested by World Health Organization (27) and Faulkner(24), Lund and Flisher(25), Birch et al.(11) and Pileroodi(26) have presented formulas for calculating the health staff requirements with a needs-based approach. Certainly, there are other sophisticated models in the needs-based approach but we didn't include them in the study (28-30).
WISN formula as the basic formula in the utilization-based approach has fundamental similarities with the formulas used in the studies in the needs-based approach (Table 1).
Table 1.
Utilization-based and needs-based formulas used in the studies and their calculation steps
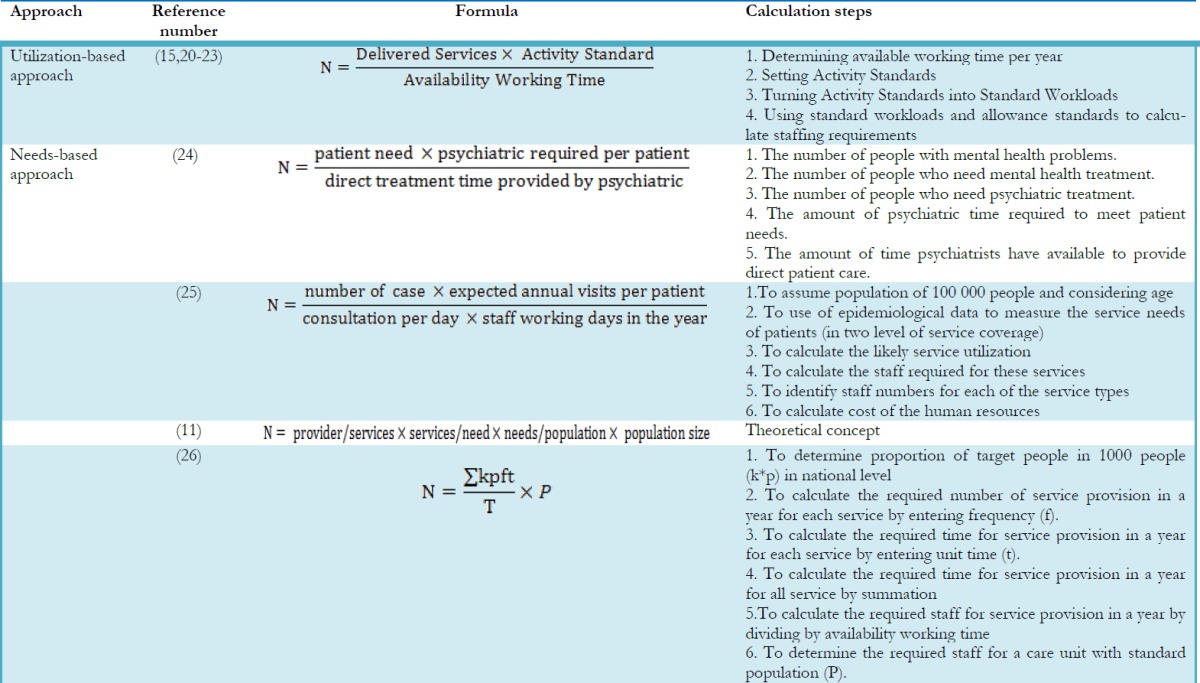
Comparing equation 3 and equation 6 shows that utilization-based and needs-based formulas are similar, although the quantum of services is defined in the utilization-based formula by ‘Delivered Services' and in the needs-based formula by ‘Needed Services'.
Assuming that needed services is the number of services expected to provide to target population and assuming that delivered services are a portion of expected services, the ratio between them can be calculated that is indeed the service coverage. Then two formulas can be combined by adding ‘Coverage' as a modifier variable and maintaining other variables, where coverage represents actual/anticipated coverage in the utilization-based approach and represents full coverage in the needs-based approach. This new formula is named ‘Combined Formula' in this study;
If coverage is equal to service coverage in previous year, the result will be the same as the one calculated ina utilization-based approach and if coverage is 100 percent, the result will be the same as the one used in the needs-based method. It also could be a number between them, as a program target.
Table Table 2 compares the family health staff requirements in Kashan health posts calculated by the use of the combined formula according to three approaches; with a utilization-based approach by considering the service coverage in previous year, with a needs-based one by considering 100 % service coverage and with a target-based approach applying expected coverage issued by the district health center in related programs. These results illustrate the differences between the three approaches in estimation of the needed family health staff in the health posts. The number of staff required according to program targets is 10-20 percent higher than required according to actual coverage in previous year based on annual statistics. Staff requirements for full coverage irrespective of efficiency are 44-57 percent higher than for actual coverage (Table 2).
Table 2.
Comparing the three approaches to calculate health staff requirements by developed formula in the health posts in Kashan City 2011
| No | Health post | Family health worker requirements | Difference rate | |||
| Utilization-based | Needs-based | Target-based | (T-U)/U% | (N-U)/U% | ||
| 1 | Bu-ali | 2.8 | 4.3 | 3.4 | 21 | 54 |
| 2 | Fin | 3.6 | 5.4 | 4.3 | 19 | 50 |
| 3 | Golabchi | 3.5 | 5.4 | 4.2 | 20 | 54 |
| 4 | Karegar | 3.1 | 4.8 | 3.7 | 19 | 55 |
| 5 | Navvab | 3 | 4.7 | 3.6 | 20 | 57 |
| 6 | Sepehri | 2.3 | 3.6 | 2.8 | 22 | 57 |
| 7 | Sultan-mir-ahmad | 2.7 | 4.2 | 3.2 | 19 | 56 |
| 8 | Amir kabir | 5 | 7.2 | 5.5 | 10 | 44 |
| 9 | Sadeghpur | 2.8 | 4.4 | 3.4 | 21 | 57 |
| 10 | Moslem- ebene-Aghil | 2 | 3.1 | 2.4 | 20 | 55 |
| 11 | Fatemiyeh | 1.6 | 2.4 | 1.8 | 13 | 50 |
| 12 | ketabchi | 3.2 | 5 | 3.8 | 19 | 56 |
| 13 | Ravand | 2.8 | 4.2 | 3.3 | 18 | 50 |
Discussion
This study seek a way to avoid disadvantages emerged in different approaches to estimate health facilities or system staffing need. Utilization-based and needs-based approaches are main approaches to estimate staffing need. Differences in the extent to which utilization matches needs in different conditions intensify the limitations of each approach when used in isolation. The comparison of basic formulas applied in the utilization-based and needs-based approaches suggests that two formulas can be combined adding a modifier variable that is indeed services coverage. In the combined formula suggested in this study, services coverage that is the proportion of provided services to expected services is used instead of services quantity. This is an advantage since number of services delivered is usually not reported but the actual service coverage is notified (28). The coverage changes could reflect the targets and therefore the number of services that managers expect to be delivered in a given period. Here, the number of expected services isn't necessarily equal to needs and is determined by considering the conditions that influence the service provision. Anticipated coverage ranges from actual coverage to full coverage (Fig.2). If actual coverage is considered, workload and staff requirements are based on delivered services whilst if full coverage is considered, other factors i.e. demographic and epidemiologic variables determine the results. Full coverage means that all needs should been met(5). In the target-based approach, the number of expected services based on program objectives will typically be somewhere in the continuum. To determine this coverage, considering policies, the goals of upper level program, the current and future conditions, community behaviors, capacities, productivity, and previous operations are important.
Fig. 2.

The coverage continuum
Pilot study results show that the calculated family health workers requirements in the target-based approach are close to the needs-based approach calculation in some health posts whilst close to the utilization-based approach in others. These results illustrates that the calculation of staff requirements in the needs-based approach isn't efficient in a situation of under-utilization. Similarly, assessment of staff requirements in the utilization-based approach isn't efficient in a situation of over servicing. Projecting staff requirements based on a reasonable target provides a more efficient incremental approach in these situations. This means that the approach used in this study assists in scenario planning and increases flexibility and helps move away from the opposition of utilization-based, needs-based or target-based approaches. This approach can help resolve the limitations of the utilization-based or needs-based approaches in situations where utilization is more or less than need (Table 3).
Table 3.
changes in the limitation of utilization-based and needs-based approach in flexible combined approach
| Approach | Limitation | Changes |
|---|---|---|
| Needs-based | Ignores the question of efficiency in allocation of resources among other sectors | Removed |
| Requires extensive data | Remained | |
| If technology changes, it requires norms update | Remained | |
| Is likely to project unattainable service and staff targets | Removed | |
| Utilization-based | Requires extensive data | Remained |
| Overlooks the consequences of ‘errors' arising from the assumptions proving to be invalid | Removed | |
| Produces a ‘status quo' projection, since future population segments are assumed to have similar utilization rates as base year segments |
Source of limitations list: Dreesch, 2005 (5)
Many studies emphasize having a combined approach explicitly or implicitly. Belayet and Syed Ahsanul declare that WISN method is applicable to calculate workforce base on current workload, standards and conditions, but they believe it could be calculated by considering anticipated workload based on the programmed services in future, better standards and changed conditions(20). WISN method has however one limitation in that it equals the number of services that should be provided during the next year to the services provided in the previous year (27). This method however permits modification of the projected level of utilization level based on service provision trend. Daviaud and Chopra calculated the health staff requirements in the rural areas of South Africa with WISN method. Highlighting that this method is relevant for short term human resource management, they believe it may however accentuate the under resourcing of facilities which have a low level of utilization precisely because they are poorly resourced whilst already better resourced facilities would receive increased resources. Therefore they suggest the combination of this approach for short-term management with a population-based approach to assess the expected utilization for long term more equitable resource planning (15).
Some of researchers have adopted the needs-based approach despite applying WISN method as the utilization-based approach. Hagopian et al. calculate the number of required health workers to deliver maternal and child health care by using WISN. They emphasize ‘with WISN, the researcher calculates the staff time it would take to deliver a package of services for a given population'. They obtained the total time required to serve the population by multiplying the required time for each service by the relevant population size(31), actually calculating the staff requirements with a needs-based approach. Claiming to use WISN method, and to assess the number of tutors, Kitanda also has obtained yearly workload by multiplying activity average time by frequency according to school curriculum that shows the needs-based approach rather than the utilization-based approach(32). These studies implicitly put emphasis on the combined approach.
Considering the coverage is seen in some studies. Kurowski et al. mentioned that demography, epidemiology, current service coverage and future service coverage are required information to calculate service quantity(28). Scheffler et al. also applied expected service coverage to forecast the shortage of physicians with a needs-based model(29). Lund and Flisher developed a model to estimate needed human resource for community-based mental health services in South Africa. In this model the expected care per year is identified base on population size, age distribution, prevalence and levels of coverage. Researchers emphasize that weighting the coverage is necessary to allow for various demands and increase in efficiency(25). Other variables in the developed formula i.e. target population, the need coefficient (k), and frequency are equal to demography, epidemiology and level of services in the needs-based analytical framework suggested by Birch et al., respectively as the determinants to estimate the number of health care providers (11).
Conclusion
This paper has focused on the centrality of the coverage level in the quantification of human resource requirements and shown that it is coverage level which is the fundamental difference between the needs-based, target-based and utilization-based approaches; The developed formula gives the opportunity to combine the needs-based, target-based and utilization-based approaches;
Target population with elements of population size, age and gender distribution is main determinant in needs-based approaches.
Need coefficient reflects the influence of prevalence of diseases and other conditions that necessitate health service provision.
Anticipated coverage matches needs-based, target-based and utilization-based approaches.
A limitation of the combined approach is that it is applicable to a given service package. It is also necessary to mention that the level from which the data is used for calculating the coverage influences the applicability of the approach.
Ethical considerations
Ethical issues (Including plagiarism, Informed Consent, misconduct, data fabrication and/or falsification, double publication and/or submission, redundancy, etc.) have been completely observed by the authors.
Acknowledgments
Our thanks go to the authorities and personnel of Kashan Health Center for their support and providing annual statistics. There was no grant or fund for this research. The authors declare that there is no conflict of interests.
References
- World Health Organisation (2000). The World health report 2000: health systems : improving performance. WHO, Switzerland. [Google Scholar]
- Roberts MJ, Hsiao W, Berman P, Reich MR (2002). Getting Health Reform Right. Oxford University Press, New York. [Google Scholar]
- Davari M, Haycox A, Walley T (2005). Health Care Challenges in Iran. Iranian J Publ Health, 34:30–31. [Google Scholar]
- Zanganeh Baygi M, Seyedin H (2013). Imbalance between Goals and Organizational Structure in Primary Health Care in Iran- a Systematic Review. Iranian J Publ Health 42(7):665–672. [PMC free article] [PubMed] [Google Scholar]
- Dreesch N, Dolea C, Dal Poz MR, Goubarev A, Adams O, Aregawi Met al. (2005). An approach to estimating human resource requi-rements to achieve the Millennium Develo-pment Goals. Health Policy and Planning 20(5):267–276. [DOI] [PubMed] [Google Scholar]
- World Health Organisation (2006). The World Health Report 2006: Working together for health. WHO, Switzerland. [Google Scholar]
- O'Brien-Pallas L, Baumann A, Donner G, Murphy GT, Lochhaas-Gerlach J, Luba M (2001). Forecasting models for human reso-urces in health care. Journal of Advanced Nursing, 33(1): 120–129. [DOI] [PubMed] [Google Scholar]
- O'Brien-Pallas L, Baumann A, Birch S, Murphy GT (2001). integrating workforce planning, human resources, and service planning. Human Resources for Health Development Journal (HRDJ), 5(1–3):2–16. [Google Scholar]
- Murphy GT, Birch S, MacKenzie A (2007). Needs-Based Health Human Resources Planning: The Challenge of Linking Needs to Provider Requirements. Canadian Nurses Association and Canadian Medical Association, Canada. [Google Scholar]
- Hall TL (2001). Human resourse for health: Models for projecting workforce supply and requirements. World Health Organization, San Francisco. [Google Scholar]
- Birch S, Kephart G, Murphy GT, O'Brien-Pallas L, Alder R, MacKenzie A (2009). Health Human Resources Planning and the Production of Health: Development of an Extended Analytical Framework for Needs-Based Health Human Resources Planning. Journal of Public Health Management and Practice, 15(6): 56–61 [DOI] [PubMed] [Google Scholar]
- Roberfroid D, Leonard C, Stordeur S (2009). Physician supply forecast: better than peering in a crystal ball? Human Resources for Health, 7(10):1–13 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hirschhorn LR, Oguda L, Fullem A, Dreesch N, Wilson P (2006). Estimating health workforce needs for antiretroviral therapy in resource-limited settings. Human Resources for Health, 4(1):1–16 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Powell J, Griffith S, Kanny E (2005). Occupational Therapy Workforce Needs: A Model for Demand-Based Studies. The American Journal of Occupational Therapy (AJOT), (59): 467–474. [DOI] [PubMed] [Google Scholar]
- Daviaud E, Chopra M (2008). How much is not enough? Human resources requirements for primary health care: a case study from South Africa. Bulletin of the World Health Organization, 86(1):46–51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dussault G, Buchan J, Sermeus W, Padaiga Z (2010). Assessing future health workforce needs, in Investing in Europe's health workforce of tomorrow: scope for innovation and collaboration. World Health Organization, Europe. [Google Scholar]
- Ros K, Drzymala L (2002). Planning Physician Services: Is There a Method to the Madness? Economics and Health Policy, 79(3):257–262. [Google Scholar]
- Simba D, Kamwela J, Mpembeni R, Msamanga G (2010). The impact of scaling-up prevention of mother-to-child transmission (PMTCT) of HIV infection on the human resource require-ment: the need to go beyond numbers. Int J Health Plann Mgmt, 25:17–29. [DOI] [PubMed] [Google Scholar]
- Zurn P, Poz MRD, Stilwell B, Adams O (2004). Imbalance in the health workforce. Human Resources for Health, 2(13). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Belayet H, Ahsanul AS (1999). Likely Benefit of Using Workload Indicators of Staffing Need (WISN) for Human Resources Management and Planning in the Health Sector of Bangladesh. Human Resources for Health Development Journal(HRDJ) 3(2): 99–111. [Google Scholar]
- Musau P, Nyongesa P, Shikhule A, Birech E, Kirui D, Njenga Met al. (2008). Workload Indicators of Staffing Need method in determining optimal staffing levels at moi teaching and referral hospital. East Af Med J, 85. [DOI] [PubMed] [Google Scholar]
- Ozcan S, Hornby P (1999). Determining Hospital Workforce Requirements: A Case Study. Human Resources for Health Development Journal (HRDJ) 3(3): p. 210–220. [Google Scholar]
- Nyamtema A, Urassa D, Massawe S, Massawe A, Lindmark G, Roosmalen JV (2008). Staffing Needs for Quality Perinatal Care in Tanzania. African Journal of Reproductive Health 12(3):113–124. [PubMed] [Google Scholar]
- Faulkner LR (2003). Implications of a Needs-Based Approach to Estimating Psychiatric Workforce Requirements. Academic Psychiatry 27(4):241–246. [DOI] [PubMed] [Google Scholar]
- Lund C, Flisher AJ (2009). A model for community mental health services in South Africa. Trop Med Int Health, 14(9): 1040–1047. [DOI] [PubMed] [Google Scholar]
- Pileroodi S (2006). District health network. 3rd ed Razavieh publication, Tehran. (Persian) [Google Scholar]
- World Health Organization (2010). Workload indicators of staffing need. User's manual. WHO, Switzerland. [Google Scholar]
- Kurowski C, Wyss K, Abdulla S, Mills A (2007). Scaling up priority health interventions in Tanzania: the human resources challenge. Health Policy and Planning 22(3):113–127. [DOI] [PubMed] [Google Scholar]
- Scheffler RM, Liu JX, Kinfu Y, Poz MRD (2008). Forecasting the global shortage of physicians: an economicand needs-based approach. Bulletin of the World Health Organization, 86:516–523. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barber P, López-Valcßrcel BG (2010). Forec-asting the need for medical specialists in Spain: application of a system dynamics model. Hum-an Resources for Health, 8:24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hagopian A, Mohanty MK, Das A, House PJ (2011). Applying WHO's ‘workforce indicat-ors of staffing need' (WISN) method to calcu-late the health worker requirements for India's maternal and child health service guarantees in Orissa State. Health Policy and Planning,1–8. [DOI] [PubMed] [Google Scholar]
- Kitanda J (2008). workload-based indicators of staffing need (WISN) for health tutors in two public health training institutions in uganda. Health Policy and Development 6(1):16–30. [Google Scholar]