

Abstract
Arthroscopic Bankart repair with suture anchors is widely considered a mainstay for surgical treatment of anterior shoulder instability after recurrent anterior shoulder dislocations. Traditionally, the displaced capsulolabral complex is restored and firmly attached to the glenoid by placing multiple suture anchors individually from a 5- to 3-o'clock position. A variety of different techniques using different anchor designs and materials have been described. Knotless anchors are widely used nowadays for shoulder instability repair, providing a fast and secure way of labral fixation with favorable long-term outcomes. However, these techniques result in a concentrated point load of the reduced labrum to the glenoid at each suture anchor. We describe a technique, developed by the first author, using a 1.5-mm LabralTape (Arthrex, Naples, FL) in combination with knotless suture anchors (3.5-mm PEEK [polyether ether ketone] PushLock anchors; Arthrex), for hybrid fixation of the labrum. The LabralTape is used to secure the torn labrum to the glenoid between each suture anchor, thus potentially providing a more even pressure distribution.
Patients with symptomatic anterior glenohumeral instability that is refractory to conservative measures are treated with surgical stabilization. Since Bankart's initial description of his repair of the “essential lesion” responsible for recurrent anterior instability,1 surgeons have continually been developing and refining new techniques to stabilize the dislocating shoulder. Traditionally, these techniques have been performed through an open incision.2 However, the advent of arthroscopic technology has allowed operations to be performed in a minimally invasive fashion.3 Contemporary arthroscopic techniques use suture anchors to secure the damaged capsulolabral complex to the glenoid and to tension the attenuated inferior glenohumeral ligament complex.3,4 Knotless suture anchor techniques have been developed to maintain secure fixation of the labrum to the glenoid while avoiding potential irritation of the articular cartilage with suture knots.5,6 Nevertheless, suture anchors—with or without knots—leave intervening labral tissues without firm attachment to the glenoid rim. We describe a novel hybrid technique, developed by the first author (R.C.O.), using a 1.5-mm LabralTape (Arthrex, Naples, FL) in combination with knotless suture anchors (3.5-mm PEEK [polyether ether ketone] PushLock anchors; Arthrex). The LabralTape is secured between the suture anchors, providing an even pressure distribution and potentially encouraging biological healing of the labrum to the glenoid (Fig 1).
Fig 1.
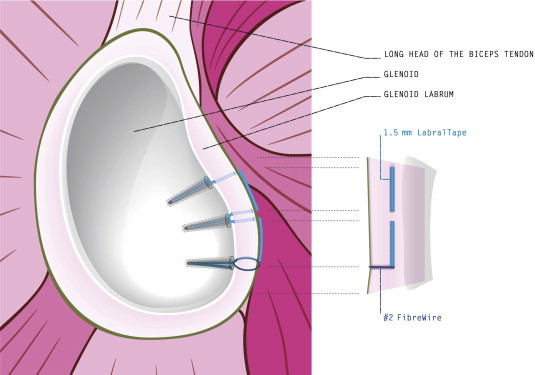
The LabralTape is secured between the suture anchors, providing an even pressure distribution and potentially encouraging biological healing of the labrum to the glenoid.
Surgical Technique
This technique is indicated for patients with a clinical history, physical examination, and diagnostic imaging consistent with an anteroinferior capsulolabral injury leading to recurrent anteroinferior glenohumeral instability (Video 1). The patient is positioned in the beach-chair position, and a standard diagnostic arthroscopy is performed through a posterior portal. The anteroinferior capsulolabral injury is identified and confirmed, and anterolateral and anteroinferior portals are established with an outside-in technique. Cannulas may be used for ease of suture passage; however, this technique may also be performed percutaneously. The labrum and capsule are elevated off of the glenoid and mobilized through the anteroinferior portal. Any adhesions or scar tissue on the glenoid is then debrided and abraded to a healthy bleeding bony surface to enhance biological healing of the labrum and capsule to bone.
The actual repair begins by passing a 45° SutureLasso (Arthrex) through the anteroinferior portal and piercing the inferior capsule and labrum. We always use a 45° left curved SutureLasso for a right shoulder and vice versa. The goals of this step are to re-tension the attenuated inferior glenohumeral ligament through a south-north shift and to prepare the inferior labrum for reattachment. The nitinol wire loop of the SutureLasso is advanced into the joint and is shuttled out through the anterolateral portal with a suture grasper. One limb of a No. 2 FiberWire suture (Arthrex) and 1 limb of a 1.5-mm LabralTape are then passed through the nitinol wire loop of the SutureLasso outside the shoulder. The nitinol wire of the SutureLasso is shuttled back to the anteroinferior portal, leaving 1 limb of FiberWire and 1 limb of LabralTape in the anterolateral portal. The remaining limb of the FiberWire suture and the remaining limb of the LabralTape within the anterolateral portal are then shuttled into the anteroinferior portal with a suture grasper.
The 1 limb of the LabralTape that was shuttled from the anterolateral portal is secured with a mosquito clamp. The location of the first anchor placement is approximately at the 5-o'clock (right shoulder) or 7-o'clock (left shoulder) position, as close as possible to the chondrolabral junction. The targeting guide is placed in this position, and a power drill is used to make the path for passage of the knotless PushLock anchor. After drilling, a nitinol wire is placed through the drill guide to confirm that the tunnel is securely in bone and to highlight the position of the tunnel. The anchor eyelet of a 3.5-mm PushLock anchor is then loaded with both ends of the FiberWire suture and the 1 end of the LabralTape secured with the mosquito clamp that was originally shuttled from the anterolateral portal (Fig 2). While appropriate tension is maintained on the FiberWire suture, the anchor is advanced through the anteroinferior portal, the nitinol wire is removed, and the anchor is placed in the prepared bone tunnel, thus securing the FiberWire suture with the labrum and 1 limb of the LabralTape at the glenoid rim (Fig 3). Both FiberWire limbs are then cut as close to the anchor position as possible with a standard suture cutter. The free end of the LabralTape, which was secured with the mosquito clamp and now leaves the bone tunnel lateral to the anchor position, is also cut with a suture cutter close to the anchor at the glenoid rim. This leaves 1 free end of the LabralTape in the anteroinferior portal.
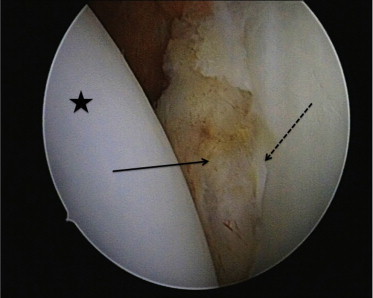
Fig 2.
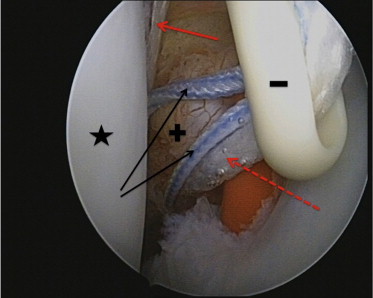
Stitch configuration before the first anchor is placed at the 7-o'clock position, viewed from a standard posterior portal in a left shoulder in the beach-chair position. In this case the bone tunnel at the chondrolabral junction is secured with a red plastic stick. The humeral head is marked with a star. Both limbs of the No. 2 FiberWire (black arrows) run through the anchor eyelet (minus sign), in addition to the 1 limb of the LabralTape that runs through the chondrolabral junction (dashed red arrow). The other limb of the LabralTape that leaves the tissue medial to the newly created capsulolabral complex/bump (plus sign) is marked with a solid red arrow.
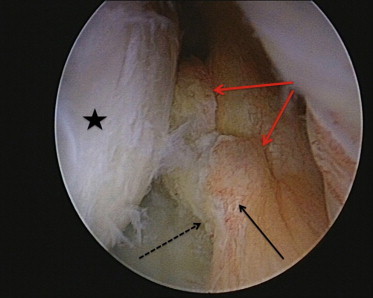
Fig 3.
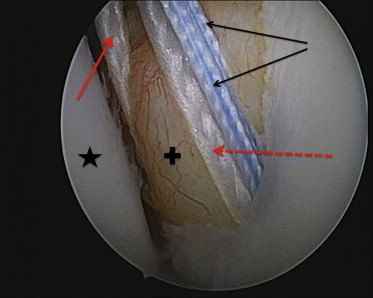
The first stitch after the anchor has been placed at the 7-o'clock position, viewed from a standard posterior portal in a left shoulder in the beach-chair position. The humeral head is marked with a star, and the newly created capsulolabral complex/bump is marked with a plus sign. Both limbs of the No. 2 FiberWire (black arrows) leave the bone tunnel at the chondrolabral junction together with 1 limb of the LabralTape (dashed red arrow). The other limb of the LabralTape that leaves the tissue medial to the newly created capsulolabral complex/bump (plus sign) is marked with a solid red arrow.
Through the anteroinferior portal, the SutureLasso is again used to pierce through the labral and capsular tissue in the area superior to the first stitch, anticipating the placement of the second anchor. The nitinol wire loop is then retrieved through the anterolateral portal. The actual SutureLasso device is removed from the shoulder through the anteroinferior portal, thus leaving the nitinol wire loop inside the shoulder with 1 end out of the anterolateral portal and 1 end out of the anteroinferior portal. The free end of the LabralTape is then passed through the nitinol wire loop parked in the anteroinferior portal, and the wire is shuttled to the anterolateral portal, thus passing the LabralTape through the labral and capsular tissue. With a suture grasper, the remaining limb of the LabralTape is retrieved and shuttled back to the anteroinferior portal. The tunnel for the second anchor is drilled at the appropriate point on the glenoid, and again, a nitinol wire is placed through the drill guide to confirm that the tunnel is securely in bone and to highlight the position of the tunnel. After that, the eyelet of the second PushLock anchor is loaded with the limb of the LabralTape in the anteroinferior portal. While appropriate tension is maintained on the LabralTape and after removal of the nitinol wire from the drilled tunnel, the PushLock anchor is advanced through the anteroinferior portal and secured on the glenoid. This aids in securing the tissue between the 2 suture anchors to the glenoid rim with the LabralTape. Next, the free end of the LabralTape is shuttled to the anterolateral portal with a suture grasper.
A SutureLasso is inserted through the anteroinferior portal, and the labral tissue is then pierced with it close to the second anchor. The nitinol wire loop is advanced and shuttled to the anterolateral portal, where it is loaded with the LabralTape. The nitinol wire loop is then shuttled back to the anteroinferior portal, thus passing the LabralTape through the labral and capsular tissue back to the anteroinferior portal. With a SutureLasso, inserted through the anteroinferior portal, the labral and capsular tissue is pierced for the final time in the area in which the third and final anchor will be placed, at approximately the 3-o'clock (right shoulder) or 9-o'clock (left shoulder) position. In the same fashion as that described earlier, the nitinol wire loop is advanced and retrieved through the anterolateral portal with a suture grasper, whereas the SutureLasso device is removed through the anteroinferior portal, thus leaving 1 end of the nitinol wire loop within each portal. Outside the anteroinferior portal, the nitinol wire loop is loaded with the LabralTape and then shuttled through the tissue to the anterolateral portal (Fig 4). The limb of the LabralTape is retrieved and shuttled back to the anteroinferior portal. Next, the tunnel for the final anchor is drilled at the desired location on the glenoid rim, and a nitinol wire is placed in the tunnel to highlight the location of the tunnel. The final PushLock anchor is then loaded with the LabralTape parked in the anteroinferior portal. While appropriate tension is maintained on the LabralTape and after removal of the nitinol wire from the drilled tunnel, the final PushLock anchor is advanced through the anteroinferior portal and secured on the glenoid. This aids in securing the tissue between the second and third suture anchors to the glenoid rim with the LabralTape. The free end of the LabralTape is cut with a suture cutter close to the anchor. This finalizes the construct, firmly securing the labral and capsular tissue to the glenoid rim all the way from the first anchor at the 5-o'clock position (right shoulder) to the final anchor at the 3-o'clock position (right shoulder) (Figs 5 and 6).
Fig 4.
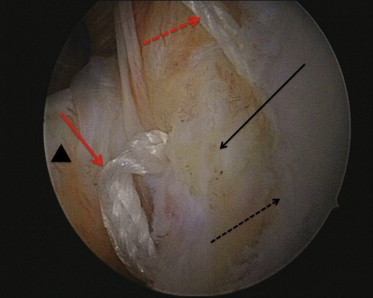
The LabralTape mattress stitch (solid red arrow) running from the second anchor to the desired position of the third anchor before tightening, viewed from a standard posterior portal in a left shoulder in the beach-chair position. The solid black arrow shows the newly created capsulolabral complex/bump, the dashed black arrow shows the chondrolabral junction, and the triangle indicates the subscapularis tendon. The dashed red arrow shows the remaining limb of the LabralTape running out of the anterolateral portal.
Fig 5.
The newly created capsulolabral complex/bump (solid arrow) after finalizing the construct, viewed from a standard posterior portal in a left shoulder in the beach-chair position. The dashed arrow marks the chondrolabral junction, and the star indicates the humeral head.
Fig 6.
The newly created capsulolabral complex/bump (solid black arrow) after finalizing the construct, viewed from the anterolateral portal. The red arrows mark the grooves within the capsular tissue, created by the LabralTape mattress stitches between the anchors. The dashed black arrow indicates the chondrolabral junction, and the star marks the humeral head. The newly created capsulolabral complex/bump seems well perfused because small vessels can still be observed.
Discussion
Two critical factors for a positive outcome of arthroscopic shoulder stabilization are re-tensioning of the inferior glenohumeral ligament and secure fixation of the labrum and capsule to the glenoid.4 This article presents a novel arthroscopic technique designed to optimize secure fixation across the entire length of the capsulolabral complex. The main potential advantage of this technique is that the LabralTape provides secure fixation of the labral tissue between each suture anchor, creating some kind of seal; this provides a more uniform pressure distribution of the entire labrum when compared with traditional techniques, in which the labrum is secured only with “spot welds” at each anchor (Table 1). Because tissue-to-bone healing is what we want to achieve when performing a Bankart repair, one could expect that this is achieved to a superior grade if the tissue is attached to the bone over a larger total length. The labral bridge technique exactly seems to provide this when compared with traditional techniques. The second potential advantage is that this technique avoids the direct labral fixation to the second and third anchors in a horizontal way, thus potentially preventing interruption of the blood supply to the labrum and capsule because the vessels in this portion of the labrum tend to run in a more longitudinal way (Fig 6).7 Furthermore, it has been shown that a horizontal suture anchor repair seems to better restore labral height and anatomy when compared with a simple suture technique.8 The third advantage is that because of the knotless fixation, the amount of suture material in direct contact with the articular cartilage is minimized.9
Table 1.
Advantages and Disadvantages of Labral Bridge Technique
| Advantages |
| Allows secure fixation with uniform pressure distribution from inferior to superior throughout repair construct |
| Avoids spot welds of fixation across repair construct |
| Optimizes blood supply to labral tissue by avoiding constricting horizontal fixation of labrum at level of each anchor |
| Places suture material away from articular cartilage, therefore minimizing risk of articular abrasion and degeneration |
| Disadvantages |
| Technically demanding |
| Technical mistakes in middle of operation are difficult to revise |
| Failure of single point of fixation leads to failure of entire construct |
The main potential disadvantage of this technique is that it is technically demanding and has a high learning curve; therefore we recommend caution to the novice arthroscopist performing this technique. In particular, interlooping of the No. 2 FiberWire limbs and the LabralTape limbs within the anteroinferior portal before placing the first anchor is a potential pitfall, and this step of the procedure should be performed with special caution (Table 2).
Table 2.
Technical Pearls and Pitfalls of Labral Bridge Technique
| Pearls |
| Creation of sufficient labral bump at chondrolabral junction by LabralTape mattress stitches |
| Pitfalls |
| Interlooping of No. 2 FiberWire limbs and LabralTape limbs within anteroinferior portal before placing first anchor |
| Placement of LabralTape mattress stitches too loosely |
| Breakage of nitinol wire loop |
Because no biomechanical data are available yet, another possible disadvantage might be inferior fixation strength and lower ultimate load–to–failure values compared with more traditional techniques. The labral bridge technique warrants further studies to evaluate the potential biomechanical and clinical advantages or even disadvantages of this technique compared with more traditional methods.
Footnotes
The authors report that they have no conflicts of interest in the authorship and publication of this article.
Supplementary Data
The labral bridge technique in a typical young male patient with traumatic anterior glenohumeral instability of the left shoulder operated on in the beach-chair position, viewed from a posterior portal. After diagnostic arthroscopy, anterolateral and anteroinferior portals are established. Through these 2 portals, the labral bridge technique, as described in this article, is used to anatomically reconstruct the anatomy of the anteroinferior labrum and attenuated inferior glenohumeral ligament complex.
References
- 1.Bankart A.S., Cantab M.C. Recurrent or habitual dislocation of the shoulder-joint. 1923. Clin Orthop Relat Res. 1993;(291):3–6. [PubMed] [Google Scholar]
- 2.Rowe C.R., Patel D., Southmayd W.W. The Bankart procedure: A long-term end-result study. J Bone Joint Surg Am. 1978;60:1–16. [PubMed] [Google Scholar]
- 3.Pope E.J., Ward J.P., Rokito A.S. Anterior shoulder instability—A history of arthroscopic treatment. Bull NYU Hosp Jt Dis. 2011;69:44–49. [PubMed] [Google Scholar]
- 4.Cole B.J., Romeo A.A. Arthroscopic shoulder stabilization with suture anchors: Technique, technology, and pitfalls. Clin Orthop Relat Res. 2001;(390):17–30. doi: 10.1097/00003086-200109000-00005. [DOI] [PubMed] [Google Scholar]
- 5.Ng D.Z., Kumar V.P. Arthroscopic Bankart repair using knot-tying versus knotless suture anchors: Is there a difference? Arthroscopy. 2014;30:422–427. doi: 10.1016/j.arthro.2014.01.005. [DOI] [PubMed] [Google Scholar]
- 6.Dines J.S., Elattrache N.S. Horizontal mattress with a knotless anchor to better recreate the normal superior labrum anatomy. Arthroscopy. 2008;24:1422–1425. doi: 10.1016/j.arthro.2008.06.012. [DOI] [PubMed] [Google Scholar]
- 7.Cooper D.E., Arnoczky S.P., O’Brien S.J., Warren R.F., DiCarlo E., Allen A.A. Anatomy, histology, and vascularity of the glenoid labrum. An anatomical study. J Bone Joint Surg Am. 1992;74:46–52. [PubMed] [Google Scholar]
- 8.Hagstrom L.S., Marzo J.M. Simple versus horizontal suture anchor repair of Bankart lesions: Which better restores labral anatomy? Arthroscopy. 2013;29:325–329. doi: 10.1016/j.arthro.2012.08.025. [DOI] [PubMed] [Google Scholar]
- 9.Byram I.R., Dunn W.R., Kuhn J.E. Humeral head abrasion: An association with failed superior labrum anterior posterior repairs. J Shoulder Elbow Surg. 2011;20:92–97. doi: 10.1016/j.jse.2010.05.013. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
The labral bridge technique in a typical young male patient with traumatic anterior glenohumeral instability of the left shoulder operated on in the beach-chair position, viewed from a posterior portal. After diagnostic arthroscopy, anterolateral and anteroinferior portals are established. Through these 2 portals, the labral bridge technique, as described in this article, is used to anatomically reconstruct the anatomy of the anteroinferior labrum and attenuated inferior glenohumeral ligament complex.