

Abstract
We describe an all-suture transosseous repair technique used in the management of rotator cuff tears by means of an all-suture anchor secured on the intra-articular side of the humeral calcar. The technique uses an anterior cruciate ligament guide to ensure accurate positioning of the tunnels, avoiding the articular cartilage and minimizing risk to the neurovascular structures. The distal end of the guide is inserted through a rotator interval portal and passed down to the axillary pouch. The proximal end of the guide is approximated to the greater tuberosity at the cuff footprint, and a complete transosseous tunnel is created with a 2.4-mm drill. An all-suture implant is inserted through this tunnel down to the calcar, and its deployment is visualized under arthroscopy. Gentle traction is applied to the anchor, resulting in a 4-mm concertina of the suture anchor that rests opposed to the medial cortex. The major advantage of this technique is the fixation strength gained from the biomechanically superior cortical bone of the calcar. Furthermore, this method permits greater preservation of bone surface area at the level of the footprint for a larger tendon-to-bone healing surface. This technique also provides an excellent alternative in revision situations.
Rotator cuff pathology is a common problem, with an incidence of 87 per 100,000 person-years. The highest incidence of this pathology is seen in women and in the age group 55 to 59 years.1,2 Surgical management of rotator cuff tears has shown predictable pain relief and functional improvement, with good overall patient satisfaction.3
Over the past 20 years, multiple techniques have been described for repairing rotator cuff tendons back to their insertion on the proximal humerus with the aim of restoring them to the anatomic footprint. These include open, mini-open, and arthroscopic approaches with single- and double-row suture configurations.4 Notably, double-row suture repair techniques are considered to increase the tendon-footprint contact area, with the intention of improving functional outcomes and healing rates.5
Rotator cuff repair with transosseous sutures was first described by McLaughlin.6 Garofalo et al.7 further developed this technique for suturing the torn rotator cuff back to the greater tuberosity in an all-arthroscopic manner without the use of anchors and declared this new technique the gold standard for rotator cuff repair. We have developed a complete transosseous technique to maximize the tendon-footprint contact area and improve fixation, which we have termed all-suture transosseous rotator cuff repair.
Several studies have compared traditional transosseous repairs with single- and double-row configurations, the results of which have shown that load to failure is higher in transosseous repairs.4,8 Transosseous rotator cuff repairs are known to fail most commonly at the bone-anchor interface. This failure occurs more frequently in osteoporotic bone, which is a significant concern for surgeons performing rotator cuff repairs in increasingly elderly populations. Bone quality studies with high-resolution micro–computed tomography have shown that a more superior bone stock is located adjacent to the articular surface of the humeral head (calcar region) than the more cancellous bone found in the region of the greater tuberosity.9,10 By using the all-suture transosseous repair technique, cortical transosseous fixation is achieved at the medial humeral intra-articular cortex.
Surgical Technique
The patient is placed in the beach-chair position. Surface landmarks for the underlying bony anatomy are marked on the skin before commencing surgery. Anterior, lateral, posterior, anterolateral, and posterolateral arthroscopic portals are used to perform our technique (Video 1).
First, a wide bursectomy and footprint preparation are performed in the subacromial space to improve visualization. The rotator cuff tear pattern is then assessed to determine the optimal method of reducing the cuff to the footprint.
Step 1
Viewing is commenced through a standard posterior portal. An anterior portal is created using an outside-in technique at the level of the rotator interval. This anterior portal should be large enough to permit the passage of the distal limb of the anterior cruciate ligament (ACL) guide (Acufex Director ACL system; Smith & Nephew, Andover, MA). This is approximately 8 mm. The distal limb of the guide is introduced through an interval portal and passed down to the medial humeral calcar at the level of the axillary pouch. Care should be taken with the straight section of the guide because this does not match the curvature of the humeral head (Table 1). The guide should be directed along the course of the anterior band of the inferior glenohumeral ligament down to its humeral attachment in the axilla. It is then opposed to the strong cortical bone adjacent to the articular cartilage (Fig 1) under arthroscopic guidance from a posterior standard viewing portal.
Table 1.
Tips and Pitfalls of All-Suture Transosseous Rotator Cuff Repair Technique
| Tips |
| Ensure that the rotator interval portal is positioned to accommodate the guide and allow its inferior positioning. |
| Stabilize the guide laterally and medially until the anchor is inserted. |
| Perform gentle anchor introduction through the prepared pilot hole. |
| Apply light traction, which enables optimal anchor deployment and calcar fixation; always check under direct visualization. |
| Pitfalls |
| To avoid articular cartilage damage, be aware that the ACL guide is not contoured to the curvature of the humeral head. |
| Ensure that guide positioning and drilling occur under direct visualization to reduce the risk of axillary nerve injury. |
| Bear in mind that strong initial traction may hinder proper anchor deployment with an anomalous fixation. |
| Be aware of longer suture limbs running through the tunnels; lock the knots properly. |
ACL, anterior cruciate ligament.
Fig 1.
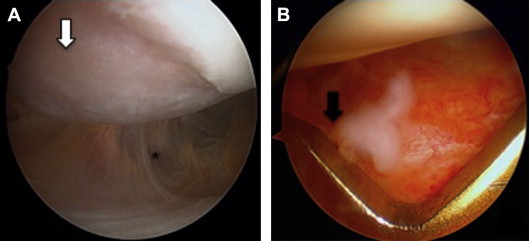
(A) Arthroscopic view of the glenohumeral joint (left side) from the standard posterior portal showing the inferior capsular recess (asterisk) and inferior bare area (arrow). (B) From the anterior portal, the distal limb of the anterior cruciate ligament guide is introduced through the rotator interval and passed down along the anteroinferior glenohumeral ligament to the medial humeral calcar at the level of the axillary pouch (arrow).
Step 2
Next, an anterolateral portal is created at the level of the cuff defect on the footprint. Here, the proximal component of the guide can be inserted and positioned at the desired position on the rotator cuff footprint (Fig 2). Before guide positioning is completed, light decortication of the greater tuberosity is highly recommended to promote cancellous bone bleeding to achieve better tendon-to-bone healing. Once the guide is correctly positioned, it can be stabilized by using its locking-teeth mechanism (Video 1).
Fig 2.
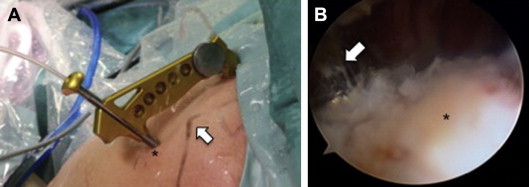
(A) Outside view of left shoulder in beach-chair position. After the anterolateral portal (asterisk) is created at the level of the cuff defect (aligned with the anterolateral corner of the acromion [arrow]), the proximal component of the guide is inserted. (B) Inside view from posterior portal. The proximal limb of the anterior cruciate ligament guide (arrow) is positioned at the lateral aspect of the greater tuberosity (asterisk).
Step 3
Correct positioning of the guide is finally confirmed at the calcar and greater tuberosity using the posterior viewing portal. Once this is satisfactorily achieved, the 2.4-mm drill (Acufex Director ACL system) is introduced to create a transosseous tunnel (Fig 3, Video 1). It is important to penetrate the medial cortex of the humerus with caution because it exits at the level of the humeral calcar. Breaching the inferior capsule should be avoided to minimize any risk of damage to the axillary nerve.
Fig 3.
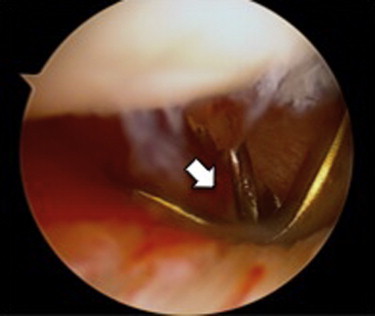
Arthroscopic view from posterior portal (left shoulder). Correct positioning of the guide is confirmed at the level of the greater tuberosity and at the calcar. Once it has been secured, the 2.4-mm drill is used to create a transosseous tunnel (arrow).
Step 4
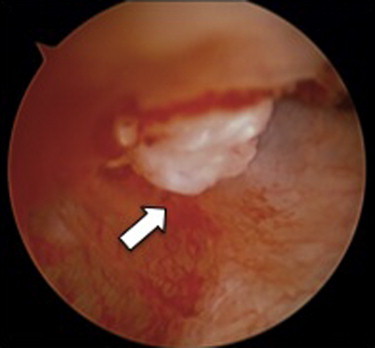
A 2.3-mm all-suture anchor (Iconix; Stryker Endoscopy, San Jose, CA) is inserted by gentle impaction through the transosseous tunnel until the implant emerges completely through the medial calcar. This can be seen in the axillary pouch by viewing through the posterior portal (Fig 4, Video 1). The anchor is then deployed by placing gentle traction on the proximal suture ends. The fixation strength and stability can be checked under arthroscopy (Fig 5, Video 1). The rest of the cuff repair then proceeds using the surgeon's preferred technique for suture passage through the cuff.
Fig 4.

Arthroscopic view from posterior portal (left shoulder). After drilling, the all-suture implant is inserted completely through the transosseous tunnel into the axillary pouch until reaching the elbow of the guide (arrow).
Fig 5.
Arthroscopic view from posterior portal (left shoulder). The anchor has been introduced through the guide and rests at the medial humeral calcar; light traction is applied to deploy the all-suture anchor until it engages (arrow).
Discussion
Rotator cuff tears occur frequently in elderly persons in whom surgery is performed to improve pain and functional disability when conservative measures fail.2 In these patients, anchor fixation can be a concern in the relatively osteoporotic bone of the greater tuberosity. Our all-transosseous technique improves this potential weakness of the anchor fixation.
The basis of the all-suture anchor fixation relies on the increased diameter of the all-suture anchor, from 2.3 to 4.0 mm, once it has been deployed. This small initial anchor size requires that the diameter of the transosseous tunnel need only be 2.4 mm extending from the greater tuberosity to the humeral calcar. This medial cortical fixation improves the pullout strength of the anchor as compared with the weaker cancellous bone of the greater tuberosity.
A further advantage of this technique occurs through greater preservation of the bony surface area at the level of the cuff footprint (Table 2). Creating these small-diameter footprint tunnels maximizes the tendon-footprint contact area, and subsequently, the bone-tendon healing area is substantially increased as compared with traditional larger anchors. This technique is ideally suited to revision cases in which previous anchor pullout has occurred or in which traditional anchors have been placed very close to one another8,11,12 (Fig 6).
Table 2.
Advantages and Disadvantages of All-Suture Transosseous Repair Technique
| Advantages |
| Footprint bone preservation |
| Increased tendon-to-bone healing |
| Strong medial cortical bone fixation |
| Not strictly footprint bone dependent |
| Disadvantages |
| Shoulder-specific guide not available |
| Technically more demanding |
| Not every axillary pouch is wide |
Fig 6.
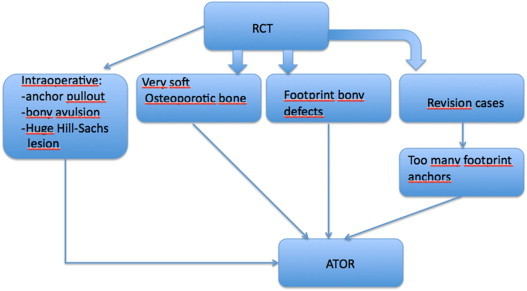
Indications for all-suture transosseous repair (ATOR) technique. Intraoperatively, all-suture transosseous repair is indicated in the following different scenarios: (1) anchor pullout, bony avulsion, and huge Hill-Sachs lesions; (2) very soft osteoporotic bone; (3) footprint bony defects; and (4) revision cases, in which there is very little space at the footprint and leaving as much tendon-to-bone contact as possible is desired. (RCT, rotator cuff tear.)
Our technique involves drilling a transosseous tunnel to the axillary pouch using an ACL guide to ensure accurate and safe drill placement. This is performed under direct arthroscopic visualization. The procedure remains an intra-articular procedure with minimal risk to the axillary nerve, which runs extra-articularly crossing the axilla. Anatomic studies have shown mean distances between the nerve and the articular surface of 7 mm.13,14 It is possible to use multiple anchors with this technique. One limitation of the technique is occasional difficulty accessing the posterior aspect of the humeral calcar. This occurs because of the use of a guide designed for use in the knee, which is not adapted to the different anatomy of the proximal humerus.
The arthroscopic all-suture transosseous repair for rotator cuff repairs is based on strong medial calcar fixation and allows complete transosseous fixation. This allows greater bone stock preservation and the resultant larger bone-to-tendon healing footprint surface area. This technique is especially useful in revision situations.
Footnotes
The authors report the following potential conflict of interest or source of funding: M.A-G. receives support from expert meetings. Biomet, Stryker, and DePuy Mitek. Shoulder courses.
Supplementary Data
Surgical steps for performing an all-suture transosseous repair technique, that is, a transosseous rotator cuff repair using an all-suture anchor that is secured on the intra-articular side of the humeral calcar by means of a knee anterior cruciate ligament guide.
References
- 1.Jain N.B., Higgins L.D., Losina E., Collins J., Blazar P.E., Katz J.N. Epidemiology of musculoskeletal upper extremity ambulatory surgery in the United States. BMC Musculoskelet Disord. 2014;15:4. doi: 10.1186/1471-2474-15-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.White J.J., Titchener A.G., Fakis A., Tambe A.A., Hubbard R.B., Clark D.I. An epidemiological study of rotator cuff pathology using The Health Improvement Network database. Bone Joint J. 2014;96:350–353. doi: 10.1302/0301-620X.96B3.32336. [DOI] [PubMed] [Google Scholar]
- 3.Ensor K.L., Kwon Y.W., Dibeneditto M.R., Zuckerman J.D., Rokito A.S. The rising incidence of rotator cuff repairs. J Shoulder Elbow Surg. 2013;22:1628–1632. doi: 10.1016/j.jse.2013.01.006. [DOI] [PubMed] [Google Scholar]
- 4.Lavery K.P., Rasmussen J.F., Dhawan A. Arthroscopic transosseous-equivalent rotator cuff repair. Arthrosc Tech. 2013;2:e183–e185. doi: 10.1016/j.eats.2013.02.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Millett P.J., Warth R.J., Dornan G.J., Lee J.T., Spiegl U.J. Clinical and structural outcomes after arthroscopic single-row versus double-row rotator cuff repair: A systematic review and meta-analysis of level I randomized clinical trials. J Shoulder Elbow Surg. 2014;23:586–597. doi: 10.1016/j.jse.2013.10.006. [DOI] [PubMed] [Google Scholar]
- 6.McLaughlin H.L. Lesions of the musculotendinous cuff of the shoulder. The exposure and treatment of tears with retraction. 1944. Clin Orthop Relat Res. 1994;(304):3–9. [PubMed] [Google Scholar]
- 7.Garofalo R., Castagna A., Borroni M., Krishnan S.G. Arthroscopic transosseous (anchorless) rotator cuff repair. Knee Surg Sports Traumatol Arthrosc. 2012;20:1031–1035. doi: 10.1007/s00167-011-1725-4. [DOI] [PubMed] [Google Scholar]
- 8.Lee T.Q. Current biomechanical concepts for rotator cuff repair. Clin Orthop Surg. 2013;5:89–97. doi: 10.4055/cios.2013.5.2.89. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Garrigues G.E., Lazarus M.D. Arthroscopic bone tunnel augmentation for rotator cuff repair. Orthopedics. 2012;35:392–397. doi: 10.3928/01477447-20120426-04. [DOI] [PubMed] [Google Scholar]
- 10.Kirchhoff C., Braunstein V., Milz S. Assessment of bone quality within the tuberosities of the osteoporotic humeral head: Relevance for anchor positioning in rotator cuff repair. Am J Sports Med. 2010;38:564–569. doi: 10.1177/0363546509354989. [DOI] [PubMed] [Google Scholar]
- 11.Aleem A.W., Brophy R.H. Outcomes of rotator cuff surgery: What does the evidence tell us? Clin Sports Med. 2012;31:665–674. doi: 10.1016/j.csm.2012.07.004. [DOI] [PubMed] [Google Scholar]
- 12.Kuroda S., Ishige N., Mikasa M. Advantages of arthroscopic transosseous suture repair of the rotator cuff without the use of anchors. Clin Orthop Relat Res. 2013;471:3514–3522. doi: 10.1007/s11999-013-3148-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Nijs S., Sermon A., Broos P. Intramedullary fixation of proximal humerus fractures: Do locking bolts endanger the axillary nerve or the ascending branch of the anterior circumflex artery? A cadaveric study. Patient Saf Surg. 2008;2:33. doi: 10.1186/1754-9493-2-33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Bono C.M., Grossman M.G., Hochwald N., Tornetta P. Radial and axillary nerves. Anatomic considerations for humeral fixation. Clin Orthop Relat Res. 2000;373:259–264. [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Surgical steps for performing an all-suture transosseous repair technique, that is, a transosseous rotator cuff repair using an all-suture anchor that is secured on the intra-articular side of the humeral calcar by means of a knee anterior cruciate ligament guide.