

Abstract
Meniscal tears are among the most commonly diagnosed knee injuries and often require surgical intervention. Understanding the types of meniscal tears and treatment options is paramount to caring for the young athlete. Sports medicine and arthroscopic physicians now recognize that meniscal preservation in the young athlete is essential to the long-term health and function of the knee. Although uncommon, the discoid lateral meniscus is more prone to injury because of its increased thickness and lack of blood supply. Because of the abnormal development, the peripheral attachments are frequently absent and instability often persists after a partial meniscectomy. If the instability is unrecognized during the initial treatment, a recurrence of pain and mechanical symptoms is likely and a subsequent subtotal meniscectomy may be the only treatment option. With increased awareness, arthroscopic saucerization accompanied by arthroscopically assisted inside-out meniscal repair is a preferable treatment option with an excellent outcome.
The prevalence of meniscal tears reported in the young athlete has escalated in recent years. This may be attributable to an increase in sports participation, as well as greater clinical suspicion.1 The sports medicine physician should be familiar with not only the more common meniscal pathology but also the less frequent symptoms of the discoid meniscus. Although Young2 originally described the discoid meniscus in 1887, the diagnosis and treatment remain controversial and surgical management continues to evolve.
The overall incidence of discoid menisci in the United States is 3% to 5%.3 Most discoid meniscus variants are asymptomatic in the pediatric population. Younger patients may present with the classical snapping knee syndrome. Initially, this may be painless, but the condition often progresses to mechanical symptoms and loss of range of motion.4 In contrast, adolescent meniscal tears most commonly are associated with a traumatic event.1,5 This is the scenario in our case of a wrestler who sustained a tear of the discoid lateral meniscus after maneuvering from a flexed-knee position with an opponent on his back.
Historical treatment would have advocated a total meniscectomy. Prior studies in which total meniscectomy was performed have shown good short-term results and poor long-term results with the development of early advanced arthritis.6,7 More recent literature promotes meniscal preservation with saucerization accompanied by repair of unstable discoid meniscal tears. Ahn et al.8 performed a retrospective study that examined 23 patients with symptomatic discoid meniscal tears with peripheral instability. Arthroscopic debridement followed by meniscal peripheral repair was performed in all cases and yielded good results at 51 months of follow-up, with no reoperations. Our technique illustrates operative treatment of a radial tear of the inner third of the meniscus (Fig 1) along with an unstable posterior horn in a discoid lateral meniscus, which was subsequently treated with saucerization and peripheral repair (Fig 2) by an inside-out technique (Video 1).
Fig 1.

Frontal and top views of a knee showing an inner-third radial tear of the discoid lateral meniscus.
Fig 2.

Frontal and top views of a knee showing saucerization and peripheral repair of the posterior horn of an unstable discoid lateral meniscus.
Surgical Technique
A traditional knee arthroscopy setup is adequate to perform arthroscopic-assisted discoid lateral meniscal saucerization and repair. Use of a proximal tourniquet and leg holder is recommended for ample room for repair. We also prefer to mark our surgical incision for inside-out repair before performing arthroscopy so that landmarks are not distorted after insufflation of the knee with arthroscopic fluid. A diagnostic knee arthroscopy is performed through the standard anteromedial and anterolateral portals. A hook probe (Smith & Nephew, Andover, MA) is used to confirm a lateral meniscal tear (Fig 3), as well as an unstable posterior peripheral attachment, by placing the probe in the popliteal hiatus and pulling the posterior horn anteriorly (Fig 4). Additional knee pathology may be addressed in the same setting.
Fig 3.

Arthroscopic view of a discoid lateral meniscus with a radial tear (arrow) in a left knee, viewing through an anterolateral portal.
Fig 4.

Arthroscopic view of an unstable discoid lateral meniscus with a radial tear in a left knee, viewing through an anterolateral portal. A probe (arrow) is being used to pull the posterior horn anteriorly.
Once the tear pattern is confirmed, an arthroscopic punch (Smith & Nephew) and shaver (Smith & Nephew) are used to perform saucerization of the discoid meniscus (Fig 5). Meniscal instability is again confirmed, and preparation for repair is undertaken. We initially stimulate a healing environment with a meniscal rasp (ConMed Linvatec, Largo, FL) and a 22-gauge, 3.5-inch-long spinal needle (Kimberly-Clark, Irving, TX) to create vascular access channels.
Fig 5.

Arthroscopic view of the discoid lateral meniscus after saucerization in a left knee, viewing through an anterolateral portal.
We then perform a standard inside-out meniscal repair by incising our previously marked incision parallel and just posterior to the lateral collateral ligament with the knee in 45° of flexion. This is carried down to the fascia just anterior to the biceps, and the fascia is incised and retracted posteriorly to expose the interval between the lateral posterior capsule and gastrocnemius. This allows a medium Graves speculum blade (MedGyn, Addison, IL) to be positioned as a meniscal retractor to aid in retrieving sutures and protecting the neurovascular structures behind the knee.
Once the retractor is in place, the arthroscope is then positioned in the anterolateral portal and the posterior left zone–specific cannula (ConMed Linvatec) is positioned in the anteromedial portal. The surgical assistant passes multiple meniscal repair needles with Orthocord (DePuy Mitek, Raynham, MA) in a vertical mattress configuration using the zone-specific cannulas. We prefer a high-strength partially absorbable suture for repair to minimize the potential for chondral abrasion. The repair proceeds from the posterior horn to the meniscal body to secure the meniscus to the posterior capsule (Fig 6). The suture needles are retrieved under direct visualization through the previously prepared lateral incision (Fig 7). The sutures are tagged in preparation to be tied over the capsule after all the sutures have been passed. Once the final repair has been accomplished, a microfracture awl (Arthrex, Naples, FL) is used in the notch to release bone marrow into the knee in an effort to promote a healing environment for the repair. The arthroscopic portals and lateral incision are closed in the standard surgical fashion, and a dry sterile dressing is applied along with a knee immobilizer. A postoperative protocol consisting of immediate full weight bearing in extension with graduated flexion is advanced under the supervision of a physical therapist.
Fig 6.

Arthroscopic view of an unstable discoid lateral meniscus after saucerization and inside-out suture repair (arrow) of the posterior horn in a left knee, viewing through an anterolateral portal.
Fig 7.
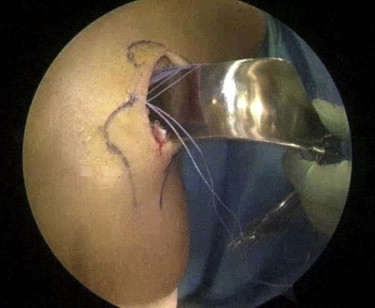
Outside view of a left knee showing a lateral meniscal repair approach with a speculum used as a meniscal retractor. The sutures (purple) were passed and retrieved using an inside-out technique during saucerization and repair of an unstable discoid lateral meniscus.
Discussion
Acute traumatic hemarthrosis of the knee in the young athlete should raise suspicion for an intra-articular injury.5 The enhanced use of magnetic resonance imaging coupled with a heightened awareness has resulted in an increase in diagnosis and subsequent surgical intervention for pediatric meniscal tears.1 Historical treatment of discoid lateral meniscal tears has shown poor long-term results with total meniscectomy.6,7 An evolution in the contemporary literature strongly supports repair with meniscal preservation in an effort to restore long-term function.8 Recent literature also supports a timely repair for isolated discoid meniscal tears to decrease the incidence of articular cartilage lesions.9
The orthopaedic surgeon preparing to address a torn lateral meniscus should be equipped to handle an unstable discoid meniscus. The advantages of the described technique (Table 1) are that we use standard knee arthroscopic skills combined with an inside-out repair technique coupled with a high-strength partially absorbable vertical mattress suture configuration. Compared with recent all-inside repair techniques, the traditional inside-out technique for lateral meniscal repair may be considered unfavorable because of its invasiveness and proximity to the surrounding neurovascular structures. We believe that if this technique is consistent with prior descriptions in the literature and if performed properly, the risks are minimized and healing is optimized. Our short-term clinical outcome at 1 year is promising, with the patient showing painless full range of motion without an effusion. Although the discoid lateral meniscus is uncommon, this technique should be a part of the surgeon's armamentarium not only to address the radial meniscal tear but also to safely provide peripheral stabilization to the unstable posterior horn.
Table 1.
Advantages of Arthroscopic Saucerization and Repair of Discoid Lateral Meniscal Tear
| Standard knee arthroscopic setup and portals |
| No special instrumentation required |
| Standard meniscectomy and repair skills |
| Preservation and stabilization of remainder of lateral meniscus |
| Safe approach to meniscal repair to minimize neurovascular damage |
| Partially absorbable high-strength meniscal repair sutures to reduce potential chondral injury |
| Marrow-stimulation techniques to promote healing |
Footnotes
The authors report the following potential conflict of interest or source of funding: This work was supported by Arthrex, Bon Secours, DJO, DePuy Mitek, and Smith & Nephew.
Supplementary Data
Technique for arthroscopic treatment of a radial tear of the inner third of an unstable discoid lateral meniscus with saucerization and peripheral repair by an inside-out suture technique.
References
- 1.Brown T.D., Davis J.T. Meniscal injury in the skeletally immature patient. In: Micheli L.J., Kocher M.S., editors. The pediatric and adolescent knee. Elsevier; Philadelphia: 2006. pp. 236–259. [Google Scholar]
- 2.Young R.B. Williams and Norgate; London: 1889. Memoirs and memoranda in anatomy. [Google Scholar]
- 3.Jordan M.R. Lateral meniscal variants: Evaluation and treatment. J Am Acad Orthop Surg. 1996;4:191–200. doi: 10.5435/00124635-199607000-00003. [DOI] [PubMed] [Google Scholar]
- 4.Dickhaut S.C., DeLee J.C. The discoid lateral-meniscus syndrome. J Bone Joint Surg Am. 1982;64:1068–1073. [PubMed] [Google Scholar]
- 5.Stanitski C.L., Harvell J.C., Fu F. Observations on acute knee hemarthrosis in children and adolescents. J Pediatr Orthop. 1993;13:506–510. doi: 10.1097/01241398-199307000-00016. [DOI] [PubMed] [Google Scholar]
- 6.Raber D.A., Friederich N.F., Hefti F. Discoid lateral meniscus in children: Long-term follow-up after total meniscectomy. J Bone Joint Surg Am. 1998;80:1579–1586. doi: 10.2106/00004623-199811000-00003. [DOI] [PubMed] [Google Scholar]
- 7.Washington E.R., III, Root L., Liener U.C. Discoid lateral meniscus in children: Long-term follow-up after excision. J Bone Joint Surg Am. 1995;77:1357–1361. doi: 10.2106/00004623-199509000-00011. [DOI] [PubMed] [Google Scholar]
- 8.Ahn J.H., Lee S.H., Yoo J.C., Lee Y.S., Ha H.C. Arthroscopic partial meniscectomy with repair of symptomatic discoid lateral meniscus tears in children: Results of a minimum 2 year follow-up. Arthroscopy. 2008;24:888–898. doi: 10.1016/j.arthro.2008.03.002. [DOI] [PubMed] [Google Scholar]
- 9.Fu D., Guo L., Yang L., Chen G., Duan X. Discoid lateral meniscus tears and concomitant articular cartilage lesions in the knee. Arthroscopy. 2014;30:311–318. doi: 10.1016/j.arthro.2013.11.029. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Technique for arthroscopic treatment of a radial tear of the inner third of an unstable discoid lateral meniscus with saucerization and peripheral repair by an inside-out suture technique.