

Abstract
Objectives:
To introduce an effective and safe ophthalmic triaging system to be used by non-ophthalmologists.
Methods:
A modified scoring triage system with more relevant clinical symptoms and signs from a previously published Rome Eye Scoring System for Urgency and Emergency (RESCUE) was evaluated over a 2-month period. The study was conducted following a prospective cohort design between March and September 2014 at King Abdulaziz University Hospital, Riyadh, Saudi Arabia. Only self-referred patients were included. Its reliability in differentiating urgent and semi-urgent conditions from non-urgent conditions, identifying patients who need immediate intervention, and decreasing the waiting time were tested using Mann Whitney U test.
Results:
A total of 531 patients were included in the validation phase to evaluate the triaging system reliability, and 824 patients were included in the implementation phase (applying the system in the ophthalmology emergency room). The sensitivity to differentiate urgent and semi-urgent conditions from non-urgent conditions improved from 90.7 to 98.7%, while the specificity decreased from 97.2 to 87% compared with RESCUE. The sensitivity in differentiating urgent conditions from semi-urgent and non-urgent conditions was 99%, and the specificity was 90%. Mean waiting time reduced from 58.23 minutes to 46 minutes (p=0.014), and the median waiting time reduced from 46 minutes to 33 minutes (p=0.009).
Conclusion:
This triage system appears to be safe and effective in recognizing the urgency of different ophthalmic conditions, reducing unnecessary ophthalmic emergency load and waiting time significantly.
The ophthalmology emergency room (OER) receives patients from different referral sources; such as self-referred, referral from general practitioners, optometrists, or other secondary or tertiary hospitals.1 The number of self-referrals in a dedicated OER was found to be as high as 89% of the patients who attended the OER.2 One major reason for a loaded emergency room (ER) by patients is expected to be related to receiving large number of patients with non-emergency conditions. Only 25% of patients presenting to the ER were found to have urgent medical conditions by using a triaging process.3 Emergency room visits by patients with non-urgent conditions contributes to long waiting times and patients’ frustration with the service.4 Handling an acute ophthalmic condition is different from the management of general acute medical conditions. It can be challenging for general emergency physicians and nurses to manage patients with ophthalmic complaints, because there are many acute ophthalmic conditions that can be vision threatening without obvious clinical findings.5 Therefore, because of the unique presentations of acute ophthalmic conditions, it might be risky to manage the situation entirely by general medical doctors.6 Considering such conditions, a reliable ophthalmic triaging system would be of great benefit for non-ophthalmologists working at acute care services to manage peculiar presentations of some of the acute ophthalmic problems. Limited literature exists on OER triage. Further research in this area including triage scales, facilities for triage, qualifications, and experience of triage personnel, triage standards, and guidelines are needed. Revisions of the triage criteria should focus on reducing the unnecessary use of emergency services without compromising the clinical safety.7 A recent study carried out in King Abdul Aziz University Hospital’s OER in 2013 during the month of July found that 1,094 self-referred patients were seen during that month. Out of those 1,094 patients, 712 (65.1%) were found to have non-urgent conditions after they were examined by the OER doctors.8 Lack of an appropriate triaging system for OER with high sensitivity has drawn our attention to address this urgent need for developing a new ophthalmic triage system. We introduce here a newly developed ophthalmic triage system, which gives the priority to emergency patients to be attended first among self-referred patients presenting to the OER. Our proposed ophthalmic triage system is a modified version of the Rome Eye Scoring System for Urgency and Emergency (RESCUE).9 The modification was carried out to overcome some of the limitations of the RESCUE; such as the considerable potential to miss patients with serious ophthalmic conditions as the sensitivity was only 90.7%, and not including important clinical parameters that are known to be the presentations of serious ophthalmic emergency conditions. The main objectives of this project were to evaluate the effectiveness of the newly modified ophthalmic triage system on recognizing patients with emergency ophthalmic conditions and giving the priority to patients according to the level of urgency of the ophthalmic condition.
Methods
This project was conducted at a dedicated OER of a tertiary hospital in Riyadh, Saudi Arabia. Approval was obtained from the Research Review Board (RRB), Department of Ophthalmology, King Abdul-Aziz University Hospital where the research project adhered to the tenets of the Declaration of Helsinki for research involving humans. Oral consent was sought from emergency patients in phase I (validation phase), while in phase II (implantation phase) the triage was set as a policy for the emergency room. All recruited subjects agreed to participate in the current study. Literature was carefully reviewed for similar studies following a meticulous search strategy. Relevant scientific databases such as PubMed, Medline, and Google scholar were used. The reviewed literature was then filtered and narrowed down, where a limited number of highly related articles were selected for full article reviewing. Selection criteria were: relevance, regional, and studies categorized as health systems/services research. A committee consisting of 5 senior ophthalmologists from the ophthalmology department met to develop an ophthalmic triage system more reliable than the previously published RESCUE9 (Table 1). Only ophthalmic symptoms and signs that are known to be the presentations of urgent ophthalmic conditions were used for constructing triaging of the patients and getting the total score. Complaints such as tearing and itching were not scored during completion of the triaging form (Table 2). The committee also classified the ophthalmic conditions urgency based on their expertise and ophthalmic literature5,10 (Table 3). Depending on the total score obtained by completing the triage form, patients were divided into 3 categories: a non-urgent ophthalmic condition (total triaging score of 0 or 1), semi-urgent ophthalmic condition (total triaging score of 2 or 3), and urgent ophthalmic condition (total triaging score of 4 or more). Patients with urgent ophthalmic conditions were attended as soon as a vacant space was available in the ophthalmology exam room. An urgent ophthalmic condition was expected to be examined within 45 minutes from registration. Patients with semi-urgent ophthalmic conditions were also seen as soon as there was vacant ophthalmology exam room, but with no patient win the red (urgent) category waiting, if presenting between 8:00 am to 12:00 noon. Patients with non-urgent ophthalmic conditions were not attended to at the OER, and were instructed to seek treatment in the outpatient clinic. The development of the new triage system involved 2 critical phases. In the first phase, which was a prospective cohort study, we validated the modified ophthalmic triage system to determine its safety along with the assurance of the proper training of the nurses. During this phase, no action was taken based on the scores obtained by the new triage system. The triaging was performed to all self-referred patients to study its sensitivity and specificity by testing the association between final diagnosis and total score for each patient during the month of September 2013. The patients’ waiting time before implementing the triaging system was also recorded. Self-referred patients with presenting complaints of 2 weeks or less were included in the triage. By reviewing all the triage files for this period, we found that complaints of more than one week duration were all of the non-urgent category. A decision was then made to change the accepted duration of the presenting complaints in the triage form from 2 weeks to one week. Before implementing the triaging system all self-referred patients were seen. As soon as the patient presented to the OER, the receptionist registered the patient. Screening was then carried out, which involved taking the patient’s visual acuity and intraocular pressure. Following screening, the patient was examined by OER doctor. The second prospective phase started in January 2014, it involved implementing the triage system and evaluating the self-referred patients with complaints of one-week duration or presenting to the OER. The patients were first registered, followed by triaging to determine the category of the ophthalmic condition and the suitability of the patient to be seen at the OER.
Table 1.
Triage of ophthalmic patients presenting to the emergency room without official referral.
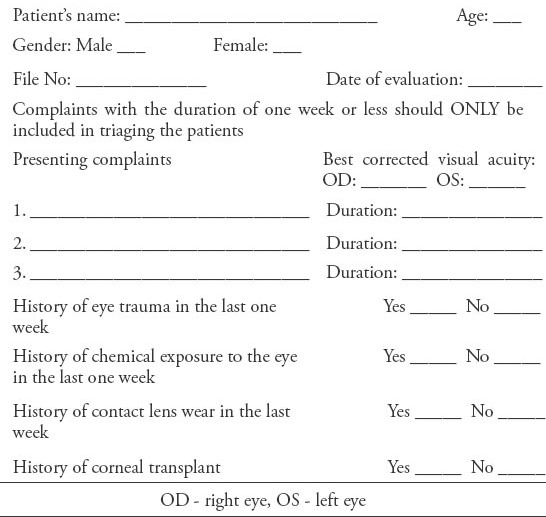
Table 2.
Different categories of clinical findings of emergency ophthalmic patients at presentation and the corresponding score.
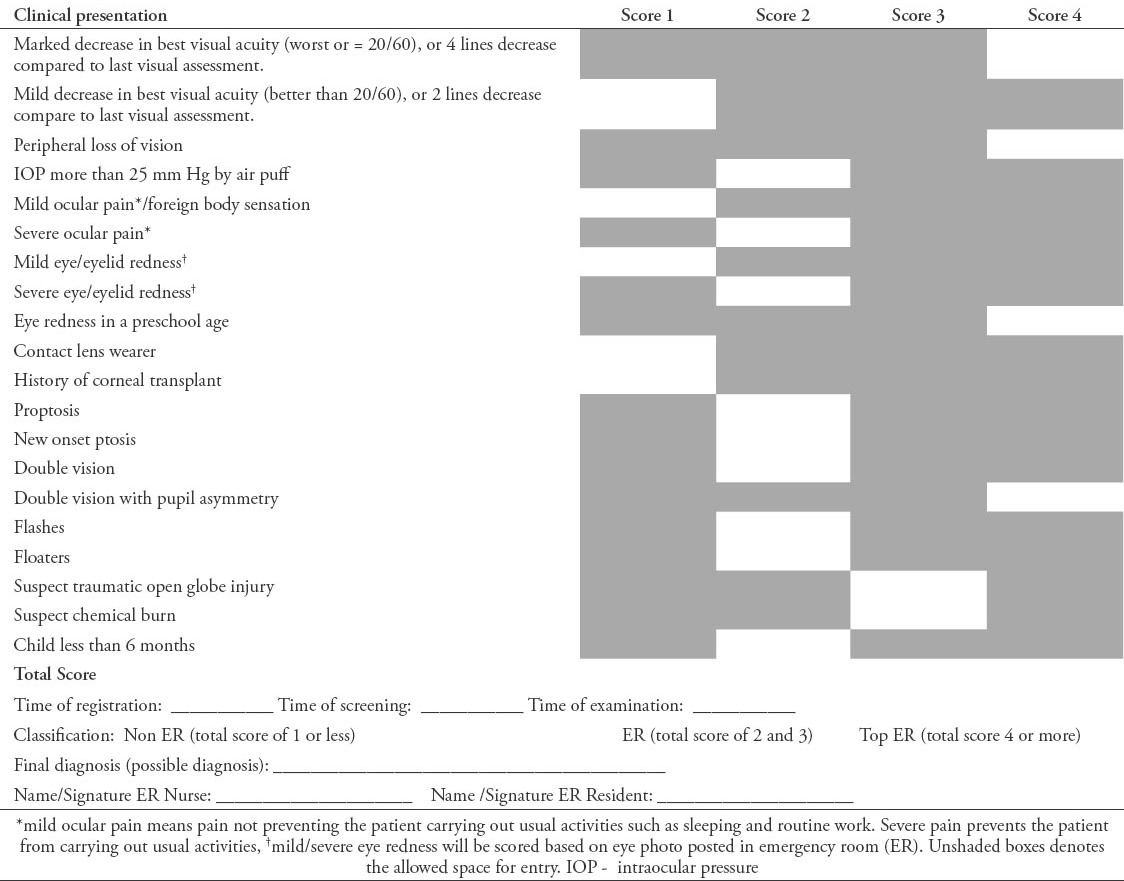
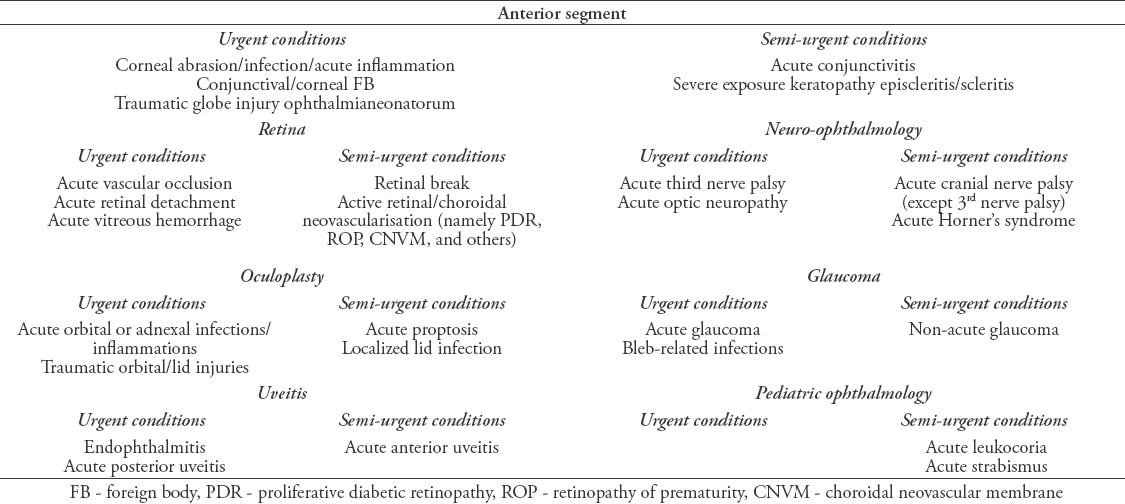
Table 3.
Categories and clinical diagnosis of common ophthalmic conditions presenting to the ophthalmic emergency room.
Data were collected and stored in a spreadsheet using Microsoft Excel 2010® software (Microsoft Corporation, Redmond, WA, USA). Data management and coding were then carried out in excel. Data were analyzed via IBM SPSS Statistics for Windows, version 20.0 (IBM Corp., Armonk, NY, USA). Descriptive statistics were used to describe numerical values and presented in frequency (percentage) for counts, mean and median for continuous variables (times). Mann Whitney U test was used to detect whether the difference in time was statistically significant. Comparison of proportion test was used to compare pre and post intervention proportion of non-urgent ophthalmic conditions.
Results
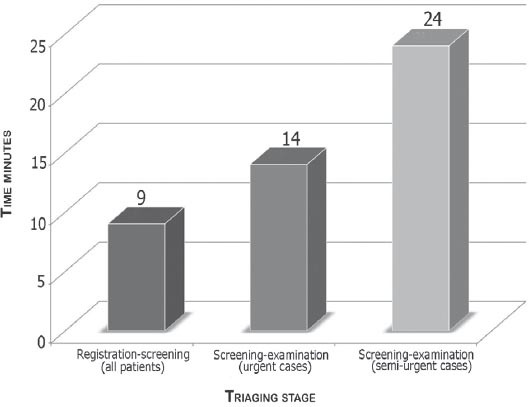
During the month of September, 531 self-referred patients presented to our OER. We went over all the triaging forms filled for the 531 patients and determined the level of the urgency of each patient’s condition according to the diseases’ categories after looking at the final diagnosis given by the OER doctors (Table 3). During this period, 24 (46.5%) patients were found to have non-urgent conditions based on triaging, and all of them were attended as the triaging system was not approved yet. Statistical association between the total score, and the urgency level of each patient’s condition after being examined by the OER doctors was carried out to evaluate the reliability of the triaging system to predict the level of urgency based on the total score. The sensitivity of the triaging system in differentiating urgent and semi-urgent conditions from non-urgent conditions based on the total score obtained by filling the triaging form was 98.7%, and the specificity was 87%. The sensitivity of the triaging system in differentiating urgent conditions from semi-urgent and non-urgent conditions based on the total score obtained by filling the triaging form was 99%, while the specificity for urgent conditions was 90%. The mean waiting time between registration and screening was 22 minutes. The median waiting time between registration and screening was 13 minutes. The mean waiting time between screening and examination was 39.32 minutes. The median waiting time between screening and examination was 25 minutes (Figure 1). The results of evaluating the safety and effectiveness of the modified triage system were very reassuring for the project team and the ophthalmology administration. Data for one month between January and February were collected for post implementation analysis. During this period, 824 self-referred patients were seen at the OER. Out of these 824 patients, 319 (38.7%) patients were found to have non-urgent conditions and were discharged from the OER directly following the triaging. Comparing pre- and post- intervention proportions of non-urgent ophthalmic conditions, the reduction was found to be statistically significant (p=0.005). Following implementation of the triaging system, the mean waiting time between registration and screening including triaging decreased from 22 minutes to 15 minutes (p=0.052). The median waiting time between registration and screening including triaging decreased from 13 minutes to 9 minutes (p=0.090). The mean waiting time between triaging and examination by OER doctors for urgent patients was 29 minutes. The median waiting time between triaging and examination by OER doctors for urgent patients was 14 minutes. The mean waiting time between triaging and examination by OER doctors for semi-urgent patients was 35 minutes. The median waiting time between triaging and examination OER doctors for semi-urgent patients was 24 minutes (Figure 2). Completing the triaging form for each patient took less than 2 minutes.
Figure 1.
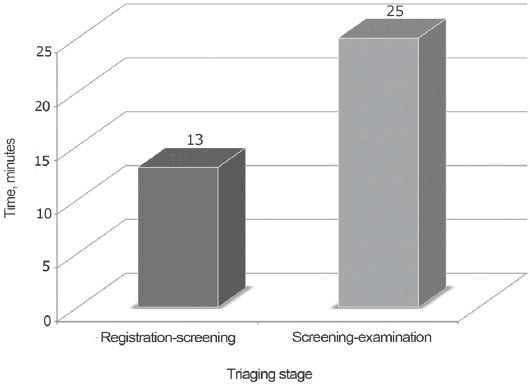
Median time consumed between registration-screening and screening-examination at the pre-triaging stage.
Figure 2.
The median waiting time between triaging and examination for semi-urgent patients.
Discussion
Triaging is an important process in any ER setting. It provides the patients with information regarding their ophthalmic complaints; whether they are urgent or non-urgent, and also how to obtain the appropriate treatment.11,12 This type of service helps the OER staff to identify patients with potentially urgent conditions ahead of time and prioritize them for emergency eye treatment.
Rome Eye Scoring System for Urgency and Emergency can be considered the first structured ophthalmic triaging system that is specifically designed for acute ophthalmic conditions. It was published in 2007 and aimed to triage walk-in patients coming to the OER. This triaging system was based on simple ophthalmic signs and symptoms for accurate and timely identification of the urgency of an ophthalmic condition (Figure 3).9 This system; in fact, showed 90.7% sensitivity, and 97.2% specificity.13 However, a sensitivity of 90.7% indicates considerable chances of missing some patients with some very urgent emergency conditions. The sensitivity of our triage system was 98.7%. This indicates that our system has a better ability to detect urgent and semi-urgent conditions. On the other hand, the specificity of our system was 87% compared with specificity of 97.2% for the previously published one. This indicates that our system has less ability to rule out patients with non-urgent conditions. It was very acceptable for our medical administration to see more patients at the expense of a significant decrease in the chance of missing patients with urgent or semi-urgent condition, as safety is our priority. The sensitivity of our triaging system in separating urgent from semi-urgent or non-urgent conditions was 99%, and the specificity for urgent conditions was 90%. This was found to be very encouraging by the ophthalmology administration. With the demonstrated reliability and safety of our triaging system, we have limited the service of our OER between 12:00 am to 8:00 am to patients with urgent conditions only. This helps the on-call doctor to be undisturbed late at night unless there is a patient with an urgent condition.
Figure 3.

An image of an eye with A) mild redness and B) an eye with severe redness.
A study was carried at our OER in July 2011 on the outcome of ocular emergencies.8 In this study, 1,094 self-referred patients were seen during that month. Out of those 1,094 patients, 712 (65.1%) were found to have non-urgent conditions after they were examined by the OER doctors. The implementation of the modified triaging system helped in decreasing the unnecessary load of patients in our OER. In the month of January 2014, for example, 824 self-referred patients were seen at OER. Out of these patients, 319 (38.7%) patients were discharged immediately after triaging without the need to have them examined by OER doctors after finding them to have non-urgent conditions through the triaging system. Due to the 87% specificity of our triaging system, only 40 patients were found to have non-urgent conditions after examination by OER doctors during the month of January. This huge decrease in the number of non-urgent patients examined by the OER doctors from 712 patients (65% of self-referred patients) in July 2011 to 40 patients (4.8% of self-referred patients) is considered a remarkable achievement of the current organizational development project. Dividing the patients into urgent, semi-urgent, and non-urgent categories is a form of segmentation.14 This change in the OER operation did not lead to delaying the treatment delivery for patients who needed to be treated at OER. The mean waiting time between screening and examination by the OER before the implementation of the triaging system was 39.32 minutes, and this decreased to 29 minutes for urgent conditions, and 35 minutes for semi-urgent conditions after the implementation of the triaging system. More emphasis was given to decreasing the waiting time especially for patients with urgent conditions. This has been carried out by frequent reminders for OER staff on prioritizing urgent conditions and encouraging the OER doctor to spend the least possible time with the patients inside the exam room to facilitate seeing more patients.15
Triaging was an additional part of the screening stage of the patient’s journey in the OER. It was a concern for us that implementing this additional part would increase the waiting time between registration and screening.16 It was an unexpected finding to find that the mean waiting time between registration, and screening after implementing the triaging decreased by 5 minutes. One explanation for this surprising decrease in the mean waiting time between registration and screening after implementing triaging is the increased OER nurses awareness of the importance of the time factor. It was made clear to the nurses that one of the most important objectives of implementing the triaging system is to decrease the patients’ waiting time after implementation.
Currently, the registration time, time between registration, and screening, time between screening and examination by OER doctors, and the time patients are discharged from OER are recorded. Keeping track of waiting times information helps to facilitate the patients’ service and suggest improvement solutions. In this project, there was no discussion on the time between starting to examine the patient and the time the patient is discharged from the OER. This was carried out intentionally due to the huge variability in the time needed to complete the examination by an OER doctor.
The current study faced a number of limitations of which, while adopting the RESCUE; there was a potentiality to miss patients with serous ophthalmic conditions in addition to exclusion of important clinical parameters that are considered as serious indicators for ophthalmic emergency conditions. Moreover, adopting and implantation of a new monitoring system requires a lot of serious efforts to implant this system within the routinely implemented system. Additionally, at both stages, nurses needed repeated awareness sessions and close follow-up to assure quality of time assessment and adequate form completion.
In conclusion, the newly modified ophthalmic triaging system was found to be safe and effective. It may help in prioritizing patients with urgent ophthalmic conditions along with slightly expediting the service for patients with semi-urgent conditions and decreasing the overall waiting time in the OER.
Footnotes
Student Corner.
We invite students from a variety of medical disciplines to submit original contributions based on their supervised research.
The Student Corner of Saudi Med J aims to help students explore research opportunities and network with other peers and mentors in the same field.
Submission Guidelines
Submitted Abstracts should include the following:
Title should be descriptive
Author’s names and affiliation(specify college level/year, academic degree of Senior Author)
Abstract must be structured and not more than 300 words
The following are the typical headings:
Objectives (background, why the study was done, specific aims)
Methods (setting, date of study, design, subjects, intervention and analysis)
Results (findings, data and statistical tests) and
Conclusion (general interpretation of results)
General Information on Abstract Submission
Submitted Abstracts should be co-authored by a Senior Supervisor
Abstracts will be reviewed by Student’s Corner Section Editor
There is no fee to submit an Abstract
Ethical Approval should provided
References
- 1.Gerdtz MF, Collins M, Chu M, Grant A, Tchernomoroff R, Pollard C, et al. Optimizing triage consistency in Australian emergency departments: the Emergency Triage Education Kit. Emerg Med Australas. 2008;20:250–259. doi: 10.1111/j.1742-6723.2008.01089.x. [DOI] [PubMed] [Google Scholar]
- 2.Kadyan A, Sandramouli S, Caruana P. Reorganisation of the ophthalmic casualty in a district teaching hospital. Journal of ESONT. 2007;1:9–15. [Google Scholar]
- 3.Choi YF, Wong TW, Lau CC. Triage rapid initial assessment by doctor (TRIAD) improves waiting time and processing time of the emergency department. Emerg Med J. 2006;23:262–265. doi: 10.1136/emj.2005.025254. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.FitzGerald G, Jelinek GA, Scott D, Gerdtz MF. Emergency department triage revisited. Emerg Med J. 2010;27:86–92. doi: 10.1136/emj.2009.077081. [DOI] [PubMed] [Google Scholar]
- 5.O’Connor PM, Crock CT, Dhillon RS, Keeffe JE. Resources for the management of ocular emergencies in Australia. Emerg Med Australas. 2011;23:331–336. doi: 10.1111/j.1742-6723.2011.01411.x. [DOI] [PubMed] [Google Scholar]
- 6.Bhatt R, Sandramouli S. Evidence-based practice in acute ophthalmology. Eye (Lond) 2007;21:976–983. doi: 10.1038/sj.eye.6702374. [DOI] [PubMed] [Google Scholar]
- 7.Derlet RW, Kinser D, Ray L, Hamilton B, McKenzie J. Prospective identification and triage of nonemergency patients out of an emergency department: a 5-year study. Ann Emerg Med. 1995;25:215–223. doi: 10.1016/s0196-0644(95)70327-6. [DOI] [PubMed] [Google Scholar]
- 8.Alotaibi AG, Osman EA, Allam KH, Abdel-Rahim AM, Abu-Amero KK. One month outcome of ocular related emergencies in a tertiary hospital in Central Saudi Arabia. Saudi Med J. 2011;32:1256–1260. [PubMed] [Google Scholar]
- 9.Rossi T, Boccassini B, Iossa M, Mutolo MG, Lesnoni G, Mutolo PA. Triaging and coding ophthalmic emergency: the Rome Eye Scoring System for Urgency and Emergency (RESCUE):a pilot study of 1,000 eye-dedicated emergency room patients. Eur J Ophthalmol. 2007;17:413–417. doi: 10.1177/112067210701700324. [DOI] [PubMed] [Google Scholar]
- 10.Hau S, Ioannidis A, Masaoutis P, Verma S. Patterns of ophthalmological complaints presenting to a dedicated ophthalmic Accident & Emergency department: inappropriate use and patients’ perspective. Emerg Med J. 2008;25:740–744. doi: 10.1136/emj.2007.057604. [DOI] [PubMed] [Google Scholar]
- 11.Marsden J. An evaluation of the safety and effectiveness of telephone triage as a method of patient prioritization in an ophthalmic accident and emergency service. J Adv Nurs. 2000;31:401–409. doi: 10.1046/j.1365-2648.2000.01285.x. [DOI] [PubMed] [Google Scholar]
- 12.Smith HB, Daniel CS, Verma S. Eye casualty services in London. Eye (Lond) 2013;27:320–328. doi: 10.1038/eye.2012.297. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Rossi T, Boccassini B, Cedrone C, Iossa M, Mutolo MG, Lesnoni G, et al. Testing the reliability of an eye-dedicated triaging system: the RESCUE. Eur J Ophthalmol. 2008;18:445–449. doi: 10.1177/112067210801800321. [DOI] [PubMed] [Google Scholar]
- 14.Silvester K, Lendon R, Bevan H, Steyn R, Walley P. Reducing waiting times in the NHS: is lack of capacity the problem? Clinician in Management. 2004;12:105–111. [Google Scholar]
- 15.Raynaud L, Borne M, Coste S, Daban JL, Tourtier JP. Triage protocol: both undertriage and overtriage need to be evaluated. J Trauma. 2010;69:998. doi: 10.1097/TA.0b013e3181ec4e1d. [DOI] [PubMed] [Google Scholar]
- 16.Eriksson H, Bergbrant IM, Berrum I, Morck B. Reducing queues: demand and capacity variations. Int J Health Care Qual Assur. 2011;24:592–600. doi: 10.1108/09526861111174161. [DOI] [PubMed] [Google Scholar]