

Abstract
Objectives:
To determine the prevalence of hyperlipidemia in patients from Saudi Arabia with rheumatoid arthritis (RA), and to investigate its relationship with C-reactive protein level and disease activity.
Methods:
A cross-sectional 3-year study was conducted on RA patients at King Abdulaziz University Hospital, Saudi Arabia between January 2011 and December 2013. Lipid profiles were determined following 12-hour overnight fasting, and the association of lipid profiles with C-reactive protein (CRP) levels and disease activity was determined.
Results:
This study involved a total of 180 RA patients (mean age: 40.49±12.19 years). These subjects displayed a high prevalence of elevated total cholesterol (55.1%), and low-density lipoprotein cholesterol (51.2%). Notably, we detected a significant association between increased total cholesterol and high CRP levels (p=0.002). Moreover, we observed a positive correlation between total cholesterol and disease activity, as measured using the 28-Joint Disease Activity Score index (r=0.23, p=0.036).
Conclusions:
Hyperlipidemia is common among RA patients and is significantly associated with CRP levels and disease activity. Our findings emphasize the need to raise awareness among healthcare professionals regarding the development of hyperlipidemia when RA is active.
Rheumatoid arthritis (RA) is a chronic inflammatory disorder that typically affects middle-aged individuals. The estimated prevalence of RA in Saudi Arabia is 2.2 per thousand people; it is more common in women, and incidence increases with age.1 If left untreated, RA is associated with high morbidity and mortality, which specifically results from cardiovascular disease (CVD).2,3 In order to reduce the CVD-related mortality rate in RA patients, the European League Against Rheumatism (EULAR) has recommended annual risk assessment, management of identified risk factors, and aggressive suppression of inflammation.4-6 In this regard, it has been demonstrated that treating RA with disease-modifying anti-rheumatic drugs (DMARDs) can effectively reduce CVD-related mortality.4,7 Cardiovascular disease is not only linked to traditional risk factors as hyperlipidemia, but also to nontraditional risk factors including chronic systemic inflammation. Notably, changes in lipid profiles have been established as traditional cardiovascular (CV) risk factors, but also as non-traditional that is directly linked to active inflammation (namely, disease activity).8-11 In fact, studies on CVD in RA patients have indicated that chronic systemic inflammation can enhance the development of atherosclerosis and hyperlipidemia.12,13 In this regard, the prevalence of hyperlipidemia in RA patients is known to vary between 20-45%.14,15 Hyperlipidemia in RA patients in Saudi Arabia has not been thoroughly investigated to date. Therefore, the objective of the present study was to estimate the prevalence of hyperlipidemia in RA patients in Saudi Arabia, and to identify possible associated risk factors, including inflammatory markers.
Methods
Patients and study design
This cross-sectional study was performed in a tertiary care setting at a teaching center in the Western region of Saudi Arabia between January 2011 to December 2013. The research was approved by the local biomedical ethics committee (Faculty of Medicine, King Abdulaziz University [KAU], Jeddah, Saudi Arabia), and informed consent was obtained from all subjects prior to their consecutive enrollment. The study was conducted in accordance with the Declaration of Helsinki.
The sample size was calculated based on the hypothesis that the prevalence of the case happening between 20-40% in a population of 271 RA patients with a maximum margin of error of 5% within 95% confidence interval. It was calculated using MedCalc statistical software, available at www.medcalc.com. Initially it comprised 160 patients. The size was increased by 15% to a total of 180 patients, to account for non-respondents.
Rheumatoid arthritis was assessed based on the 2010 American College of Rheumatology (ACR)/European League Against Rheumatism (EULAR) classification.16 Patients with the following characteristics were excluded: diabetes mellitus, hypertension, post-menopausal, body mass index (BMI) >30 (namely, obesity), hypothyroidism, chronic steroid use, patients with extra-articular manifestation, active/severe infection, or hyperlipidemia treated with a lipid lowering therapy. Hyperlipidemia was defined based on the Expert Panel Third Report Classification on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel-ATPIII),15 which recommends the following respective cut-offs for high total cholesterol (TC), triglycerides (TG), high-density lipoprotein (HDL), and low-density lipoprotein (LDL): ≥240 mg/dL, ≥200 mg/dL, ≥60 mg/dL, and ≥160 mg/dL.
The following patient data was collected and recorded by the physician upon follow-up: age, gender, nationality, disease duration (years), and current medication use (DMARDs and biologics). Also, the following laboratory data was collected following 12-hour overnight fasting: TC, TG, HDL, and LDL levels (all mmol/L). In addition, immunoglobulin M (IgM) rheumatoid factor (RF), and C-reactive protein (CRP) levels were measured. Furthermore, disease activity in RA patients was measured using the 28-Joint Disease Activity Score index (DAS28) based on CRP levels.16
Statistical analysis
Statistics were used to summarize frequency distributions and simple descriptive values. Continuous data are presented as means with standard deviations (SD), whereas categorical variables are shown as percentages. Independent t-tests were used to assess mean significant differences, and the chi-square test was employed to evaluate relationships between categorical variables. In addition, 2-tailed Pearson’s correlation was used to investigate the relationship between TC levels and DAS28–CRP. All data analyses were performed using IBM SPSS Statistics for Windows version 20, (IBM Corp., Armonk, New York, USA). P-values <0.05 were considered to be statistically significant.
Results
Patient characteristics
Characteristics of the study population are summarized in Tables 1 & 2. A total of 180 patients were included. Among these patients, most were female, and over half of the subjects were Saudi. The mean age of the cohort was 40.49 ± 12.19 years, and the mean RA disease duration was 5.51 ± 5.78 years. Approximately two-thirds of the population was RF positive, and over 75% of the patients displayed high CRP values. In addition, a significant proportion of patients were treated with DMARDs in our cohort, whereas only a quarter of the subjects were given biologic therapies. Finally, over half of these RA patients were found to present with elevated TC.
Table 1.
Baseline patient characteristics among 180 RA patients.
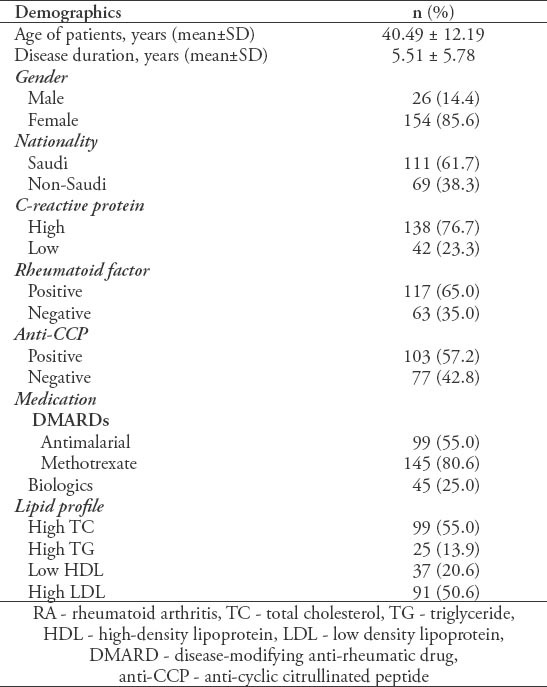
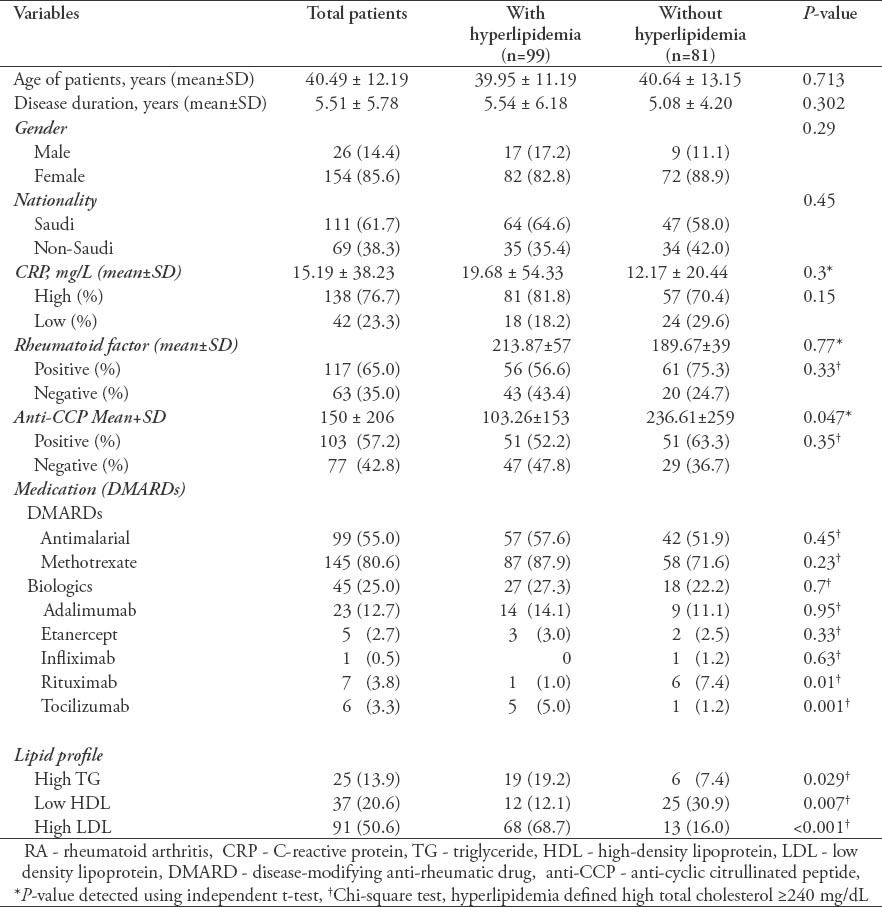
Table 2.
Comparison of baseline characteristics according to hyperlipidemia in 180 RA patients.
Hyperlipidemia in RA patients
We analyzed the relationship between high TC and various co-variables in our study population. Based on independent t-tests, we found that TC was significantly associated with TG (p=0.005), low HDL (p=0.034), and high LDL (p=0.001). In addition, chi-square tests revealed that high TC was significantly associated with high TG (p=0.029) and high LDL (p<0.001), whereas the relationship between high TC and low HDL was not significant (p=0.077).
Furthermore, we examined whether lipid levels correlated with RA activity in our cohort. Indeed, we found that high TC and LDL were significantly associated with elevated CRP (p=0.002). Strikingly, 81.2% of the patients with high TC and LDL also displayed elevated CRP levels (Figure 1). In addition, we found a statistically significant positive correlation between DAS28 and TC levels (r=0.23, p=0.036), indicating that the TC levels increased with higher disease activity in our patients. There was a significant negative correlation between TC levels and Anti-CCP level (r -0.32, p=0.41). No other significant relationships were observed between hyperlipidemia and the characteristics of our study population as well no significant correlation between HDL, LDL, TG with DAS28 or between TC and RF levels.
Figure 1.
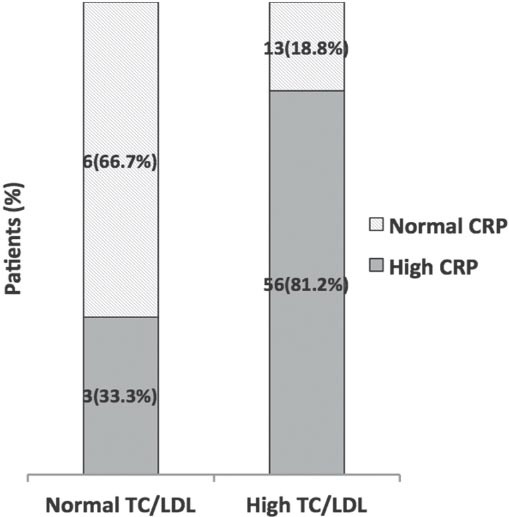
Relationship of C-reactive protein (CRP) levels with total cholesterol (TC) and low density lipoprotein (LDL).
Discussion
We conducted a cross-sectional study to examine hyperlipidemia in patients with RA in Saudi Arabia. There is a scarcity of previous investigation into the relationship between hyperlipidemia and RA in a cohort from Saudi Arabia. Our findings indicate that a large proportion of RA patients displayed high TC and LDL, which were significantly associated with elevated CRP levels and disease activity.
Prevalence of hyperlipidemia in RA patients
According to cutoff values recommended by the National Cholesterol Education Program (NCEP) guidelines,17 our findings indicate that hyperlipidemia is highly prevalent in patients with RA in Saudi Arabia. Indeed, our observed prevalence was slightly higher than that reported in a UK study (42%),14 and much greater than reports in the USA (18%),15 and France (24%).12 Furthermore, we found that the mean TC serum level in our RA cohort was comparable to that previously described for patients in the absence of lipid-lowering medications.19 Considering our findings in the context of a report by Al-Kaabba et al,20 which used the same cutoff values employed in the current study in order to establish a hyperlipidemia rate of 20-40% in the general Saudi Arabian population, it seems that our observed rate of 55% may indicate that hyperlipidemia is becoming a more prevalent health problem in Saudi Arabia, and perhaps particularly for RA patients.20
Effect of hyperlipidemia in RA patients
To date, data regarding TC and LDL levels in RA patients have been conflicting, with reports indicating increased,21 decreased,22 or similar6,23 levels compared with controls. Despite the TC changes that may occur in RA patients, it is known that treating hyperlipidemia in these individuals can decrease CV events and all-cause mortality (adjusted hazard ratios: 0.45 [95% confidence intervals [CI]: 0.20-0.98] and 0.43 [95% CI: 0.20–0.92]).24 In addition, it has been reported that untreated hyperlipidemia can increase the risk of abnormal liver function tests secondary to methotrexate therapy.25 Furthermore, hyperlipidemia might accelerate radiological progression in RA patients. In this regard, Park et al26 recently demonstrated that the risk of radiographic progression was 5.6-fold higher in RA patients displaying plasma LDL cholesterol and TG levels within the third tertile.
Regarding HDL-cholesterol, it has been reported that patients with active RA consistently demonstrate reduced levels.27 Nevertheless, in the present study, only 12.1% of patients with hyperlipidemia were observed to have low HDL. Moreover, HDL levels were not found to be associated with disease activity. We did not detect any association between hyperlipidemia and RF or anti-CCP levels that have been previously demonstrated.10,11 this could be explained by several factors including: sample size (despite it was calculated), hetrogenicity of the studied group, polyautoimmunity, familial autoimmunity, and smoking.
Association of hyperlipidemia with CRP levels and disease activity
There have been limited reports on the association of lipid levels with disease activity in RA patients. While some investigations have demonstrated a relationship between lipid profiles and disease activity, others have not.7 However, most studies considering CRP levels have indicated an association of lipid levels with CRP.26 Nevertheless, it is important to note that CRP levels do not always correlate with disease activity. In fact, a recent US registry study,28 which included more than 9,000 RA patients, observed discordance between clinical disease activity indexes and acute phase reactants, such as CRP. That being said, emerging evidence also suggests that the chronic inflammatory state that exists in RA patients can contribute to CV morbidity.7,29,30 Thus, our observed relationship between hyperlipidemia and CRP levels might explain the increased CVD risk in RA patients, which could stem from the role of inflammatory factors in driving the development of atherosclerosis.29 Our correlation analysis suggested that TC levels increased with higher disease activity and elevated CRP, a finding that has been previously documented in other populations.7,24,30 Therefore, identifying high CRP levels and DAS28 through monitoring may indicate a need for evaluation of hyperlipidemia risk in RA patients. Future clinical studies assessing the efficacy of using CRP levels and DAS28 to identify hyperlipidemia in a large cohort of RA patients are warranted and could lead to improved patient care. Furthermore, investigations are needed to assess how diverse treatments might impact accelerated atherosclerosis in rheumatic diseases.33
Traditional and non-traditional risk factors for CV diseases in RA patients
CVD carries high frequency in RA patients due to either traditional (i.e., dyslipidemia, abnormal BMI, male) and Novel non-traditional risk factors (which are divided into genetic factors, RA related factors including, familial autoimmunity, RF positivity, Anti-CCP, chronic proinflammatory state, high disease activity, duration of the disease more than 10 years, extraarticular manifestation, steroids treatment and finally other variable).34 Solomon et al,35 showed that the relative risk (RR) of Myocardial infarction in women with rheumatoid arthritis compared with those without was 2.0 (95% confidence interval [CI], 1.23 to 3.29), and the longer the disease duration defined >10 years the higher the risk, RR= 3.10 (95% CI, 1.64 to 5.87). In our study we tried to exclude risk factors other than disease activity and chronic inflammation.
Possible role of dyslipidemia in new assessment tools for cardiovascular risk in RA
The notion that RA represents an indication for lipid testing has recently gained momentum. Indeed, the American Heart Association and the Canadian Cardiovascular Society Guidelines for prevention of CVD have listed RA as a major risk factor for which lipid testing is recommended.36,37 In addition, the EULAR recommendation on estimating the CVD risk in RA patients have been published but not validated and it includes lipid testing. However, optimal intervals and therapeutic goals related to such testing in RA patients remain to be determined. While it is well known that RA is associated with a 2-fold increase in CVD compared to control patients, to the best of our knowledge, the risk of CVD in RA patients with hyperlipidemia has not been defined [37]. In addition, neither the Framingham Risk Score nor the Reynold’s Score were designed to estimate risk in RA patients. Thus, a large-scale study is warranted to analyze CVD risk over time in our population of RA patients with hyperlipidemia.
Study limitations
This study presented several limitations. Indeed, the size of our cohort may not have been sufficient for drawing definitive conclusions regarding hyperlipidemia in RA patients. Thus, although our findings were shown to be statistically significant, studies in a larger Saudi population may be needed to confirm these results. Multivariate analysis of the data may also add weight to the results. Also, the fact that this study was conducted at a single center in Saudi Arabia may have introduced bias. Moreover, we have not included a comparison of RA and non-RA patients in the present study. It would also be interesting to investigate the variation in DAS28, CRP, and lipids over time.
In conclusion, hyperlipidemia is common in RA patients in Saudi Arabia. Our findings emphasize the need to raise awareness among healthcare professionals regarding the development of hyperlipidemia in RA patients. Screening for hyperlipidemia may be particularly important in patients with active RA or persistently high inflammatory markers to prevent CVD-related morbidity and mortality.
Footnotes
Related Articles.
Safi MA, Fathaldin OA. Pattern of drugs use and association with anti-mutated citrullinated vimentin antibody in rheumatoid arthritis. Saudi Med J 2015; 36: 316-323.
Almoallim HM, Alharbi LA. Rheumatoid arthritis in Saudi Arabia. Saudi Med J 2014; 35: 1442-1454.
Janoudi N, Almoallim H, Husien W, Noorwali A, Ibrahim A. Work ability and work disability evaluation in Saudi patients with rheumatoid arthritis. Special emphasis on work ability among housewives. Saudi Med J 2013; 34: 1167-1172.
References
- 1.Al-Dalaan A, Al Ballaa S, Bahabri S, Biyari T, Al Sukait M, Mousa M. The prevalence of rheumatoid arthritis in the Qassim region of Saudi Arabia. Ann Saudi Med. 1998;18:396–397. doi: 10.5144/0256-4947.1998.396. [DOI] [PubMed] [Google Scholar]
- 2.del Rincón ID, Williams K, Stern MP, Freeman GL, Escalante A. High incidence of cardiovascular events in a rheumatoid arthritis cohort not explained by traditional cardiac risk factors. Arthritis Rheum. 2001;44:2737–2745. doi: 10.1002/1529-0131(200112)44:12<2737::AID-ART460>3.0.CO;2-%23. [DOI] [PubMed] [Google Scholar]
- 3.Snow MH, Mikuls TR. Rheumatoid arthritis and cardiovascular disease: the role of systemic inflammation and evolving strategies of prevention. Curr Opin Rheumatol. 2005;17:234–241. doi: 10.1097/01.bor.0000159924.97019.25. [DOI] [PubMed] [Google Scholar]
- 4.Bartels CM, Kind AJ, Thorpe CT, Everett CM, Cook RJ, McBride PE, et al. Lipid testing in patients with rheumatoid arthritis and key cardiovascular-related comorbidities: a medicare analysis. Semin Arthritis Rheum. 2012;42:9–16. doi: 10.1016/j.semarthrit.2012.01.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Peters MJ, Symmons DP, McCarey D, Dijkmans BA, Nicola P, Kvien TK, et al. EULAR evidence-based recommendations for cardiovascular risk management in patients with rheumatoid arthritis and other forms of inflammatory arthritis. Ann Rheum Dis. 2010;69:325–331. doi: 10.1136/ard.2009.113696. [DOI] [PubMed] [Google Scholar]
- 6.Park YB, Choi HK, Kim MY, Lee WK, Song J, Kim DK, et al. Effects of antirheumatic therapy on serum lipid levels in patients with rheumatoid arthritis: a prospective study. Am J Med. 2002;113:188–193. doi: 10.1016/s0002-9343(02)01186-5. [DOI] [PubMed] [Google Scholar]
- 7.Choy E, Sattar N. Interpreting lipid levels in the context of high-grade inflammatory states with a focus on rheumatoid arthritis: a challenge to conventional cardiovascular risk actions. Ann Rheum Dis. 2009;68:460–469. doi: 10.1136/ard.2008.101964. [DOI] [PubMed] [Google Scholar]
- 8.Myasoedova E, Crowson CS, Kremers HM, Roger VL, Fitz-Gibbon PD, Therneau TM, et al. Lipid paradox in rheumatoid arthritis: the impact of serum lipid measures and systemic inflammation on the risk of cardiovascular disease. Ann Rheum Dis. 2011;70:482–487. doi: 10.1136/ard.2010.135871. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Maradit-Kremers H, Nicola PJ, Crowson CS, Ballman KV, Gabriel SE. Cardiovascular death in rheumatoid arthritis: a population-based study. Arthritis Rheum. 2005;52:722–732. doi: 10.1002/art.20878. [DOI] [PubMed] [Google Scholar]
- 10.Amaya-Amaya J, Sarmiento-Monroy JC, Mantilla RD, Pineda-Tamayo R, Rojas-Villarraga A, Anaya JM. Novel risk factors for cardiovascular disease in rheumatoid arthritis. Immunol Res. 2013;56:267–286. doi: 10.1007/s12026-013-8398-7. [DOI] [PubMed] [Google Scholar]
- 11.Amaya-Amaya J, Montoya-Sánchez L, Rojas-Villarraga A. Cardiovascular involvement in autoimmune diseases. Biomed Res Int 2014. 2014:367359. doi: 10.1155/2014/367359. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Scott IC, Ibrahim F, Johnson D, Scott DL, Kingsley GH. Current limitations in the management of cardiovascular risk in rheumatoid arthritis. Clin Exp Rheumatol. 2012;30:228–232. [PubMed] [Google Scholar]
- 13.del Rincón I, Escalante A. Atherosclerotic cardiovascular disease in rheumatoid arthritis. Curr Rheumatol Rep. 2003;5:278–286. doi: 10.1007/s11926-003-0006-8. [DOI] [PubMed] [Google Scholar]
- 14.Soubrier M, Zerkak D, Dougados M. Indications for lowering LDL cholesterol in rheumatoid arthritis: an unrecognized problem. J Rheumatol. 2006;33:1766–1769. [PubMed] [Google Scholar]
- 15.Willerson JT, Ridker PM. Inflammation as a cardiovascular risk factor. Circulation. 2004;109(21 Suppl 1):II2–II10. doi: 10.1161/01.CIR.0000129535.04194.38. [DOI] [PubMed] [Google Scholar]
- 16.Neogi T, Aletaha D, Silman AJ, Naden RL, Felson DT, Aggarwal R, et al. The 2010 American College of Rheumatology/European League Against Rheumatism classification criteria for rheumatoid arthritis: Phase 2 methodological report. Arthritis Rheum. 2010;62:2582–2591. doi: 10.1002/art.27580. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation. 2002;106:3143–3421. [PubMed] [Google Scholar]
- 18.Aletaha D, Ward MM, Machold KP, Nell VP, Stamm T, Smolen JS. Remission and active disease in rheumatoid arthritis: defining criteria for disease activity states. Arthritis Rheum. 2005;52:2625–2636. doi: 10.1002/art.21235. [DOI] [PubMed] [Google Scholar]
- 19.McCarey DW, McInnes IB, Madhok R, Hampson R, Scherbakov O, Ford I, et al. Trial of Atorvastatin Rheumatoid Arthritis (TARA):double-blind, randomized placebo-controlled trial. Lancet. 2004;363:2015–2021. doi: 10.1016/S0140-6736(04)16449-0. [DOI] [PubMed] [Google Scholar]
- 20.Al-Kaabba AF, Al-Hamdan NA, El Tahir A, Abdalla AM, Saeed AA, Hamza MA. Prevalence and correlates of dyslipidemia among adults in Saudi Arabia: results from a national survey. Open J Endocr Metab Dis. 2012;2:89–97. [Google Scholar]
- 21.Georgiadis AN, Papavasiliou EC, Lourida ES, Alamanos Y, Kostara C, Tselepis AD, et al. Atherogenic lipid profile is a feature characteristic of patients with early rheumatoid arthritis: effect of early treatment--a prospective, controlled study. Arthritis Res Ther. 2006;8:R82. doi: 10.1186/ar1952. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Boers M, Nurmohamed MT, Doelman CJ, Lard LR, Verhoeven AC, Voskuyl AE, et al. Influence of glucocorticoids and disease activity on total and high density lipoprotein cholesterol in patients with rheumatoid arthritis. Ann Rheum Dis. 2003;62:842–845. doi: 10.1136/ard.62.9.842. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Chung CP, Giles JT, Petri M, Szklo M, Post W, Blumenthal RS, et al. Prevalence of traditional modifiable cardiovascular risk factors in patients with rheumatoid arthritis: comparison with control subjects from the multi-ethnic study of atherosclerosis. Semin Arthritis Rheum. 2012;41:535–544. doi: 10.1016/j.semarthrit.2011.07.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Sheng X, Murphy MJ, Macdonald TM, Wei L. Effectiveness of statins on total cholesterol and cardiovascular disease and all-cause mortality in osteoarthritis and rheumatoid arthritis. J Rheumatol. 2012;39:32–40. doi: 10.3899/jrheum.110318. [DOI] [PubMed] [Google Scholar]
- 25.Kent PD, Luthra HS, Michet C., Jr Risk factors for methotrexate-induced abnormal laboratory monitoring results in patients with rheumatoid arthritis. J Rheumatol. 2004;31:1727–1731. [PubMed] [Google Scholar]
- 26.Park YJ, Cho CS, Emery P, Kim WU. LDL cholesterolemia as a novel risk factor for radiographic progression of rheumatoid arthritis: a single-center prospective study. PLoS One. 2013;8:e68975. doi: 10.1371/journal.pone.0068975. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Dursunoğlu D, Evrengül H, Polat B, Tanriverdi H, Cobankara V, Kaftan A, et al. Lp(a) lipoprotein and lipids in patients with rheumatoid arthritis: serum levels and relationship to inflammation. Rheumatol Int. 2005;25:241–245. doi: 10.1007/s00296-004-0438-0. [DOI] [PubMed] [Google Scholar]
- 28.Kay J, Morgacheva O, Messing SP, Kremer JM, Greenberg JD, Reed GW, et al. Clinical disease activity and acute phase reactant levels are discordant among patients with active rheumatoid arthritis: acute phase reactant levels contribute separately to predicting outcome at one year. Arthritis Res Ther. 2014;16:R40. doi: 10.1186/ar4469. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Libby P, Ridker PM. Inflammation and atherosclerosis: role of C-reactive protein in risk assessment. Am J Med. 2004;116(Suppl 6A):9S–16S. doi: 10.1016/j.amjmed.2004.02.006. [DOI] [PubMed] [Google Scholar]
- 30.Maradit-Kremers H, Nicola PJ, Crowson CS, Ballman KV, Gabriel SE. Cardiovascular death in rheumatoid arthritis: a population-based study. Arthritis Rheum. 2005;52:722–732. doi: 10.1002/art.20878. [DOI] [PubMed] [Google Scholar]
- 31.Ku IA, Imboden JB, Hsue PY, Ganz P. Rheumatoid arthritis: model of systemic inflammation driving atherosclerosis. Circ J. 2009;73:977–985. doi: 10.1253/circj.cj-09-0274. [DOI] [PubMed] [Google Scholar]
- 32.Yoo WH. Dyslipoproteinemia in patients with active rheumatoid arthritis: effects of disease activity, sex, and menopausal status on lipid profiles. J Rheumatol. 2004;31:1746–1753. [PubMed] [Google Scholar]
- 33.Gasparyan AY, Stavropoulos-Kalinoglou A, Mikhailidis DP, Toms TE, Douglas KM, Kitas GD. The rationale for comparative studies of accelerated atherosclerosis in rheumatic diseases. Curr Vasc Pharmacol 201. doi: 10.2174/157016110791330852. [DOI] [PubMed] [Google Scholar]
- 34.Sarmiento-Monroy JC, Amaya-Amaya J, Espinosa-Serna JS, Herrera-Diaz C, Anaya JM, Rojas-Villarraga A. Cardiovascular diseases in rheumatoid arthritis : a systematic literature review in Latin Americans. Arthritis 2012. 2012:371909. doi: 10.1155/2012/371909. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Solomon DH, Kremer J, Curtis JR, Hochberg MC, Reed G, Tsao P, et al. Explaining the cardiovascular risk associated with rheumatoid arthritis: traditional risk factors versus markers of rheumatoid arthritis severity. Ann Rheum Dis. 2010;69:1920–1925. doi: 10.1136/ard.2009.122226. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Mosca L, Benjamin EJ, Berra K, Bezanson JL, Dolor RJ, Lloyd-Jones DM, et al. Effectiveness based guidelines for the prevention of cardiovascular disease in women--2011 update: a guideline from the American Heart Association. J Am Coll Cardiol. 2011;57:1404–1423. doi: 10.1016/j.jacc.2011.02.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Genest J, McPherson R, Frohlich J, Anderson T, Campbell N, Carpentier A, et al. 2009 Canadian Cardiovascular Society/Canadian guidelines for the diagnosis and treatment of dyslipidemia and prevention of cardiovascular disease in the adult--2009 recommendations. Can J Cardiol. 2009;25:567–579. doi: 10.1016/s0828-282x(09)70715-9. [DOI] [PMC free article] [PubMed] [Google Scholar]