

The Kingdom of Saudi Arabia (KSA), is one of the largest Middle Eastern countries with a landmass of 2.5 million square kilometers, and has transformed over 50 years to the most urbanized country in the region. With an estimated population of almost 30 million residents with an annual growth rate of 2.7%,1 the Saudi Arabian healthcare sector caters to a rapidly growing population and the concurrent increasing demand on the healthcare sector.
Healthcare services in the KSA receive much attention from its leadership. Such services are considered top priority. It has undergone considerable development brought about by means of the successive development plans, where the Ministry of Health (MOH) has a crucial role to play. According to the World Health Organization, the Saudi health care system is ranked 26th among 190 of the world’s health care systems.2 The purpose of this brief report is to provide some insights into the current status of critical care practice in Saudi Arabia, including major challenges like, intensive care unit (ICU) standard level, cost, education, training, research activities, and Saudi critical care experience during Hajj. In the year 2012, the cumulative budget allocation for the MOH was around 54 billion (6.6% from the total government budget) Saudi Riyals (SAR) compared to around 25 billion (5.6%) SAR in year 2008.1 This was reflected on the total number of hospitals throughout the kingdom. The Ministry’s strategy has placed particular emphasis on expanding the critical care services and promoted the accessibility and feasibility of the critical care services. In order to improve the health care and to invest in citizens, the MOH has embraced several projects and redirected the necessary funds for these programs, such as establishing and developing of a new general hospitals, medical cities, and specialist hospitals. These projects aim to cover the whole land of KSA, and to deliver health care, including critical care services to all Saudi citizens and expatriates working in public sectors, free of charge to all.3
There is an increasing demand for critical care services in KSA and globally, this demand is attributable to the increasing population age, longer survival of previously incurable diseases, and advanced surgical procedure that makes post-operative intensive care admission mandatory. Many patients who required such treatment in the past, had to go abroad, while it becomes possible now to provide such advanced medical treatments locally. The improvement in critical care medicine itself has made it possible to improve or prolong survival of certain diseases leading to longer ICU stay and increasing demand for critical care services and support. The return of highly qualified physicians and surgeons after completion of their postgraduate training in an international academic medical centers lead to the introduction of new treatment modalities, such as bone marrow and liver transplantation and radical cancer surgeries. Such therapies and surgeries typically require intensive care. Factors like worldwide growth in the critical care specialty and the national introduction of advanced medical therapies were other reasons behind the recently witnessed major developments in critical care medicine in KSA.
The MOH provides health services at primary, secondary, and tertiary hospitals. Three different levels of critical care are provided by these hospitals (Tables 1 & 2). Cases that need more complex levels of care are transferred to specialized hospitals (the tertiary level of health care).4 The Saudi Critical Care Society (SCCS) is a premier critical care society in the Middle East with its largest and most expansive education programs focused on serving the critical care community in KSA (both adult and neonatal). The organization helps in the development of the critical care sector and disseminates quality information and knowledge among all its members, and professionals associated with the industry. The SCCS has a long and distinguished history of staffing critical care units during Hajj, training staff at MOH hospitals, and training generation after generation of critical care managers through association with the Saudi Healthcare Leadership Institute. In addition, the society has special relationships with the Society of Critical Care Medicine, the European Society of Intensive Care Medicine, and many regional societies. By this means, it is proud to bring world-class leaders in critical care medicine to KSA through joint conferences with both societies.
Table 1.
Different levels of critical care provided in Saudi hospitals.
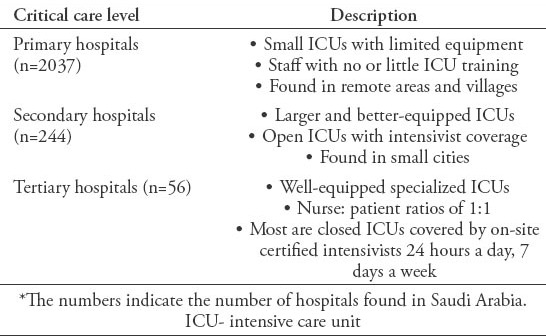
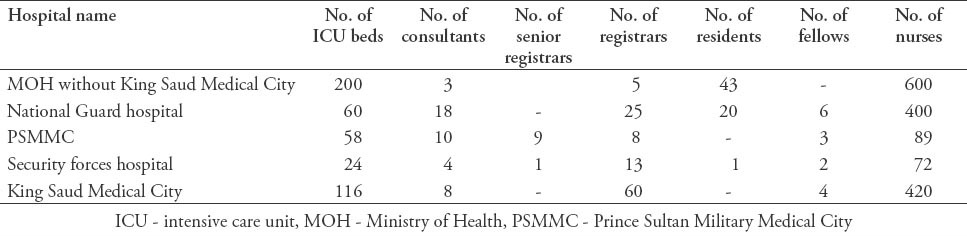
Table 2.
The number of Riyadh hospital ICU beds, intensivist, and nurses.
Over the past 20 years, research activity has been developing slowly in Saudi Arabia, especially in critical care areas. But, research activities are still lagging behind the international level. The etiology is multifactorial. First, lack of research funds, which seem to be a worldwide problem as in the United States the research funding for critical care represents between 1.7% and 6.3% of the federal research budget.5 Second, the absence of good databases in most of Saudi Arabia ICUs. Third, inadequate statistics, fourth limited training and expertise in the area of research and last, poor ethical practice due to social and cultural misunderstanding of the research concept. In a survey carried out by Al-Dorzi et al,6 ICU staff reported that the main barriers against participation in research were lack of time, lack of financial compensation, and lack of encouragement. Despite the previous limiting factors, there has been some good work from individual centers with very good results either as local publications,7-9 or participating in international projects.10 To improve the quality and quantity of research in Saudi Arabian critical care, we should create an increased pool of trained researchers, providing more funds, working on more national and regional projects, supporting research training as part of the science curriculum at the undergraduate and graduate level. Planned annual large gatherings, and events pose a huge logistic challenge in providing medical care, especially critical care. Kingdom of Saudi Arabia’s responsibility for the Hajj has affected the country’s advanced healthcare infrastructure. Within the immediate vicinity of the Hajj, there are more than 130 centers equipped with the latest emergency management medical systems. Thirty percent of the bed capacity in these centers is equipped to provide state of the art critical care service, all at no charge. As one Hajj ends, planning for the next begins, all with better quality of service than the previous year.11
Knowledge of critical illness during Hajj is an essential tool to help understand and therefore prepare for such events. It helped the critical care professional body avoid mismatched “illness demand-care capacity”. In a prospective cohort study of the critically ill patients in 2009 Hajj in KSA, 110 patients needed ICU admission due to various reasons. They had a mean Acute Physiology, and Chronic Health Evaluation IV score (APACHE IV) of 60.5. Sixty patients (54.6%) required ventilation upon admission. Their median predicted mortality by APACHE IV was 14%. However, with the ability to provide a state of the art full-service intensive care, their short-term mortality (over 2 weeks) was only 6.4% (p=0.009).11
In conclusion, critical care service in KSA has the elements needed for success through its leadership support and manpower. In fact, the performance of many tertiary ICU’s scattered throughout the Kingdom parallels that of many similar units in industrialized countries. Kingdom of Saudi Arabia could form a professional national critical care organization through the SCCS that was needed to establish critical care practice standards throughout the kingdom.
Footnotes
Ethical Consent.
All manuscripts reporting the results of experimental investigations involving human subjects should include a statement confirming that informed consent was obtained from each subject or subject’s guardian, after receiving approval of the experimental protocol by a local human ethics committee, or institutional review board. When reporting experiments on animals, authors should indicate whether the institutional and national guide for the care and use of laboratory animals was followed.
References
- 1.Ministry of Health. General Directorate of Statistics & Information, Health statistic book. Riyadh (KSA): Ministry of Health; 2013. Accessed 10 March 2015; Updated 6 March 2013. Available from: http://www.moh.gov.sa/en/Ministry/Statistics/book/Documents/Statistics-Book-1434.pdf . [Google Scholar]
- 2.World Health Organization (WHO) Health systems: improving performance. Geneva (CH): 2000. Updated 2000; Accessed 10 March 2015. Available from: http://www.who.int/whr/2000/en/whr00_en.pdf . [Google Scholar]
- 3.Albejaidi F. Healthcare System in Saudi Arabia: An Analysis of Structure, Total Quality Management and Future Challenges. Journal of Alternative Perspectives in the Social Sciences. 2010;2:794–818. [Google Scholar]
- 4.Almalki M, Fitzgerald G, Clark M. Health care system in Saudi Arabia: an overview. East Mediterr Health J. 2011;17:784–793. doi: 10.26719/2011.17.10.784. [DOI] [PubMed] [Google Scholar]
- 5.Coopersmith CM, Wunsch H, Fink MP, Linde-Zwirble WT, Olsen KM, Sommers MS, et al. A comparison of critical care research funding and the financial burden of critical illness in the United States. Crit Care Med. 2012;40:1072–1079. doi: 10.1097/CCM.0b013e31823c8d03. [DOI] [PubMed] [Google Scholar]
- 6.Al-Dorzi HM, Naidu B, Khokhar S, White D, Arabi YM. Research experience, interest and perceived barriers of clinical staff working at the Intensive Care Department of a tertiary care academic hospital in Saudi Arabia. Middle East Journal of Anaesthesiology. 2013;22:301–307. [PubMed] [Google Scholar]
- 7.Arabi YM, Tamim HM, Rishu AH. Hypoglycemia with intensive insulin therapy in critically ill patients: predisposing factors and association with mortality. Crit Care Med. 2009;37:2536–2544. doi: 10.1097/CCM.0b013e3181a381ad. [DOI] [PubMed] [Google Scholar]
- 8.Arabi YM, Haddad SH, Tamim HM, Rishu AH, Sakkijha MH, Kahoul SH, et al. Near-target caloric intake in critically ill medical-surgical patients is associated with adverse outcomes. JPEN J Parenter Enteral Nutr. 2010;34:280–288. doi: 10.1177/0148607109353439. [DOI] [PubMed] [Google Scholar]
- 9.Arabi YM, Tamim HM, Dhar GS, Al-Dawood A, Al-Sultan M, Sakkijha MH, et al. Permissive underfeeding and intensive insulin therapy in critically ill patients: a randomized controlled trial. Am J Clin Nutr. 2011;93:569–577. doi: 10.3945/ajcn.110.005074. [DOI] [PubMed] [Google Scholar]
- 10.PROTECT Investigators for the Canadian Critical Care Trials Group and the Australian and New Zealand Intensive Care Society Clinical Trials Group, Cook D, Meade M, Guyatt G, Walter S, Heels-Ansdell D, et al. Dalteparin versus unfractionated heparin in critically ill patients. N Engl J Med. 2011;364:1305–1314. doi: 10.1056/NEJMoa1014475. [DOI] [PubMed] [Google Scholar]
- 11.Mandourah Y, Ocheltree A, Al Radi A, Fowler R. The epidemiology of Hajj-related critical illness: lessons for deployment of temporary critical care services*. Crit Care Med. 2012;40:829–834. doi: 10.1097/CCM.0b013e318236f49b. [DOI] [PubMed] [Google Scholar]