

Abstract
Introduction:
Oral health problems, especially dental caries are known to be common in children with severe heart disease, especially at early ages. The role of nitric oxide (NO) in protection against oral diseases owing to its strong antimicrobial action has been a topic of interest.
Objective:
The current study was carried out to estimate the NO levels in the salivary samples of children diagnosed with congenital heart diseases (CHDs) and to determine whether salivary NO can serve as a potential biomarker for the evaluation of dental caries-risk.
Methodology:
This prospective study was performed on 50 children suffering from CHDs who reported to the department of pediatrics and the levels were compared with those of 50 healthy caries-free children. NO levels in the collected salivary levels were determined spectrophotometrically using the Griess reaction method.
Results:
Subjects between the age group of 6 and 12 years had maximum decayed teeth (20.95%). The mean NO level in children in study group (60.63) was decreased in comparison to the control group (132.40), which was statistically significant (P value of 0.001). The mean age of the subjects in the study group was 7.24 and the salivary NO levels decreased with age, which was statistically significant.
Conclusion:
Children are suffering from medically compromising conditions such as CHDs are at a higher risk for dental caries and decreased salivary NO levels in these patients may prove as a critical indicator of the same. Saliva can be further utilized as an important biomarker for the determination of the relationship between salivary NO levels and development of dental caries.
Keywords: Congenital heart diseases, dental caries, salivary nitric oxide
INTRODUCTION
Heart disease is one of the most common developmental abnormalities among children, affecting approximately 6 per 1,000 live births.[1,2] Dental management of children with congenital heart disease (CHD) requires special attention, because of their increased susceptibility to infectious endocarditis, associated with bacteremia induced by invasive dental procedures. Oral health in these patients is not given due importance, and thus they often have poor oral health. These patients also have increased caries–risk, which may be largely attributed to the developmental enamel defects.[3,4,5]
There has been a mounting interest in the role of nitrates and nitrites in protection against oral diseases particularly dental caries in the last few years.[6,7] There is a constant supply of concentrated nitrates, the metabolic products of nitric oxide (NO) in the human oral cavity. It is generated either directly from the physiological reduction of dietary nitrates or it originates from L-arginine undergoing the reaction catalyzed by inducible NO synthase, which is an enzyme expressed in salivary glands and duct epithelial cells when induced by pro-inflammatory stimuli.[8,9,10,11]
Nitric oxide and its metabolic products, nitrates and nitrites, have been associated with various deleterious effects in humans in the past decades. However, the recent evidence has suggested that NO has a certain beneficial antimicrobial role in the oral cavity.[12] The interest in identifying caries-risk individuals through various salivary biomarkers among medically compromised children has also increased. Hence, the aim of the present study was to estimate the salivary NO levels in patients with CHDs.
Selection of subjects
Unstimulated saliva samples were collected from 100 children who were divided into two groups of 50 each. Study group consisted of cooperative children diagnosed with CHD in the age group of 4–14 years who reported to the Department of Paediatrics at Acharya Vinobha Bhave Rural Hospital, Wardha for the treatment of same. The control group included cooperative healthy caries free children in the age group of 4–14 years who reported to the Department of Pedodontics and Preventive Dentistry, Sharad Pawar Dental College, Wardha for routine dental check-up. Children who were un-cooperative, severely ill or having any other concomitant systemic or local diseases, which may affect the salivary secretion were excluded from the study.
METHODOLOGY
The study was carried out after taking the institutional ethical committee approval and informed written consent from parents of all the children who participated in the study. All the participants were asked to refrain from eating, drinking and tooth brushing 90 min before saliva collection. In order to eliminate the effect of the sympathetic tone, the participant in an upright position was asked to relax with no movement or talking. 1 ml of unstimulated saliva sample was collected and refrigerated. The dental caries status of all the participants was also recorded under natural daylight with the mouth mirror and explorer using the WHO oral health assessment criteria (1997).
Determination of nitric oxide concentration
The refrigerated saliva samples were coded before measuring the NO and decoded thereafter. NO was determined in saliva according to the method described by Miranda et al., 2001.[13]
Principle
This method determines the total nitrite/nitrate level based on the reduction reaction of any nitrate to nitrite by vanadium, followed by the detection of total nitrite (intrinsic + nitrite obtained from reduction of nitrate) by Griess reagent. The Griess reaction involves the formation of a pink colored chromophore from the diazotization of sulfanilamide by acidic nitrite, followed by coupling with bicyclic amines such as N-(1-naphthyl) ethylenediamine, which can be measured colorimetrically at 540 nm.
Procedure
In an eppendorf tube (Haimen Shengbang Laboratory Equipment Co., Ltd.), 0.75 ml cold absolute ethanol was added to 0.75 ml saliva. In order to attain complete protein precipitation, the mixture was left for 48 h in the refrigerator. It was then centrifugated at 4000 rpm at 12°C for 30 min using a cooling centrifuge. Only 250 μl of the obtained supernatant was used to which 250 μl vanadiumyrichloride was added, followed by rapid addition of 125 μl sulfanilamide (2% [w/v] in 5% HCl) and 125 μl of N-(1-naphthyl) ethylenediamine dihydrochloride (0.1% [w/v] in distilled water). The mixture was left at room temperature for 30 min after which the absorbance of the pink colored chromophore was measured at 540 nm using a double beam spectrophotometer against a blank treated in the same manner to the test but using 250 μl distilled water instead of the sample. The standard was treated exactly as the supernatant and measured against a blank reagent containing 250 μl distilled water.
Calculation of nitric oxide concentration (μMol/L)
The level of total nitrite/nitrate (NOx) in the saliva was calculated using the following formula:
NOx (μMol) = AT/As × n × DF.
where AT is the absorbance of the test sample; As is absorbance of the standard sample; n is the concentration of the standard and DF is the dilution factor = 1.5/0.75 = 2.
Statistical data analysis
Data were described in terms of range and mean ± standard deviation. Comparison of quantitative variables between different groups in the present study was done using Student's t-test. P < 0.05 was considered as statistically significant.
RESULTS
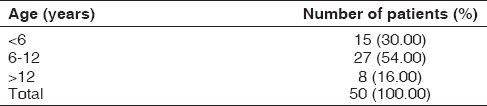
There were 15 children (30%) who were between 4 and 6 years of age, 27 children (54%) between 6 and 12 years and 8 children (16%) between 12 and 14 years of age [Table 1].
Table 1.
Age wise distribution of children in the study group
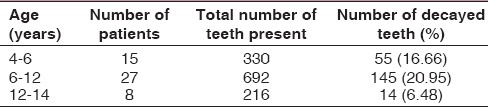
Children in the age group of 4–6 years had 55 decayed teeth (16.66%), children between 6 and 12 years had 145 decayed teeth (20.95%) and children between 12 and 14 years of age had 14 decayed teeth (6.48%) [Table 2].
Table 2.
Caries status of children in the study group
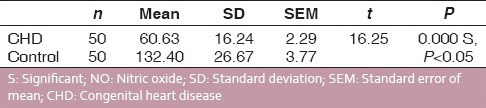
The mean NO levels obtained in the study group and the control group were 60.63 and 132.40 respectively shown graphically [Table 3 and Graph 1].
Table 3.
Comparison of NO level in children with CHD and control
Graph 1.
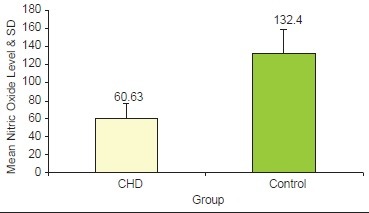
Mean salivary nitric oxide levels in the study group and control group
The correlation of mean age in years with the mean salivary NO levels in the study group (P value of 0.001) [Table 4 and Graph 2].
Table 4.
Correlation of age with respect to salivary NO levels

Graph 2.
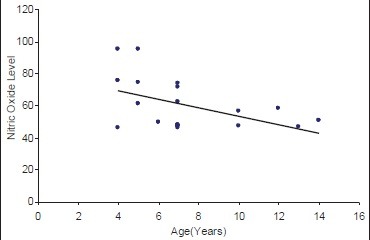
Correlation of age (years) with nitric oxide in congenital heart disease children
DISCUSSION
Dental caries is recognized as one of the most common infectious disease of the oral cavity. The general health and quality of life in these medically compromised children can be significantly affected due to untreated dental caries. The majority of studies conducted on children with heart disease patients of all ages have reported that the dental health of these subjects is usually poor.[14] Oral hygiene is often under looked by the parents of the children suffering from the CHD owing to the relatively more complex medical condition. Regular dental visits every 6–12 months starting at 2–3 years of age should be scheduled which is important for early identification of risk for dental caries in these children.[15] Improving oral health in this group of medically compromised children is a priority for which certain strategies should be developed. One of the major reasons to focus on caries prevention is the overall increased vulnerability of these children to stressful treatment procedures.
Saliva, a multiconstituent oral fluid, has high potential for the surveillance of general health and disease. The process of saliva collection is simple, noninvasive and has a high-sensitivity that has led to an emphasis on the promise of salivary biomarkers. Salivary biomarkers have proved more useful than serum analysis, for some diagnostic purposes.[16] Reasons behind the high caries prevalence in this group of children need to be explored which could be achieved by assessment of various salivary parameters.
Nitric oxide is known to have a highly reactive radical that has a strong antibacterial effect, which could play a protective role in the development of dental caries.[17] Thus, the present study was aimed to evaluate salivary NO as a biomarker of caries-risk in children with CHDs.
The children with mixed dentition (6–12 years) were found to have maximum carious teeth in the present study, that is, 145 out of 692 (20.95%) [Table 2]. Poor condition of primary teeth in children suffering from cardiac diseases could be related to the difficult situations that these children face during the 1st year of life.[18] Dasanayake et al. in 1995 stated that the use of antibiotics during early childhood is associated with higher mutans streptococci levels in children aged 5–12 years.[19] An increased intake of sweetened oral syrup drugs and poor oral hygiene also has been attributed to manifest carious lesions more in the primary and mixed than in permanent dentitions. It has been found in the previous studies that salivary NO levels are lower in the caries active individuals as compared to their caries free counterparts (Hegde Mitra et al., 2012).[17] Doel et al. in 2004 also found that children with high salivary nitrate levels had significantly less caries experience.
The study was aimed to estimate the NO levels in the saliva of children with CHDs. The mean NO level in children in study group was quite low in comparison to the control group [Graph 1] which was statistically significant. This can be directly related to the higher number of carious teeth found in the study group in comparison to healthy children. Thus it could be a risk factor for dental caries in these children apart from already mentioned above. The mean correlation of age with salivary NO levels in the diseased group was found to have significant results [Graph 2]. The mean NO levels in children with CHD decreased with age, which may be an implication of increase in the severity of the heart disease, number of hospitalizations and medications thus leading to poor dietary intake of NO. Hence from the present study, it can be proposed that measures should be taken to increase the salivary levels of NO for better protection against dental caries in children with CHDs. However, further long-term controlled studies need to be done to validate the relationship of salivary NO levels with age.
RECOMMENDATIONS
Nitrate in the diet which determines the high nitrate-reductase activity in the oral cavity could prove an important protective factor for dental caries especially in medically compromised children. Thus, dietary recommendations should include increased intake of nitrate rich foods such as green leafy vegetables, almonds, etc., A potential therapy against dental caries is providing probiotic therapy at an early age that can help for the colonization of anaerobic nitrate-reducing bacteria including Veillonella dispar and Veillonella atypica.[12]
CONCLUSION
There is an urgent need for improved caries prevention and an increased knowledge of the etiologic factors behind the oral health problems in children suffering from CHDs. Saliva is one of the important factors influencing the development of dental caries and salivary NO serves as a potential biomarker of caries-risk in medically compromised children.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Hoffman JI, Kaplan S. The incidence of congenital heart disease. J Am Coll Cardiol. 2002;39:1890–900. doi: 10.1016/s0735-1097(02)01886-7. [DOI] [PubMed] [Google Scholar]
- 2.Hoffman JI, Kaplan S, Liberthson RR. Prevalence of congenital heart disease. Am Heart J. 2004;147:425–39. doi: 10.1016/j.ahj.2003.05.003. [DOI] [PubMed] [Google Scholar]
- 3.Hallett KB, Radford DJ, Seow WK. Oral health of children with congenital cardiac diseases: A controlled study. Pediatr Dent. 1992;14:224–30. [PubMed] [Google Scholar]
- 4.Al-Sarheed M, Angeletou A, Ashley PF, Lucas VS, Whitehead B, Roberts GJ. An investigation of the oral status and reported oral care of children with heart and heart-lung transplants. Int J Paediatr Dent. 2000;10:298–305. doi: 10.1046/j.1365-263x.2000.00212.x. [DOI] [PubMed] [Google Scholar]
- 5.Da Silva DB, Souza IP, Cunha MC. Knowledge, attitudes and status of oral health in children at risk for infective endocarditis. Int J Paediatr Dent. 2002;12:124–31. doi: 10.1046/j.1365-263x.2002.00335.x. [DOI] [PubMed] [Google Scholar]
- 6.Duncan C, Li H, Dykhuizen R, Frazer R, Johnston P, MacKnight G, et al. Protection against oral and gastrointestinal diseases: Importance of dietary nitrate intake, oral nitrate reduction and enterosalivary nitrate circulation. Comp Biochem Physiol A Physiol. 1997;118:939–48. doi: 10.1016/s0300-9629(97)00023-6. [DOI] [PubMed] [Google Scholar]
- 7.Bayindir YZ, Polat MF, Seven N. Nitric oxide concentrations in saliva and dental plaque in relation to caries experience and oral hygiene. Caries Res. 2005;39:130–3. doi: 10.1159/000083158. [DOI] [PubMed] [Google Scholar]
- 8.Olin AC, Aldenbratt A, Ekman A, Ljungkvist G, Jungersten L, Alving K, et al. Increased nitric oxide in exhaled air after intake of a nitrate-rich meal. Respir Med. 2001;95:153–8. doi: 10.1053/rmed.2000.1010. [DOI] [PubMed] [Google Scholar]
- 9.Moncada S, Higgs A. The L-arginine-nitric oxide pathway. N Engl J Med. 1993;329:2002–12. doi: 10.1056/NEJM199312303292706. [DOI] [PubMed] [Google Scholar]
- 10.Green SJ. Nitric oxide in mucosal immunity. Nat Med. 1995;1:515–7. doi: 10.1038/nm0695-515. [DOI] [PubMed] [Google Scholar]
- 11.Soinila J, Nuorva K, Soinila S. Nitric oxide synthase in human salivary glands. Histochem Cell Biol. 2006;125:717–23. doi: 10.1007/s00418-005-0123-8. [DOI] [PubMed] [Google Scholar]
- 12.Doel JJ, Hector MP, Amirtham CV, Al-Anzan LA, Benjamin N, Allaker RP. Protective effect of salivary nitrate and microbial nitrate reductase activity against caries. Eur J Oral Sci. 2004;112:424–8. doi: 10.1111/j.1600-0722.2004.00153.x. [DOI] [PubMed] [Google Scholar]
- 13.Miranda KM, Espey MG, Wink DA. A rapid, simple spectrophotometric method for simultaneous detection of nitrate and nitrite. Nitric Oxide. 2001;5:62–71. doi: 10.1006/niox.2000.0319. [DOI] [PubMed] [Google Scholar]
- 14.Pimentel EL, Azevedo VM, Castro Rde A, Reis LC, De Lorenzo A. Caries experience in young children with congenital heart disease in a developing country. Braz Oral Res. 2013;27:103–8. doi: 10.1590/s1806-83242013000100016. [DOI] [PubMed] [Google Scholar]
- 15.Smith P. Primary care in children with congenital heart disease. J Pediatr Nurs. 2001;16:308–19. doi: 10.1053/jpdn.2001.26572. [DOI] [PubMed] [Google Scholar]
- 16.Streckfus C, Bigler L. The use of soluble, salivary c-erbB-2 for the detection and post-operative follow-up of breast cancer in women: The results of a five-year translational research study. Adv Dent Res. 2005;18:17–24. doi: 10.1177/154407370501800105. [DOI] [PubMed] [Google Scholar]
- 17.Surdilovic D, Stojanovic I, Apostolovic M, Igic M, Kostadinovic L. The role of nitric oxide in saliva in reduction of caries. Acta Fac Med Naissensis. 2004;25:93–5. [Google Scholar]
- 18.Talebi M, Khordi Mood M, Mahmoudi M, Alidad S. A study on oral health of children with cardiac diseases in Mashhad, Iran in 2004. J Dent Res Dent Clin Dent Prospects. 2007;1:114–8. doi: 10.5681/joddd.2007.020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Dasanayake AP, Roseman JM, Caufield PW, Butts JT. Distribution and determinants of mutans streptococci among African-American children and association with selected variables. Pediatr Dent. 1995;17:192–8. [PubMed] [Google Scholar]