

Abstract
Context:
Very recently, diode laser has been used for disinfecting the root canals in endodontic treatment and increasing its success rate and longevity utilizing the thermal effect of laser on surrounding tissues.
Aims:
The aim of this study is to evaluate the effect of 980 nm laser irradiation on intra-canal dentin surface – scanning electron microscopic (SEM) - in-vitro study.
Methods:
A total of 40 single-rooted freshly extracted permanent teeth were collected. Teeth were sectioned at the cemento-enamel junction using diamond disc. Root canals of all samples were prepared using hand ProTaper, which were randomly assigned into two groups (n = 20 each). Group 1: Receiving no treatment after biomechanical preparation; Group 2: 980 nm diode laser-treated root canals. Teeth were prepared for SEM analysis to check the size of intra-canal dentinal tubule openings.
Statistical Analysis Used:
Data were analyzed using SPSS V.16 software and compared using Levene's and independent t-test.
Results:
On statistical analysis, width of intracanal dentinal tubule openings in Group 1 (control) was significantly higher than those observed in Group 2 (diode laser-treated) (P < 0.001).
Conclusion:
This study showed that the application of 980 nm diode laser on intra-radicular dentin resulted in ultrastructural alterations resulting in melting of dentin.
Keywords: 980 nm diode laser, intra-canal dentinal tubules, intra-radicular, ProTaper, scanning electron microscopic, ultrastructural
INTRODUCTION
Success of a root canal treatment mainly depends on the disinfection and adequate seal of the root canal system.[1,2,3] Disinfection is achieved by removing the persisting micro-organisms and infected organic and inorganic debris. Proper apical seal prevents microleakage and subsequent re-infection.[1,2,3]
While doing biomechanical preparation, during canal instrumentation, fine dentinal debris gets deposited over the intra-canal dentin surface in the form of smear layer and obliterates the dentinal tubule openings.[4] Smear layer consists of inorganic dentin, necrosed organic debris, bacteria and their byproducts.[4] It can harbor micro-organisms, which may reach deep into the dentinal tubules and hinders in disinfection procedure by limiting the entry of dis-infective agents.[4] It also prevents the contact between the dentin surface and filling material, resulting in microleakage rendering it vulnerable to reinfection.[4] Thus, removal of smear layer is an important step in achieving adequate seal and prevention of microleakage for successful root canal treatment.
Various chemicals used for smear layer removal in endodontics are chelating agents like Ethylenediaminetetraacetic acid (EDTA),[5,6,7] sodium hypochlorite,[6] organic acids like citric acid and phosphoric acid,[8,9] combination of sodium hypochlorite and EDTA.[10,11] These irrigating solutions have limited efficacy because of inadequate penetration ability into the dentinal tubules and insufficient potential in removing micro-organism due to the complex root canal system.[12]
Newer techniques are thus explored for disinfection of root canal without causing damage to healthy tissues. The use of lasers in endodontic therapy appears to be a promising adjunct to the conventional root canal therapy.[13] One of the laser that has gained popularity in endodontics is diode laser due to its ability to effectively remove smear layer and Disinfecting even the lateral and accessory canals.[13] Diode lasers are available in four different wavelengths of 810–830 nm, 940 nm, 980 nm, 1064 nm.[14] The antibacterial quality of diode lasers is attributed to the thermal effect and rise in temperature occurring inside the root canals on irradiation.[14] Their effects vary on modifying the time of exposure, power and wavelength of radiation used.[14] To the best of our knowledge, no study has been reported in the literature which quantifies the diameter of dentinal tubule openings after irradiation with diode lasers.
Therefore, the purpose of this study was to evaluate and to quantify the effect of 980 nm diode laser irradiation on intra-canal dentin surface and dentinal tubule openings and also its ability to remove smear layer after Biomechanical preparation.
METHODS
The study was conducted in the Department of Pedodontics and Preventive dentistry, I.T.S- CDSR, Muradnagar and the ethical clearance was taken for conducting the study. Forty freshly extracted intact human single-rooted and caries-free teeth were selected for the purpose of the study. Intra-oral peri-apical radiographs were taken to ensure for any morphological defects in pulp chamber and root canal. Teeth were then autoclaved according to occupational safety and health administration guidelines and were sectioned at the cemento-enamel junction with diamond sectioning disc. Each root was mounted on a wax block. Specimens were randomly divided into two groups containing 20 samples each.
Group 1 (control)
Apical preparation was done till 20 number K-file, following which roots were prepared with ProTaper files (Dentsply, Switzerland) till F2 file using RC Prep along with sodium hypochlorite solution (5.25%) irrigation, followed by final flush by 17% EDTA solution.
Group 2 (980 nm diode laser irradiated)
Apical preparation was done till 20 number K-file, following which roots were prepared with ProTaper files (Dentsply, Switzerland) till F2 file using RC Prep along with sodium hypochlorite solution (5.25%) irrigation, followed by final flush by 17% EDTA solution. Specimens were then irradiated by Zolar diode lasers with 980 nm wavelength, 2 watt power, and 200 μm fiber size. Root canals were irradiated by introducing the fiber-optic cable along the entire length of the root canal irradiating all the dentinal walls from apical to the cervical region in helical movements at the speed of 1 mm/s. The procedure was repeated 4 times. Specimens were kept at room temperature for 20 s in between each irradiation to prevent temperature rise from exceeding the accepted allowance.
Scanning electron microscopy analysis
Roots of both the groups were then hemi-sectioned in the bucco-lingual direction and were then stored in ethanol (100%). The intracanal dentin surface of all the specimens of both the groups were subjected to gold spluttering in the gold spluttering chamber. The specimens were then mounted in the vacuum chamber of SEM and viewed under ×5000 magnification. Micrographs of the intra-canal dentin surface were taken randomly at any point. Following that, ten dentinal tubule openings were randomly selected per micrograph and maximum width of dentinal tubule openings were recorded for all the samples.
Statistics analysis
Data were analyzed on SPSS V.16 statistical software (SPSS Inc., Chicago). Test of homogeneity of data was tested by Levene's test. Width of intracanal dentinal tubule openings was compared using t-test for two independent groups (Group 1 and 2).
RESULTS
Scanning electron microcopic analysis of intracanal dentin surface
On SEM, analysis, micrographs of intra-canal dentin surface of Group 1 [Figure 1] showed open dentinal tubules and partial presence of smear layer. Mean width of dentinal tubule openings on intacanal dentin surface for Group 1 was calculated to be 2.4701 ± 0.302 μm. Micrographs of Group 2 [Figure 2] showed partial to nearly completely obliterated dentinal tubules openings and melting of inter-tubular dentin on intracanal dentin surface making it smooth with absence of smear layer. In contrast to Group 1, mean width of dentinal tubule openings on intracanal dentin surface in Group 2 was 0.1975 ± 0.136 μm [Figure 3].
Figure 1.
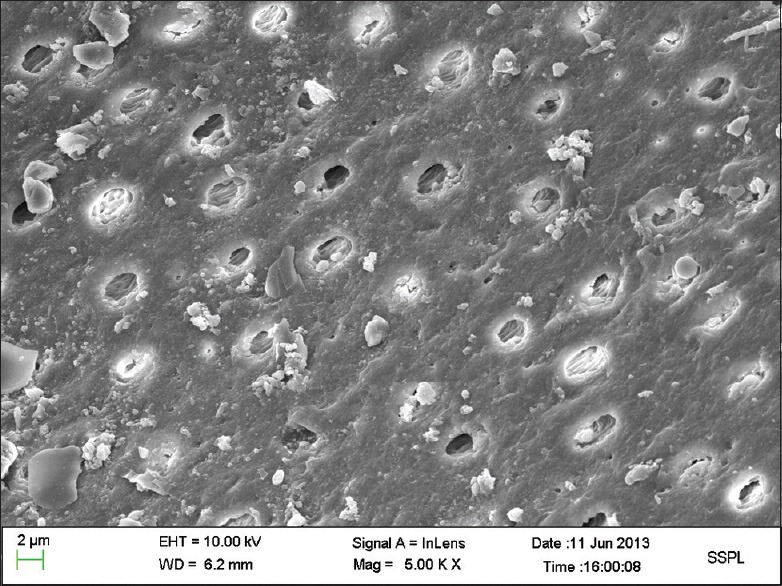
Scanning electron micrograph of intracanal root dentin surface for Group 1 (postbiomechanical preparation with irrigants)
Figure 2.
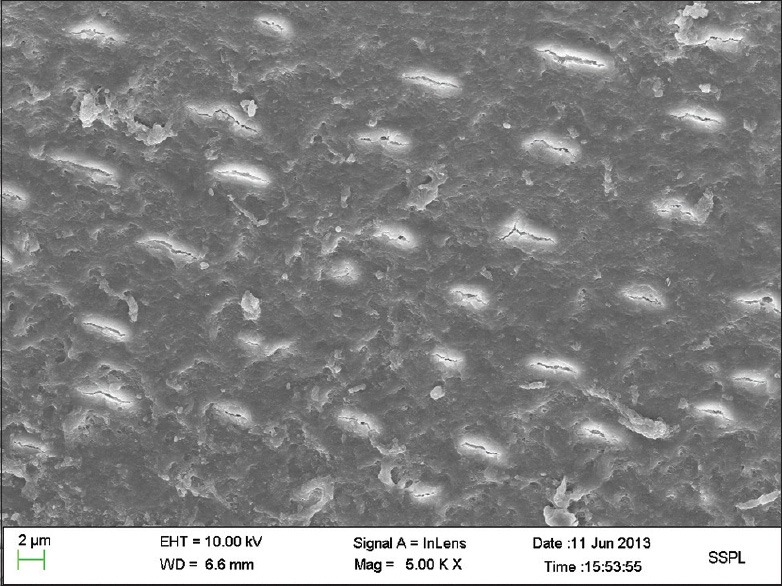
Scanning electron micrographs of intracanal root dentin surface for Group 2 (980 nm diode laser irradiated root canal after biomechanical preparation)
Figure 3.
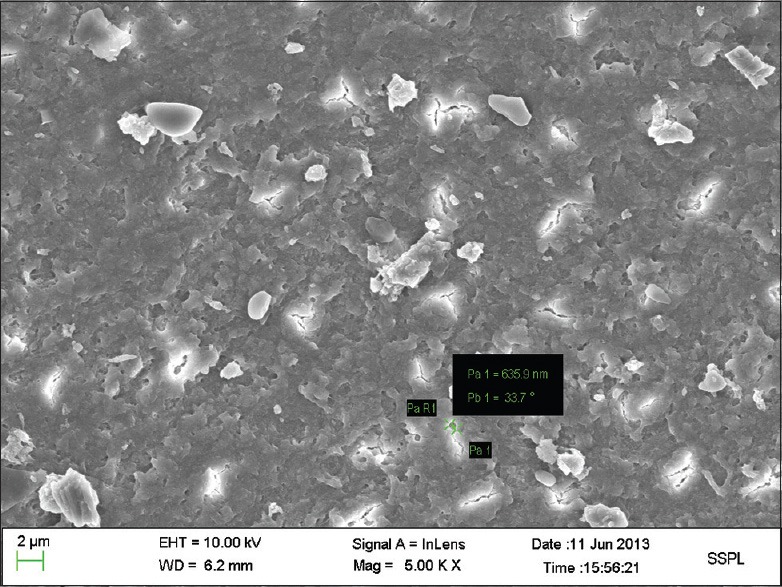
Scanning electron micrograph showing width of one intracanal dentinal tubule opening for Group 2 (980 nm diode laser irradiated root canal after biomechanical preparation)
Result of statistical analysis
The distribution of means ± standard deviation of intracanal dentinal tubule openings of Group 1 was 2.4701 ± 0.302 μm and Group 2 was 0.1975 ± 0.136 μm [Figure 4]. By Levene's test it was found that the data was normally distributed. On applying t-test for two independent groups, the mean difference of width of intracanal dentinal tubule openings (−2.2726400 μm) was highly significant (P < 0.001). The lower bound and upper bound of this mean difference at 95% confidence were −2.3188332 and −2.22.64468 respectively [Tables 1 and 2].
Figure 4.

Graph showing mean width of intracanal dentinal tubule openings in the two groups in μm Group 1 (control) and Group 2 (980 nm diode laser irradiated root canals)
Table 1.
The distribution of mean±SD of width of intracanal dentinal tubule openings in Group 1 and Group 2 in μm

Table 2.
Difference in the mean width of intracanal dentinal tubule openings in Group 1 and Group 2 in μm is highly significant (P<0.001)

DISCUSSION
Root canal system is a complex system comprising of many accessory canals branching out from the main root canal. The complexity of the root canal system poses a difficulty in its complete debridement.[15] Several irrigants have been used in the literature with the aim of complete removal of debris and elimination of micro-organisms from the root canal system, but due to the torturous branching network of the root canal system, complete disinfection from the dentinal tubules have not been successfully achieved alone with use of irrigants.[16]
With the advancement in technology, lasers have made their way into dentistry. Out of the numerous uses, an important one is their use as an adjunct to root canal therapy due to their disinfecting potential reaching even up to lateral canals.[17] This property of disinfection is due to the thermal effects causing increase in temperature in the root canal system thus killing bacteria even in lateral canals.[18,19] Various types of lasers have been used for root canal disinfection namely, carbon dioxide lasers,[20] neodymium-doped:yttrium aluminium garnet,[21] erbium group of lasers[21,22,23] and diode lasers.[13]
Diode lasers have recently gained popularity because of their ease of use, versatility, compactness allowing easy mobility, and less cost of the machine as compared to other lasers. One of the qualities of diode lasers which ensures a successful endodontic treatment is its antibacterial ability causing disinfection of root canal system.[13,24]
Another important quality of diode lasers is their ability to remove the smear layer and melting of the intra-canal dentin surface.[25] Cameron and Mader et al. studied the smear layer as two components being superficial smear layer and debris clogged in the dentinal tubules which extended up to 40 mm into the dentinal tubules.[26,27] Cengiz et al. suggested that packing of smear debris into the dentinal tubules occurs by capillary action due to adhesive forces between tubules and debris. Smear layer acts as a physical barrier to penetration of medicaments and irrigants into the dentinal tubules.[28]
The present study demonstrated excellent removal of smear layer and dentinal debris from the root canal surfaces after treatment with diode laser [Figure 2], whereas in the control group dentinal surface was covered with smear layer [Figure 1]. Another very important observation seen is diode laser caused morphological effects on the intra-canal dentin and dentinal tubule openings causing melting of intracanal dentin and partial to complete obliteration of dentinal tubules. This was in accordance with the results reported by Saghiri et al.[29] and Alfredo et al.[30] It has been proposed that photo-ablative effects of laser causes fusion and re-solidification of dentin and thus reduce dentin permeability.
Studies done by various authors on microleakage and sealing ability on root canals irradiated by diode lasers show less microleakage and good seal.[31,32] Faria et al. investigated effect of 980 nm diode laser on intra-radicular dentin morphology and apical microleakage after obturation of canals and found the change in dentin morphology, which intensified on increasing the power.[33]
In the present study, we attempted to quantify the size of dentinal tubule openings on intra-canal dentin surface. In the present study, SEM was used to observe the difference in the size of the dentinal tubule openings on the intracanal dentin surface. The results showed a marked difference in size of the openings between the two groups. The mean width of the dentinal tubule opening in Group 1 was 2.4701 μm, whereas; mean width in Group 2 (diode laser irradiated) was 0.1975 μm [Tables 1 and 2][Figure 4]. The diameter of most micro-organisms present in the root canal system ranges from 0.2 to 0.7 μm.[34] The present study showed that the maximum width of dentinal tubule of the laser irradiated group was less than the diameter of the micro-organism species present in oral cavity thus making it difficult for them to pass through the opening consequently reducing the possibility of re-infection.
It can be concluded from the present study that diode laser causes partial to complete obliteration of the dentinal tubules in the intra-canal system, leading to a sterile environment and reducing the chances of re-infection thus increasing the success rate of the root canal treatment if used as an adjunct to the conventional root canal therapy.
The advantages of diode lasers are many if used with proper specifications mentioned by the manufacturer. However, lasers also have the potential to cause harmful hazards. Further clinical research is required to determine optimal power and exposure time specifications of diode lasers to achieve maximum benefit on intra-canal dentin and least risk to surrounding tissues.
CONCLUSION
It can be concluded that 980 nm diode laser (2 watt power, and 200 μm fiber size) causes melting of intra-canal dentin and partial to complete obliteration of the dentinal tubule openings if the intra-canal dentin is irradiated for four cycles in helical movements at the speed of 1 mm/s. Thus to increase the success rate of the root canal treatment and prevent reinfection, use of diode lasers can be recommended as an adjunct to conventional root canal treatment as it would limit the re-entry of microflora into the root canal system.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Cobankara FK, Adanir N, Belli S, Pashley DH. A quantitative evaluation of apical leakage of four root-canal sealers. Int Endod J. 2002;35:979–84. doi: 10.1046/j.1365-2591.2002.00577.x. [DOI] [PubMed] [Google Scholar]
- 2.Vivan RR, Bortolo MV, Duarte MA, Moraes IG, Tanomaru-Filho M, Bramante CM. Scanning electron microscopy analysis of RinsEndo system and conventional irrigation for debris removal. Braz Dent J. 2010;21:305–9. doi: 10.1590/s0103-64402010000400003. [DOI] [PubMed] [Google Scholar]
- 3.Karagöz-Küçükay I, Bayirli G. An apical leakage study in the presence and absence of the smear layer. Int Endod J. 1994;27:87–93. doi: 10.1111/j.1365-2591.1994.tb00236.x. [DOI] [PubMed] [Google Scholar]
- 4.Violich DR, Chandler NP. The smear layer in endodontics – A review. Int Endod J. 2010;43:2–15. doi: 10.1111/j.1365-2591.2009.01627.x. [DOI] [PubMed] [Google Scholar]
- 5.Gouveia MA, Carvalho MF, Paulo M. Smear layer in endodontics: A bibliographic review. Endodoncia. 2002;20:100–8. [Google Scholar]
- 6.Hülsmann M, Heckendorff M, Schäfers F. Comparative in-vitro evaluation of three chelator pastes. Int Endod J. 2002;35:668–79. doi: 10.1046/j.1365-2591.2002.00543.x. [DOI] [PubMed] [Google Scholar]
- 7.Hülsmann M, Heckendorff M, Lennon A. Chelating agents in root canal treatment: Mode of action and indications for their use. Int Endod J. 2003;36:810–30. doi: 10.1111/j.1365-2591.2003.00754.x. [DOI] [PubMed] [Google Scholar]
- 8.Sceiza MF, Daniel RL, Santos EM, Jaeger MM. Cytotoxic effects of 10% citric acid and EDTA-T used as root canal irrigants: An in vitro analysis. J Endod. 2001;27:741–3. doi: 10.1097/00004770-200112000-00007. [DOI] [PubMed] [Google Scholar]
- 9.Scelza MF, Teixeira AM, Scelza P. Decalcifying effect of EDTA-T, 10% citric acid, and 17% EDTA on root canal dentin. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2003;95:234–6. doi: 10.1067/moe.2003.89. [DOI] [PubMed] [Google Scholar]
- 10.Braguetto CA, Souza-Neto MP, Cruz-Filho AM, Gariba Silva R, Saqui PC, Pécora JD. Action of the solution of EDTA and Dakin's solution used alone or mixed alternating in cleaning the root canal. Rev Odontol Univ São Paulo. 1997;1:67–70. [Google Scholar]
- 11.Sen BH, Wesselink PR, Türkün M. The smear layer: A phenomenon in root canal therapy. Int Endod J. 1995;28:141–8. doi: 10.1111/j.1365-2591.1995.tb00289.x. [DOI] [PubMed] [Google Scholar]
- 12.Sjogren U, Hagglund B, Sundqvist G, Wing K. Factors affecting the long-term results of endodontic treatment. J Endod. 1990;16:498–504. doi: 10.1016/S0099-2399(07)80180-4. [DOI] [PubMed] [Google Scholar]
- 13.Kaiwar A, Usha HL, Meena N, Ashwini P, Murthy CS. The efficiency of root canal disinfection using a diode laser: In vitro study. Indian J Dent Res. 2013;24:14–8. doi: 10.4103/0970-9290.114916. [DOI] [PubMed] [Google Scholar]
- 14.Miserendino L, Robert PM. Hanover Park, IL: Quintessence Publishing; 1995. Lasers in Dentistry. [Google Scholar]
- 15.Cohen S, Burns RC. 7th ed. Missouri: Mosby; 1998. Pathways of the Pulp; p. 150. [Google Scholar]
- 16.Goodis HE, White JM, Marshall SJ, Marshall GW., Jr Scanning electron microscopic examination of intracanal wall dentin: Hand versus laser treatment. Scanning Microsc. 1993;7:979–87. [PubMed] [Google Scholar]
- 17.Rooney J, Midda M, Leeming J. A laboratory investigation of the bactericidal effect of a NdYAG laser. Br Dent J. 1994;176:61–4. doi: 10.1038/sj.bdj.4808364. [DOI] [PubMed] [Google Scholar]
- 18.de Souza EB, de Amorim CV, Marques JL. Effect of diode laser irradiation on the apical sealing of MTA retrofillings. Braz Oral Res. 2006;20:231–4. doi: 10.1590/s1806-83242006000300009. [DOI] [PubMed] [Google Scholar]
- 19.Moritz A, Gutknecht N, Goharkhay K, Schoop U, Wernisch J, Sperr W. In vitro irradiation of infected root canals with a diode laser: Results of microbiologic, infrared spectrometric, and stain penetration examinations. Quintessence Int. 1997;28:205–9. [PubMed] [Google Scholar]
- 20.Le Goff A, Dautel-Morazin A, Guigand M, Vulcain JM, Bonnaure-Mallet M. An evaluation of the CO2 laser for endodontic disinfection. J Endod. 1999;25:105–8. doi: 10.1016/S0099-2399(99)80006-5. [DOI] [PubMed] [Google Scholar]
- 21.Moritz A, Schoop U, Goharkhay K, Jakolitsch S, Kluger W, Wernisch J, et al. The bactericidal effect of Nd: YAG, Ho: YAG, and Er: YAG laser irradiation in the root canal: An in vitro comparison. J Clin Laser Med Surg. 1999;17:161–4. doi: 10.1089/clm.1999.17.161. [DOI] [PubMed] [Google Scholar]
- 22.Dos Santos Antonio MP, Moura-Netto C, Camargo SE, Davidowicz H, Marques MM, Maranhão de Moura AA. Bactericidal effects of two parameters of Er: YAG laser intracanal irradiation: Ex-vivo study. Lasers Med Sci. 2012;27:1165–8. doi: 10.1007/s10103-011-1023-x. [DOI] [PubMed] [Google Scholar]
- 23.Schoop U, Goharkhay K, Klimscha J, Zagler M, Wernisch J, Georgopoulos A, et al. The use of the erbium, chromium: yttrium-scandium-gallium-garnet laser in endodontic treatment: The results of an in vitro study. J Am Dent Assoc. 2007;138:949–55. doi: 10.14219/jada.archive.2007.0291. [DOI] [PubMed] [Google Scholar]
- 24.Moritz A, Doertbudak O, Gutknecht N, Goharkhay K, Schoop U, Sperr W. Nd: YAG laser irradiation of infected root canals in combination with microbiological examinations. J Am Dent Assoc. 1997;128:1525–30. doi: 10.14219/jada.archive.1997.0092. [DOI] [PubMed] [Google Scholar]
- 25.Marchesan MA, Brugnera-Junior A, Souza-Gabriel AE, Correa-Silva SR, Sousa-Neto MD. Ultrastructural analysis of root canal dentine irradiated with 980-nm diode laser energy at different parameters. Photomed Laser Surg. 2008;26:235–40. doi: 10.1089/pho.2007.2136. [DOI] [PubMed] [Google Scholar]
- 26.Cameron JA. The use of ultrasonics in the removal of the smear layer: A scanning electron microscope study. J Endod. 1983;9:289–92. doi: 10.1016/S0099-2399(83)80119-8. [DOI] [PubMed] [Google Scholar]
- 27.Mader CL, Baumgartner JC, Peters DD. Scanning electron microscopic investigation of the smeared layer on root canal walls. J Endod. 1984;10:477–83. doi: 10.1016/S0099-2399(84)80204-6. [DOI] [PubMed] [Google Scholar]
- 28.Cengiz T, Aktener BO, Piskin B. Effect of dentinal tubule orientation on the removal of smear layer by root canal irrigants. A scanning electron microscopic study. Int Endod J. 1990;23:163–71. doi: 10.1111/j.1365-2591.1990.tb00094.x. [DOI] [PubMed] [Google Scholar]
- 29.Saghiri MA, Asgar K, Gutmann JL, Garcia-Godoy F, Ahmadi K, Karamifar K, et al. Effect of laser irradiation on root canal walls after final irrigation with 17% EDTA or BioPure MTAD: X-ray diffraction and SEM analysis. Quintessence Int. 2012;43:e127–34. [PubMed] [Google Scholar]
- 30.Alfredo E, Souza-Gabriel AE, Silva SR, Sousa-Neto MD, Brugnera-Junior A, Silva-Sousa YT. Morphological alterations of radicular dentine pretreated with different irrigating solutions and irradiated with 980-nm diode laser. Microsc Res Tech. 2009;72:22–7. doi: 10.1002/jemt.20638. [DOI] [PubMed] [Google Scholar]
- 31.Das M, Kumar GA, Ramesh S, Garapati S, Sharma D. An in vitro evaluation of microtensile bond strength of resin-based sealer with dentin treated with diode and Nd: YAG laser. J Contemp Dent Pract. 2013;14:183–7. doi: 10.5005/jp-journals-10024-1297. [DOI] [PubMed] [Google Scholar]
- 32.Moura-Netto C, Palo RM, Camargo SE, Jent C, Leonardo Rde T, Marques MM. Influence of prior 810-nm-diode intracanal laser irradiation on hydrophilic resin-based sealer obturation. Braz Oral Res. 2012;26:323–9. doi: 10.1590/s1806-83242012005000010. [DOI] [PubMed] [Google Scholar]
- 33.Faria MI, Souza-Gabriel AE, Alfredo E, Messias DC, Silva-Sousa YT. Apical microleakage and SEM analysis of dentin surface after 980 nm diode laser irradiation. Braz Dent J. 2011;22:382–7. doi: 10.1590/s0103-64402011000500006. [DOI] [PubMed] [Google Scholar]
- 34.Hargreaves KM, Cohen S. 10th ed. Missouri: Elsevier, Mosby; 2011. Cohen's Pathways of the Pulp; p. 560. [Google Scholar]